
Abstract
Background:
Medication-related osteonecrosis of the jaw (MRONJ) is a severe adverse medication response that manifests as progressive bone necrosis in the craniofacial area. There is still no clear treatment protocol for the management of MRONJ. The purpose of this study was to conduct a systematic review to assess the efficacy of photobiomodulation (PBM) as an adjunct to MRONJ therapy.
Methods:
In line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement, a literature search was performed on PubMed/MEDLINE, Scopus, Web of Science, and Cochrane databases. Two examiners examined eligibility and risk of bias separately before extracting data.
Results:
Two hundred sixty-nine articles were found through electronic search, out of which only 11 met the inclusion criteria and were included in qualitative synthesis (9 retrospectives, 1 prospective, and 1 case series). A total number of 759 patients and a mean age ranging from 54 to 74 years were reviewed. Females were the most frequent gender in all of the selected studies (72% females to 28% males), and the most frequent stage in the studies mentioned above was stage II (66%). Most of the studies had shown a significant improvement when PBM was used as an adjunctive treatment.
Conclusions:
Based on the results of this study, PBM as an adjuvant therapy can significantly improve the outcomes of each treatment plan. However, surgical intervention for the complete healing of the lesions is suggested.
Introduction
Osteonecrosis of the jaws (ONJ) is an adverse side effect of several therapies, in particular, nitrogen-containing bisphosphonates initially described in 2003 by Ruggiero, Migliorati, and Marx in patients receiving pamidronic acid or zoledronic acid. 1 –3 In June 2014, the Special Committee of the American Association of Oral and Maxillofacial Surgeons (AAOMS) recommended a changing of the nomenclature of Bisphosphonate-Related Osteonecrosis of the Jaw (BRONJ) in Medication-Related Osteonecrosis of the Jaw (MRONJ). 4 This decision was taken to accommodate the growing number of osteonecrosis associated with other drugs than bisphosphonates (BPs), such as antiresorptive (denosumab) and antiangiogenic therapies (tyrosine kinase inhibitors: sunitinib/sorafenib), monoclonal antibodies targeting Vascular Epithelial Growth Factor (VEGF) such as bevacizumab. These therapies are used to prevent or manage bone resorption in patients with multiple myeloma, bone lytic metastasis, and metabolic bone diseases such as osteoporosis or Paget's disease. 4
Extreme pain, pus discharge, nonhealing exposed bone sites, halitosis, ulceration, swelling of adjacent soft tissues, fistulas, and increased bone fracture risk are common symptoms of MRONJ. 5 On radiographs, osteonecrosis exists as an irregular region of osteosclerosis with a cotton-wool pattern, and osteolysis appears as a central part of the separated bone (sequestrum). 6 According to the AAOMS position paper in 2014, all three of the following criteria must be present at the same time for MRONJ to be diagnosed: 4 “1. Current or previous treatment with antiresorptive or antiangiogenic agents; 2. Exposed bone or bone that can be probed through an intraoral or extraoral fistula(e) in the maxillofacial region that has persisted for more than eight weeks; and 3. No history of radiation therapy to the jaws or obvious metastatic disease to the jaws.”
The classification suggested by AAOMS is as follows 4 : stage I (no symptomatic lesions with bone exposure in the lack of infection symptoms); stage II (bone exposure with pain, infection, and swelling); and stage III (bone exposure with discomfort, infection, secondary infections, cutaneous fistulas, and pathological fractures). While antiresorptive and anti-angiogenic therapies help patients with neoplastic diseases survive longer, they may also negatively impact their quality of life. 7 Patients report difficulty swallowing and speaking, bleeding, and lower lip paresthesia where the necrosis is severe and adjacent to the mandibular branch of the trigeminal nerve. 6
Although the precise MRONJ pathophysiology is unclear, 8 it is undoubtedly caused by a combination of several factors. The potential mechanisms of MRONJ development include altered bone remodeling or oversuppression of bone resorption, angiogenesis inhibition, immunosuppression, vitamin D deficiency, and soft tissue toxicity. It is also essential to consider the role of trauma, inflammation, and bacterial infection connected to the peculiar anatomical site. 9 Soft tissue toxicity is produced by the impact of BPs on the survival, migration, and apoptosis of oral keratinocytes and fibroblasts, resulting in an impairment of routine soft tissue healing near postextraction or local prosthetic injuries. 10
MRONJ prevalence in osteoporosis patients prescribed antiresorptive drugs is reported to be between 0.001% and 0.01%. 11 Females have a higher incidence of this complication, which has been explained due to underlying diseases such as osteoporosis and breast cancer. In a study of more than 13,000 Kaiser Permanente participants, the incidence of MRONJ in patients receiving long-term oral BP therapy was found to be 0.1% (10 cases per 10,000), increasing to 0.21% (21 cases per 10,000) in patients with more than 4 years of oral BP exposure. 12
When oral BPs are used for more than 4 years, the chance of MRONJ rises. 12 Furthermore, ONJ is more common in people treated with high-dose BPs than in those administered low-dose intravenous or oral BPs, with prevalence ranging from 0% to 0.348%, with the majority under 0.005%. 11 The lesions are more common in sites with thinner mucosa overlying bone prominences, such as tori, exostoses, and the mylohyoid ridge. 11 MRONJ may involve the maxilla, mandible, or both; However, the mandible is more frequently affected due to its mainly cortical nature, and yet, these lesions are more challenging to manage. 13 Also, lesions' size may differ, ranging from a nonhealing extraction site to broad parts of the mandible or maxilla exposed and necrosed. 14
MRONJ's management is also a source of debate. Enhancement of oral hygiene, regular dental examinations, oral washes with chlorhexidine, photobiomodulation (PBM) therapy, and antibiotic therapy are all nonsurgical treatments for MRONJ, which surgical approaches, including laser (light amplification by stimulated emission of radiation)-assisted surgery, may follow in advanced cases for reduction of necrotic bone tissues. 15 Recently, PBM therapy has been used as adjuvant therapy for treating MRONJ in recent years due to its good analgesia, potential to minimize edema development, and cell biomodulation, promoting wound healing. 16 However, the exact mechanism of PBM therapy has not yet been fully understood. At appropriate physical parameters, PBM therapy promotes the production of reactive species capable of causing bacterial death through necrosis or apoptosis while preserving the surrounding tissue. 17
PBM boosts the reparative mechanism by increasing the inorganic matrix of bone and mitotic osteoblastic index and the motility and expression of collagen type I and VEGF genes in human keratinocytes (+minamisako). 18 Irradiation results in enhanced energy potential cells, and the main reactions take place at the mitochondrial stage, particularly in the electron transport chain; other responses, including signal transduction to the cytoplasm, enhance cell proliferation and differentiation. 19 Mesenchymal stem cell proliferation is essential as they downregulate the inflammatory cells to cessate proinflammatory activity and induce the regeneration of normal tissue. 20 The extensive paracrine activity of mesenchymal stem cells, which includes the generation of cytokines and chemokines, mitochondrial translocation, and extracellular vesicle secretion, has been well proved. 21 PBM is distinct from other light-based therapies since it does not ablate and does not use heat.
The procedure yields no noticeable temperature increase in the treated tissue and, as a result, no noticeable difference in the gross tissue structure due to the low power, which usually is less than 500 mW varying on the target tissue. 22
Based on PBM's various promising characteristics, the present systematic review aims to discover the efficacy of PBM in the treatment of MRONJ.
Methods
Focus question
This systematic review of available literature was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and registered in PROSPERO: CRD42021252773.
The purpose of this review was to answer the following focus question: “Does PBM have positive effects in the treatment of MRONJ?”
The participant, Intervention, comparison, and outcome question was established as follows: (1) Participants: Patients with MRONJ; (2) Intervention: PBM; (3) Comparisons: therapies other than PBM; and (4) Outcome: improvement or total healing of MRONJ lesions
Search strategy
An electronic search of the literature using PubMed, Scopus, Web of Science, and Cochrane library was performed. The PubMed search strategy used a combination of MeSH terms and other keywords connected by Boolean operators as described below: ((“Medication-related osteonecrosis”[tiab] AND (jaw[tiab] OR mandible[tiab] OR maxilla[tiab]))OR mronj[tiab] OR BRONJ[tiab] OR (“Bisphosphonate-related osteonecrosis”[tiab] AND (jaw[tiab] OR mandible[tiab] OR maxilla[tiab])) OR (“Bisphosphonate-associated osteonecrosis“[tiab] AND (jaw[tiab] OR mandible[tiab] OR maxilla[tiab])) OR “jaw osteonecrosis”[tiab] OR (osteonecros*[tiab] AND (jaw[tiab] OR mandible[tiab] OR maxilla[tiab])) OR “Bisphosphonate-Associated Osteonecrosis of the Jaw”[Mesh]) AND ((“laser Biostimulation”[tiab] OR “Low Level Laser Therapy”[tiab] OR “low-level laser treatment”[tiab] OR “soft laser”[tiab] OR “low intensity laser”[tiab] OR “low output laser” OR Phototherapy[tiab] OR “Low Power Laser Irradiation”[tiab] OR “low-power laser therapy”[tiab] OR “low-power laser treatment” OR Photobiomodulation[tiab] OR lllt[tiab] OR “low level light therapy”[tiab] OR “therapeutic laser” OR “low level light therapy”[Mesh]))
An additional search was undertaken through Web of Science and Scopus using the following search strategy: (TS = ((“Medication-related osteonecrosis” OR “Bisphosphonate-related osteonecrosis” OR “Bisphosphonate-associated osteonecrosis “OR osteonecros*) AND (jaw OR mandible OR maxilla)) OR TS = (BRONJ OR MRONJ OR “jaw osteonecrosis”)) AND TS = (“laser Biostimulation” OR “Low Level Laser Therapy” OR “low-level laser treatment” OR “soft laser” OR “low intensity laser” OR “low output laser” OR Phototherapy OR “Low Power Laser Irradiation” OR “low-power laser therapy” OR “low-power laser treatment” OR Photobiomodulation OR lllt OR “low level light therapy”)
A further search was conducted using the Cochrane Library with the following search strategy: (“laser Biostimulation” OR “Low Level Laser Therapy” OR “low-level laser treatment” OR “soft laser” OR “low intensity laser” OR “low output laser” OR Phototherapy OR “Low Power Laser Irradiation” OR “low-power laser therapy” OR “low-power laser treatment” OR Photobiomodulation OR lllt OR “low level light therapy”) in Title Abstract Keyword AND ((“Medication-related osteonecrosis” OR “Bisphosphonate-related osteonecrosis” OR “Bisphosphonate-associated osteonecrosis “OR osteonecros*) AND (jaw OR mandible OR maxilla)) OR (BRONJ OR MRONJ OR “jaw osteonecrosis”) in Title Abstract Keyword - (Word variations have been searched)
At last, a manual search of references of the retained articles was conducted to identify any further studies that the electronic search had not retrieved.
Eligibility criteria and quality assessment
Once duplicate documents had been deleted, the titles and abstracts of the obtained studies were screened by two reviewers (A.J. and P.R.) independently following these criteria.
Inclusion
Randomized clinical trials, prospective studies, retrospective studies, and case series that focused on PBM as a treatment for MRONJ, published in English and included more than or equal to five patients with a mean follow-up period of at least 6 months.
Exclusion
Animal studies, in vitro studies, reviews, studies that did not use PBM, studies that were not published in English, studies with fewer than five patients, or studies with a mean follow-up period of less than 6 months.
Cohen's kappa coefficient was used to assess the level of agreement between the reviewers. In the case of a dispute between reviewers, a senior investigator (R.F.) decided whether or not the article would be included in the analysis. Selected articles were included in the quality assessment and full-text review.
The quality assessment was carried out, taking into account factors contributing to bias in the outcome. The evaluated parameters were adapted from Papadopoulos et al. 23 and Zen Filho et al. 24 A complete list of the variables mentioned above is shown in Table 1. Based on the above assessment, the selected studies were classified as low (0–5 points), medium (6–11 points), or high (12–16 points). Only studies classified as high or medium quality were included in this analysis as demonstrated in Table 2.
Quality Assessment Criteria
Quality Assessment of the Included Studies
0–5 points: low quality; 6–11: medium quality; and 12–16: high quality.
Data extraction
After a thorough reading of each article, a structured extraction form was used independently by two authors (P.R. and A.J.) to obtain the following data from the selected articles: First author, demographic characteristics (number of patients, age, gender, type of medication, AAOMS stages distribution), PBM characteristics (type of laser, wavelength, mode, power, energy density, power density, number of sessions, and protocol of irradiation) and outcomes.
Result
A total of 269 articles were found through an electronic search of four databases, consisting of 60 articles from PubMed, 53 articles from Web of science, 95 articles from Scopus, and 61 more articles from the Cochrane library. Moreover, four more articles were retrieved from the manual search of the literature. After removing 101 duplicates, titles and abstracts of the remaining 172 records were screened, and 45 of them were selected for full-text screening concerning the inclusion and exclusion criteria. Thirty-three articles were then excluded due to not meeting the inclusion criteria. Twelve selected articles were assessed by the quality-mentioned above assessment method, and an article classified as the low quality was removed from the data analysis. Thus, 11 articles were chosen for qualitative analysis. A flowchart of how the studies were selected is illustrated in Fig. 1.
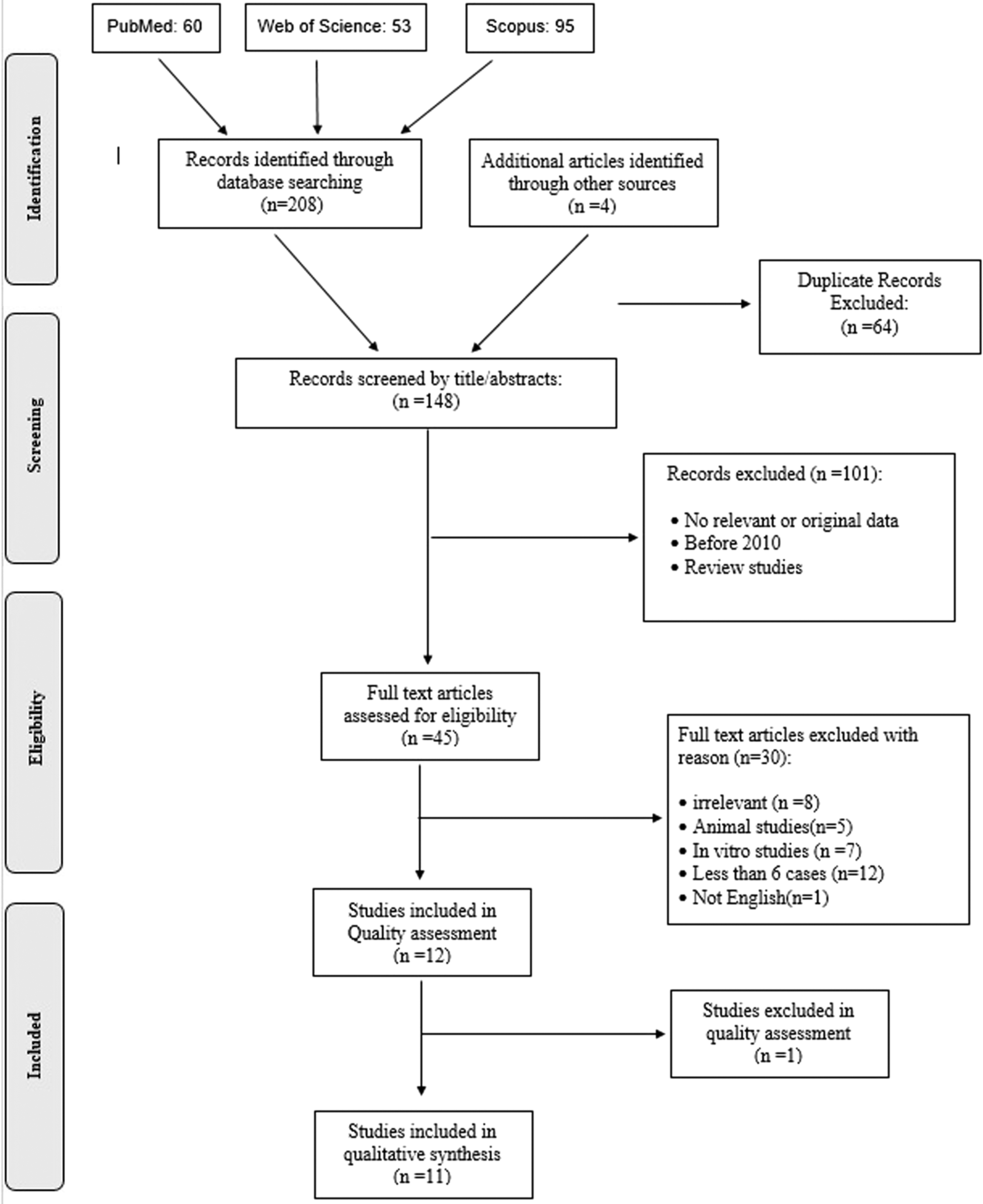
Flow diagram of the study selection.
Cohen's kappa coefficient of agreement between the reviewers was κ = 0.76. This kappa coefficient signifies substantial agreement based on the Landis and Koch interpretation. 25
Characteristics of the Selected Publications
Methodological and demographic data extracted from each of the included studies are shown in Table 3. The included studies consisted of nine retrospective studies, 26 –34 one prospective 35 study, and one case series. 36 A total of 759 patients with a mean age ranging from 54 to 74 were assessed in this review. Females were the most frequent gender in all selected studies (72% females to 28% males). The underlying disease, which resulted in the use of medication, in most of the patients (79%) were an oncologic condition consisting of prostate cancer, 27,28,32,34 bladder cancer, 34 breast cancer, 27,28,32,34 neuroendocrine tumor, 27 lung cancer, 28,32,34 multiple myeloma, 26 –28,30 –32,34 and bone metastasis. 26,30,31 In contrast, in the others (21%) osteoporosis was the initial disease. In one study, the number of oncologic or nononcologic lesions was reported, 33 yet, a previous oncologic disease could be seen in most of the stated lesions (72%).
Methodological Information, Demographic Data of the Included Studies
Patients.
Sites.
ALE, Alendronate; BIS, biophosphates; CHX, Chlorhexidine; CLO, Clodronate; CS, conventional surgery; DEN, Denosumab; Er:YAG, Erbium-doped yttrium aluminum garnet; IBA, Ibandronate; LAS, Laser-assisted surgery; L-PRF, Leukocyte- and platelet-rich fibrin; Man, Mandible; Max, Maxilla; NER, Neridronate; NM, Not Mentioned; PAM, Pamidronate; PBM, photobiomodulation; PostOP, Postoperative; PreOp, Preoperative; PRP, platelet-rich plasma; RIS, Risedronate; ZOL, Zoledronic acid.
Seven studies 27 –29,32,34 –36 have mentioned the type of BP in use, which was consisted of zoledronate, pamidronate, alendronate, clodronate, ibandronate, risedronate, neridronate, and combinations of them. Zoledronate was the most used medication in these studies (N = 163). Only two studies reported the use of denosumab with or without BPs. 33,34 Favia et al. 33 classified the lesions by the medicine responsible for them into three groups of BPs, denosumab, and both.
Most studies reported the MRONJ stages based on the AAOMS staging system by Ruggiero's classification. 4 The most frequent stage in the studies mentioned above was stage II (66%), then I (18%), and finally III (16%). Scoletta et al. 35 classified the lesions into three classes of I, II, and III and subclassified them into IA, IB, IIA, IIB, IIIA, and IIIB, based on the lesion's size or symptoms.
Types of lasers utilized in the evaluated studies were consisted of pulsed GaAs diode laser, 35 neodymium-doped yttrium aluminum garnet (Nd:YAG), 26,27,29 –31,36 indium gallium aluminum phosphide diode laser, 28 gallium aluminum arsenide diode laser, 32 diode laser (not specified), 33 and multidiodic laser. 34 Their wavelengths varied from 650 nm 34 to 1064 nm 26,27,29 –31,36 with a power range of 0.007 W 35 to 1.25 W. 26,27,29 –31,36 Complete characteristics of the lasers used in all the selected articles are shown in Table 4.
Photobiomodulation-Associated Treatments Characteristics
CW, continuous wave; Nd:YAG, neodymium-doped yttrium aluminum garnet; PW, pulsed wave; SPW, super pulsed wave; VSP, very short pulse.
The following treatment plans were used: Medical; 26,28 –31,36 PBM; 35 Medical+PBM; 26,29 –31,33,34,36 Medical+Conventional Surgery (CS); 26 –31,33,34,36 Medical+CS+PBM; 29,31,32 Medical+Laser-assisted surgery+PBM; 26,27,29 –31,36 and Medical+CS+Autologous Platelet Concentrates (APCs). 28,34 A complete list of each studies utilized treatment plans and their outcomes is shown in the Table 5.
Outcome Characteristics
Number of patients were considered as number of lesions.
To assess the effect of different treatment plans on MRONJ, a clinical parameter known as “clinical success” has been introduced.
37
It is defined as: Complete healing of the mucosa with no signs and symptoms (complete healing) Shifting from a higher stage (based on AAOMS staging system) to a lower stage (healing improved)
Due to the chronic nature of the MRONJ and possible relapses, these results must be maintained at least for 3 months to be defined as “Clinical Success.”
The success and complete healing rates of the evaluated studies are listed in Table 6.
Treatment Plans Characteristics
APC, Autologous Platelet Concentrates (PRP, L-PRF).
Discussion
Despite the importance of MRONJ as a severe complication of antiresorptive medications, there is still considerable ambiguity regarding its treatment. Currently performed therapies are either too aggressive or woefully insufficient. 38,39 As a primary or adjunctive therapy, recently suggested alternatives have shown promising results. 40 One of these adjunctive treatments is PBM, which necessitates a thorough understanding of its use. This topic has been the subject of a few systematic reviews. 40 –42 However, due to the rapidly growing literature, a new and comprehensive review of the current literature is essential. Apart from the article's recency, the current study's inclusion criteria were carefully chosen to include studies that use PBM as a treatment for MRONJ.
Medical therapy
Many writers have characterized the conservative strategy as the gold standard in MRONJ therapy since it decreases clinical symptoms and avoids disease progression. 43 AAOMS stated that conservative treatment by antimicrobial mouth rinses and antibiotic medication is limited to the early phases of the lesion. 4 Patients in stages I and II of BRONJ are more likely to recover with just antimicrobial therapy, an essential consideration in treatment strategy. 44,45
Atalay et al. 27 suggested that drug treatment, including combination systemic antibiotic treatment, chlorhexidine mouth-rinse, and anti-inflammatory medications, may only offer transient pain relief and local infection control and cannot be linked with any long-term improvement. Vescovi et al. found no complete wound healing or even healing in any of the 13 sites of BRONJ lesions managed with medication treatment alone in a retrospective analysis of 91 individuals with BRONJ affecting different locations in the oral cavity a follow-up period of at least 3 months. 26 The 3-month follow-up period was considered acceptable for evaluating the effectiveness of antibiotic treatment, which can typically only control the acute infectious process for a short time (3–4 weeks) before signs and symptoms return. Drug treatment alone can only alleviate the clinical symptoms of BRONJ, according to the data presented in the included trials, with no long-term therapeutic outcomes. 26,30
Of the studies included in this systematic review, 93 MRONJ sites were treated by medical therapy alone in the included studies, which improved the healing in one out of four patients, with the least success rate of all treatment modalities.
PBM therapy
PBM as a preliminary treatment plan was only used in one of our included studies, 35 a prospective cohort consisting of 20 treated sites using pulsed GaAs diode laser as a primary treatment for 20 patients with the use of BP medication in oncologic or nononcologic conditions. Despite the study's claims of a 60% healing improvement rate and a significant reduction in pain and clinical inflammatory parameters, none of the treated patients experienced complete wound healing. These results might suggest that PBM therapy should be used as an adjunctive rather than a primary treatment. However, further clinical investigations with larger sample sizes need to be performed to validate these results, which might be somewhat an issue due to ethical concerns.
Medical+PBM therapy
This treatment strategy was used on 157 sites throughout seven studies. 26,29 –31,33,34,36 Forty-five of them have demonstrated complete healing, and 40 have exhibited only improvement in their healing, while others have shown no sign of enhancement. The results of almost all of our included studies have shown that adding PBM (due to its osteoblastic stimulating properties) as an adjuvant therapy to medical therapy alone significantly improves treatment outcomes. 26,29 –31,34,36 The studies, as mentioned earlier, also showed a significant difference in the outcomes gained from surgical therapies over conservative nonsurgical therapies, particularly in terms of complete lesions healing. 26,29 –31,33,34,36
Nonetheless, the recommended treatment plan for stage I and stage II MRONJ, according to the AAOMS position article, consists mostly of antibiotic therapies and pain control to avoid lesion extension and control of pain and prevention of lesion extension rather than complete healing of them. 4 Therefore, the results of this study suggest that nonsurgical therapy should only be used in medically compromised patients who are unable to endure surgical treatments. These results are in good agreement with the recently conducted review by AlDhalaan et al. 46
Medical+CS
Surgical therapy is preferred when MRONJ occurs in both neoplastic and non-neoplastic individuals, as nonsurgical therapies do not appear to promote complete healing of the lesions. 33 Sequestrectomies, superficial debridement, curettage, corticotomies, and surgical excision of surrounding alveolar or cortical bone were performed with conventional surgical instruments such as a cold blade scalpel and rotary cutting devices.
Some researchers have claimed that aggressive surgical treatments, including debridement and resection, hardly result in long-term satisfactory wound healing and may exacerbate the condition, 47 –49 while for Hayashida et al., surgical intervention should be the primary option for complete healing in MRONJ lesions. 50 The study conducted by Favia et al. implies that a complete cure of MRONJ lesions is only possible with surgical excision of necrotic and infected bone, with no clinical or radiological indications of residual pathology. 33 Surgical therapies also allow histological examination of tissues, exposing uncommon but life-threatening consequences, including metastatic lesions from the initial neoplastic malignancy localized in the bone. 51
Even though surface debridement to reduce soft tissue irritation in Stage II was indicated in the most recent version of the AAOMS position document, surgical therapy should be reserved for individuals with Stage III illness. 4 In the afflicted areas, necrotic bone can impair wound healing and mucosal regeneration. Furthermore, even if complete healing does not happen following surgery, significant improvement in patients' conditions has been observed due to the lesions' downstaging, which is probably linked to enhanced patients' quality of life. 33,52
More significant regions of exposed and uncomfortable infected bone may occur from aggressive surgical therapy. Surgical debridement or resection, along with antibiotic treatment, may provide long-term relief while also resolving acute infection and discomfort. Visible mobile bony sequestrum segments should be excised without exposing unaffected bone, and remaining bone surfaces should be covered with local soft tissue closure. 53
Medical+CS+PBM therapy
For individuals with MRONJ, a combination of medical therapy, CS, and PBM is a promising therapeutic option. On 87 MRONJ sites and within three studies, this treatment strategy resulted in a 73.56% complete healing rate and an 86.20% success rate. 29,31,32 As previously stated, CS was carried out with traditional surgical instruments and removed necrotic bone with as minor damage to surrounding tissue as possible. In the study by Vescovi et al., five sites in noncancer patients and 34 sites in cancer patients were treated with this treatment modality, resulting in complete healing of all sites in noncancer patients and 24 of 34 in cancer patients. Four other cancer patients' lesions also showed signs of partial recovery.
Although no statistical analysis of the outcomes of CS with PBM versus CS alone has been done, adding PBM appears to improve the results in this study. 31 In another study, Vescovi et al. found that 24 of 33 (72.72%) lesions completely healed after using this strategy. Even though this rate is 64.7% (11 of 17) in CS alone, there was no statistically significant difference between the outcomes of these two groups. 29 Furthermore, a retrospective analysis of 11 cases by Altay et al. has found favorable results in all cases. 32
Medical+laser-assisted surgery+PBM therapy
In the treatment of MRONJ patients, laser surgery is a viable option. Erbium family lasers are the laser of choice for these procedures because of their superior absorption by hydroxyapatite and water. Erbium-doped yttrium aluminum garnet (Er:YAG) laser produces an ablated surface, optimal for cell adhesion and conductive to bone regeneration with minimal heat injury to surrounding tissue and precise and clean incisions. 54,55 Compared to other traditional tools, this leads to faster and better healing. 56 –59 It also distinguishes avascular regions from vascularized sections of the bone by preventing coagulation and carbonization. This also induces revascularization by causing bleeding from the healthy bone. 60 The Er:YAG laser is a pulsed laser with a frequency of 4 to 50 Hz and a 100 to 1000 μs pulse length.
However, among the studies included, the most frequently utilized parameters were Er:YAG with a very long pulse for tissue ablation and resection and a very short pulse for vaporizing necrotic bone, a fluence of 50 to 60 J/cm2. In these studies, iodopovidone solution and distilled water were used as irrigation. One hundred forty-three MRONJ sites were treated with laser-assisted surgery throughout 6 studies, resulting in 120 completely healed and 16 partially healed MRONJ sites. Early conservative surgical procedures with Er:YAG and PBM yielded the best results in the majority of the evaluated studies. 26,27,29 –31,36 This treatment approach could result in total mucosal healing, making it the treatment of choice at this moment.
Medical+CS+APCs+PBM therapy
APCs are biocompatible, easy, pliable, and safe oral surgical products that appear to be particularly beneficial in MRONJ surgical treatment since lack of vascularization is a crucial component in MRONJ etiology. 61
For such reasons, Leukocyte and platelet-rich fibrin (L-PRF), a second-generation APC, is recommended over platelet-rich plasma (PRP). First, removing anticoagulants during preparation guarantees that it is 100% autologous and free of chemicals. Hence, an immunogenic response is less likely. Second, its enhanced formulation enables liquid or solid usage. Moreover, L-PRF has enhanced sustained effect over 7 to 28 days compared to PRP. 34,62
An autologous concentration of platelets is found in PRP. This procedure produces a high number of human platelets, which actively release protein growth factors and assist in repairing wounds. 28 Some writers on MRONJ have utilized PRP as an additional treatment to improve bone repair. The combination of antibacterial characteristics of systemic antibiotics, APC's positive influence on tissue regeneration and angiogenesis, and PBM's biophysical features appeared successful in treating MRONJ, as evidenced by the closure of the exposed bone in 25 of 27 sites from the two included studies. 28,34
Thus, combining pharmacological and surgical treatment with PBM and PRP positively affects MRONJ healing in oncology patients. On the contrary, Del Fabbro et al. found a significant lack of evidence for the use of APCs in postextraction sockets due to the short follow-up duration and variability of the trials examined in their review. 61
It has been demonstrated that intraoperative and postoperative laser biostimulation can promote mucosal and bone healing, primarily when PBM is used to treat early-stage lesions. The interaction between PBM with the bone healing process involves a two-step mechanism; the first is likely connected to the stimulation of osteoblasts to create a bone matrix. An inhibitory photobiological mechanism would reduce osteoblast activity, whereas PBM would increase osteoclast activity to facilitate bone resorption and rebuilding in a later stage. 63 –65
PBM of bone tissue promotes the remodeling of bone tissue by increasing the amount of mRNA required to make type I collagen. 66,67 The energy obtained by intracellular chromophores, particularly mitochondrial chromophores, is transformed into metabolic energy by action at the mitochondrial respiratory chain in bone tissue. 26,68,69 Yamamoto et al. further claim that PBM stimulates osteoblast proliferation via increasing the expression of the minichromosome maintenance complex family of genes. 70
In terms of the impact of PBM on soft tissue repair, Lee et al. found that PBM reduced apoptosis caused by alendronate in a culture of alendronate-treated oral keratinocytes. PBM also improved cell viability, cell migration, protein synthesis linked with angiogenesis, and wound healing after alendronate therapy. 71 PBM improves oral soft tissue healing by shortening the exudative phase and stimulating reparative processes, transforming fibroblasts into myofibroblasts, increasing blood flow through angiogenesis and capillary growth, and various growth factors release, faster formation, and increased deposition of collagen type I and III. 30,72
There is still no consensus on the standard protocol of PBM in the treatment of MRONJ. 73 In most of our included studies, a pulsed Nd:YAG (1064 nm) laser with an energy density ranging from 2.0175 J/cm2 (Refs. 26,29,36 ) to 14.37 J/cm2 (Refs. 30,31 ) was used. Also used were pulsed 34,35 or continuous mode 28,32 diode lasers with wavelengths ranging from 650 nm 34 to 904 nm. 35 1.25 W was the most commonly utilized laser power. 26,29,30,36,74 40 mW, 200 mW, 0.5 W, 0.59 W, 0.64 W, and 1 W were among the other powers used. 27,28,32 –35 These lasers were used mostly with 2 mm probe distance from the affected area in eight sessions of treatment. 26,29,30,36,74 Average exposure duration of 348.6 sec was used in each session.
Although PBM as adjuvant therapy for MRONJ can significantly improve clinical outcomes, 26,27,30,32,34 surgical excision of necrotic bones is required to completely heal these lesions, 26,29 –31,33,34 according to the findings of this review. These findings are consistent with earlier research. 41,46 However, they differ with the AAOMS policy document on MRONJ, 4 which restricts surgery to the most severe phases of MRONJ lesions. Complying with this strategy might result in missing early stages of MRONJ progression, which have been shown to have significantly better treatment results than late stages. 29 Another outcome of the study is that Er:YAG laser-assisted surgery is an effective treatment option for a conservative operation, resulting in full healing of most lesion sites. 26,27,29 –31,36 This finding is inconsistent with that of Momesso et al. 42
The findings of this research suggest PBM using an Nd:YAG laser with 1.25 W power as an adjunct treatment to surgery, preferably laser-assisted, for the treatment of MRONJ lesions. Another innovative therapeutic strategy examined in our study was the use of APCs combined with CS and PBM, which had the highest success rate among other treatment plans. 28,34 However, the lack of evidence on this new treatment plan serves as a stimulus for future research. The data obtained from this study along with other studies on this matter, if stored and shared correctly, can help us in making precise and patient centric decisions in the treatment of MRONJ patients. The use of blockchain, which is a secure and immutable means of data sharing, can help us regarding this issue. However, further studies are needed to prove blockchains' application in health care. 75
In conclusion, the evidence from this study supports the idea of PBM as only an adjunct treatment for MRONJ patients. Our results indicate that the Medical+CS+APCs+PBM therapy protocol could be utilized in the clinical management of the MRONJ lesions and, hopefully, enhance the questionable prognosis of MRONJ management, thus improving these patients' quality of lives considerably. However, due to the absence of solid clinical evidence such as randomized controlled trials and a lack of reporting regarding laser parameters, these results must be interpreted with extreme caution. Future research based on higher quality evidence could help us achieve greater accuracy in this area. We believe that the present findings might be valuable in choosing the best treatment approach for patients with MRONJ.
Future research based on higher quality evidence could help us achieve greater accuracy in this area.
Footnotes
Authors' Contributions
P.R.: methodology, investigation, data curation, and writing—original draft; A.J.: investigation, data curation, and writing—review and editing; P.V: supervision, writing—review and editing; R.F.: conceptualization, validation, supervision, and project administration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.