
Abstract
Background:
Blue light exhibits the ability to deactivate catalase present in pathogens, significantly improving the antimicrobial performance of compounds such as hydrogen peroxide (H2O2). However, H2O2 is not used within clinical settings due to its short half-life, limiting its potential applications. In this study, we explore the usage of Food and Drug Administration-approved and clinically used silver sulfadiazine (SSD) as a potential alternative to H2O2, acting as a reactive oxygen species (ROS)-producing agent capable of synergizing with blue light exposure.
Materials and methods:
For in vitro studies, bacterial strains were exposed to a continuous wave 405 nm light-emitting diode (LED) followed by treatment with SSD for varying incubation times. For in vivo studies, bacteria-infected murine abrasion wounds were treated with daily treatments of 405 nm LED light and 1% SSD cream for up to 4 days. The surviving bacterial population was quantified through agar plating and colony-forming unit quantification.
Results:
Through a checkerboard assay, blue light and SSD demonstrated synergistic interactions. Against both gram-negative and gram-positive pathogens, blue light significantly improved the antimicrobial response of SSD within both phosphate-buffered saline and nutrient-rich conditions. Examination into the mechanisms reveals that the neutralization of catalase significantly improves the ROS-producing capabilities of SSD at the exterior of the bacterial cell, producing greater amounts of toxic ROS capable of exerting antimicrobial activity against the pathogen. Additional experiments reveal that the incorporation of light improves the antimicrobial performance of SSD within methicillin-resistant Staphylococcus aureus (MRSA)- and Pseudomonas aeruginosa strain 1 (PAO-1)-infected murine abrasion wounds.
Conclusions
: As an established, clinically used antibiotic, SSD can act as a suitable alternative to H2O2 in synergizing with catalase-deactivating blue light, allowing for better translation of this technology to more clinical settings and further implementation of this treatment to more complex animal models.
Introduction
In recent decades, the proliferation of antibiotic resistance has emerged as a ticking time bomb within the health care community. Due to agricultural and medical overuse, as well as slowing drug development, antibiotic resistance has developed within a wide array of bacterial strains. 1 –3 The spread of resistance is estimated to not only increase the mortality of infections but also induce severe economic stress, increasing yearly global health care costs from $300 billion to more than $1 trillion by 2050. 4 –6 Given these concerns, there is a need to develop alternative methods to treat infections.
In the past few years, blue light phototherapy has emerged as an exciting alternative to antibiotics due to its strong antimicrobial capabilities against a wide variety of pathogens. 7 –9 Recent studies exploring the mechanisms of blue light phototherapy have found that 405–410 nm light induces the structural deactivation of catalase within both bacterial and fungal species. 10,11 Catalase, a commonly expressed antioxidant enzyme found in aerobic organisms, is responsible for converting the toxic reactive oxygen species (ROS) hydrogen peroxide (H2O2) to water and oxygen. 12 Combining blue light with H2O2 was found to significantly improve the antimicrobial effectiveness of H2O2 against pathogens in both in vitro and in vivo conditions. Despite this, H2O2 usage remains problematic, as H2O2 is not utilized in clinical settings due to its extremely short half-life and high potential oxygen production, rendering it unsuitable for long-term treatments. 13 –15 Given these concerns, alternatives to H2O2 are needed for potential clinical translation.
The antibiotic silver sulfadiazine (SSD) has emerged as an ideal alternative to H2O2 for synergy with blue light. As a Food and Drug Administration-approved antibiotic, SSD is most often used for the treatment of infected burns and wounds. 16 –18 SSD exerts its mechanism of action partly through the binding of silver ions to amino, carboxyl, phosphate, imidazole, and thiol groups in proteins, triggering protein denaturation and inactivation. 19,20
However, this binding is believed to indirectly cause intracellular ROS generation by disrupting proteins within the bacterial respiratory chain. 21 This ROS-generating capability, alongside its clinical usage, makes SSD an ideal compound to synergize with catalase deactivation. This theoretical synergy can also potentially improve the overall efficiency of the drug, helping minimize side effects such as inhibited wound healing by improving bioburden clearance and reducing the SSD application duration. 22 –24 Thus, we hypothesize that light-induced catalase deactivation can improve the efficiency of SSD within both in vitro and in vivo environments.
Materials and Methods
Blue light source
Blue light was applied through a continuous wave 405 nm light-emitting diode (LED) (M405L4; Thorlabs) focused through a collimation adapter (SM2F32-A; Thorlabs). This application of 405 nm light will henceforth be referred to as CW-405. The CW-405 light beam was adjusted to obtain an illumination zone of 1 cm2. Fluence was controlled via a T-Cube LED Driver (LEDD1B; Thorlabs) and applied at a constant 200 mW/cm2.
Bacterial strains
Wild-type Escherichia coli BW25113 and its catalase negative mutant E. coli
SSD preparation
For in vitro studies, SSD salt (481181; Sigma–Aldrich) was dissolved in diluted (0.7–1.4%) ammonium hydroxide (NH4OH) (L13168; Alfa Aesar). For in vivo studies, topical 1% SSD cream (67877012450; Ascend) was used.
In vitro blue light catalase deactivation and SSD treatment
Bacterial strains were cultured overnight in tryptic soy broth (TSB) to stationary phase. The next day, bacteria was resuspended and diluted in 1 × phosphate-buffered saline (PBS) to an OD600 of 1.0. For light treatment, bacterial aliquots were placed on a coverslip and exposed to 200 mW/cm2 of CW-405. For a checkerboard assay, 2 μL droplets were treated for 0, 2.5, 5, 10, 20, and 40 min, diluted in 2 mL of TSB, and plated in a 96-well plate. Following this, SSD was diluted twofold from a concentration of 64 μg/mL to concentrations of 32, 16, 8, and 4 μg/mL. The assay was incubated at 37°C for 48 h before the OD600 was measured with a plate reader to identify the minimal inhibitory concentration (MIC) of CW-405 and SSD alone and in combination. Synergistic interactions were determined by calculating the fractional inhibitory concentration index (FICI) defined by the following equation:
25
Catalase rescue and salvaging
Overnight cultured PAO-1 and MRSA were subjected to light treatment as described previously. Following treatment, 100 μL of 1 mg/mL bovine catalase (C9322; Sigma–Aldrich) was added to 900 μL of each suspension, adding 200–500 U of catalase to each solution. Next, 2 μg/mL of SSD was added. The suspensions were incubated for 1 h at 37°C, plated, and quantified.
ROS detection and quantification
ROS production was quantified through a hydroxyl radical and peroxynitrite sensor (HPF) dye (H36004; Thermo Fisher Scientific). Overnight cultured PAO-1 and MRSA were treated to 60 J/cm2 of CW-405 and 2 μg/mL of SSD in the process as described previously. Following SSD addition, 2 μM of HPF was added and suspensions were incubated for 30 min at 37°C. Once complete, 100 μL of suspension was transferred to a 96-well plate and fluorescence (n = 3) was quantified at an excitation/emission setting of 490/515 nm. Background fluorescence was quantified by adding 2 μM of HPF to PBS and incubating the solution in 37°C for 30 min. Measured fluorescence was normalized by subtracting the background fluorescence.
In vivo murine model
Murine abrasion wounds were generated following the procedure established by Dong et al. 10 Seven- to eight-week-old BALB/c female mice (000651; Jackson Laboratory) were dorsally shaved and placed under isoflurane anesthesia. 1 cm2 abrasion wounds were created by a No. 15 sterile scalpel. A 10 μL aliquot containing 106 CFU of log phase MRSA or 108 CFU of log phase PAO-1 was applied to the surface of each wound. Treatment began 2 h after infection. For each bacteria tested, mice were separated into four groups: untreated, light only, SSD only, and combination. Light treatment consisted of two 60 J/cm2 CW-405 treatments applied onto wounds with 5-min breaks between treatments. A single light session would consist of 120 J/cm2 of exposure. For SSD treatment, 1% SSD cream was applied directly to the wound surface. In the combination treatment groups, mice would receive light treatment followed immediately by SSD cream application.
For the MRSA wounds, the untreated, SSD only, and combination groups consisted of n = 7 wounds, whereas the light only group consisted of n = 5 wounds. The MRSA groups were treated daily over 4 days for a total light dosage of 480 J/cm2. Twenty-four hours after the last treatment, MRSA-infected mice were euthanized and the wounds were extracted, homogenized in 2 mL of PBS, and plated on Staphylococcus aureus selective mannitol agar plates. For the PAO-1 model, each group consisted of n = 4 wounds. The PAO-1 groups were treated twice in the span of 24 h, with 12-h breaks between sessions, totaling to a final dosage of 240 J/cm2. Four hours after the last treatment, PAO-1-infected mice were euthanized and wounds were removed, homogenized, and plated on P. aeruginosa selective cetrimide agar plates. The resulting CFU was then quantified.
Statistical analysis
Student unpaired t-tests were used to conduct statistical analysis via GraphPad PRISM version 9.0.0. Significance (*) was set at p-values <0.05.
Study approval
Murine infected abrasion models were approved under protocol PROTO201800535 by the Institutional Animal Care and Use Committee (IACUC) at Boston University.
Results
Blue light and SSD exhibit synergistic response
To confirm synergy between blue light and SSD, a checkerboard assay was performed on the model bacteria E. coli BW25113 to identify the FICI in TSB (Fig. 1a). The FICI can be used to determine the type of interactions between two agents, with synergistic interactions identified though FICI values ≤0.5. 26 E. coli was found to exhibit an MIC of 480 J/cm2 for CW-405 and 32 μg/mL for SSD. In contrast, the MICs of the agents in combination were found to be 60 J/cm2 for CW-405 and 8 μg/mL for SSD. Based on the FICI equation listed, these values correspond to an FICI of 0.375, confirming the presence of synergy. To further explore the capability of light to improve SSD performance, the CFU of E. coli after light and SSD treatment was evaluated. Following 1 h of incubation in PBS, both 60 J/cm2 light and 2 μg/mL SSD reduced the CFU of E. coli by less than 0.5 log. In contrast, the combination treatment completely eradicated the E. coli population beyond the detection limit (Fig. 1b).
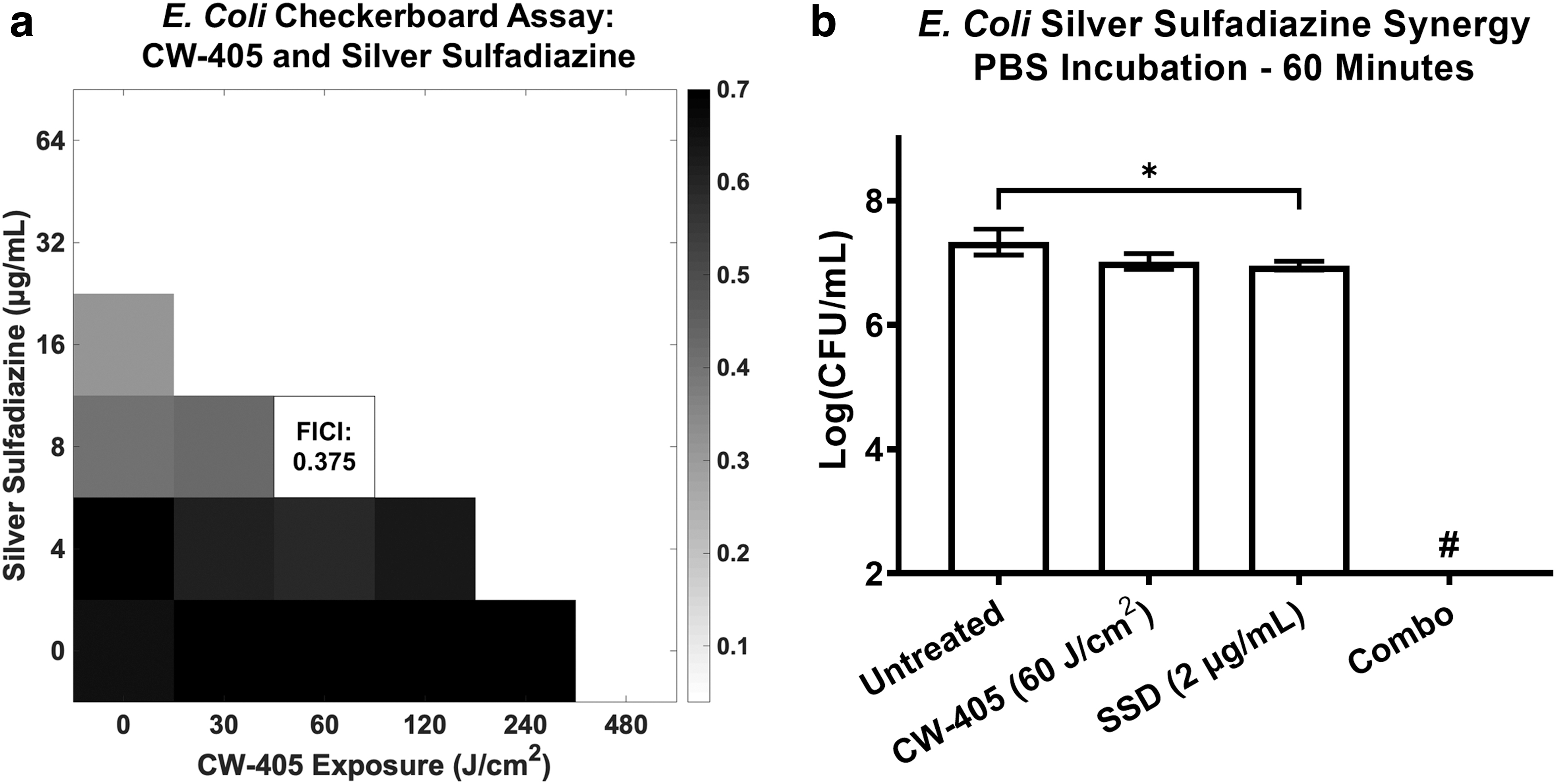
Combination of catalase-deactivating CW-405 and SSD results in synergistic interactions within model bacteria organism Escherichia coli BW25113.
Next, the treatment was evaluated on gram-negative P. aeruginosa (PAO-1) and gram-positive MRSA. PAO-1 treated to either CW-405 or SSD (2 μg/mL) experienced a less than 0.5 log CFU reduction, whereas the combination-treated samples experienced complete eradication (Fig. 2a). MRSA treated to either CW-405 or SSD (5 μg/mL) resulted in a 0.5 log CFU reduction, whereas the combination treatment also demonstrated full eradication (Fig. 2b).
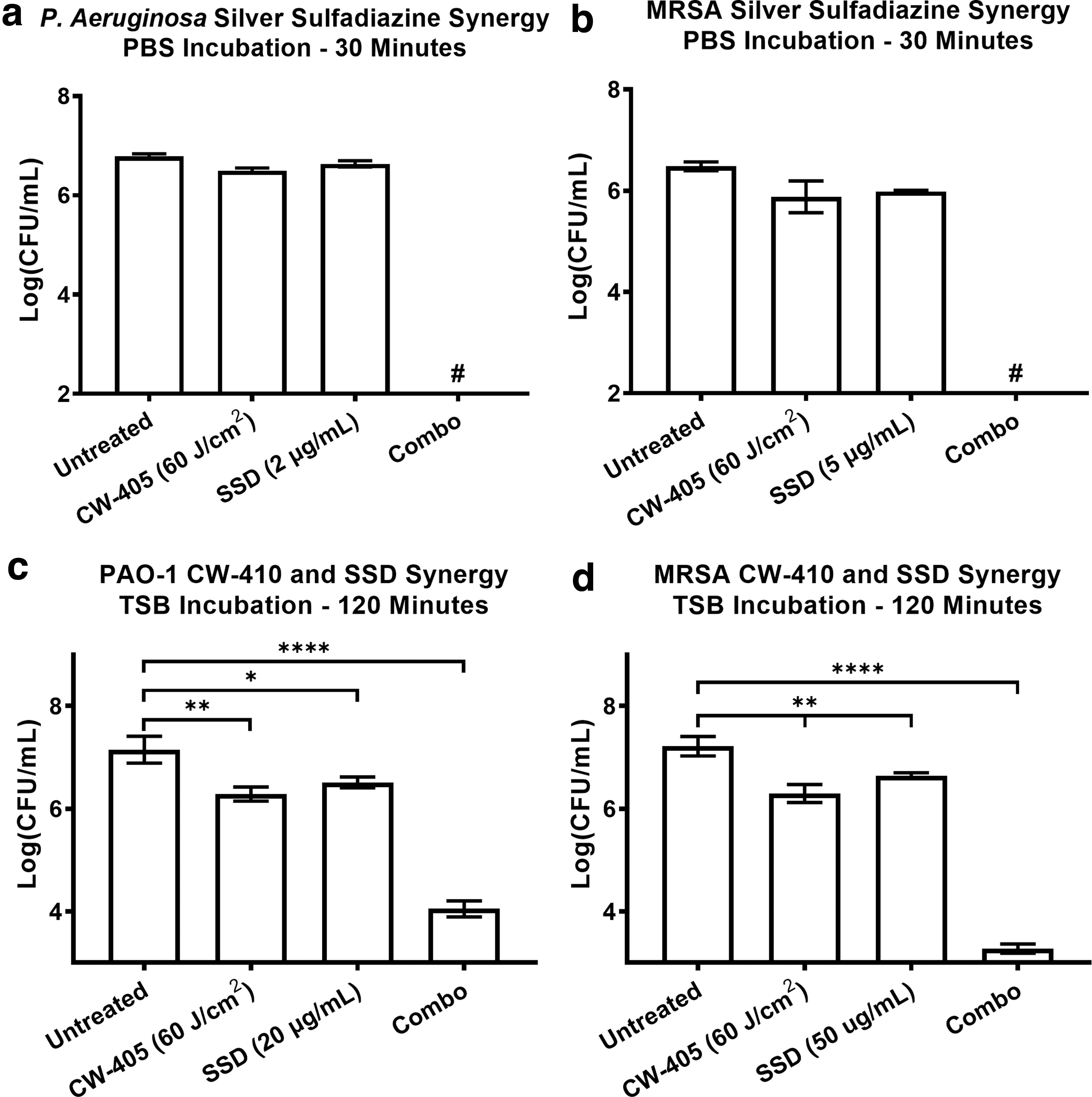
CFU measurements of CW-405 (60 J/cm2)-treated
Within more nutrient-rich environments, the combination treatment conducted on bacteria incubated within TSB for 2 h was found to require higher SSD concentrations to achieve an improved response. For PAO-1, CW-405 alone induced a 1 log CFU reduction, whereas treatment with 20 μg/mL of SSD induced a 0.5 log reduction. The combination treatment of PAO-1 resulted in a 3 log CFU reduction (Fig. 2c). For MRSA, treatment with CW-405 and 50 μg/mL of SSD resulted in a 1 and 0.5 log CFU reduction, respectively, identical to the PAO-1 results. However, the combination treatment of MRSA was slightly more effective with a log CFU reduction of 4 (Fig. 2d).
Mechanisms of blue light and SSD synergy
To investigate the mechanisms behind light and SSD synergy, the role of catalase against SSD activity was explored. In wild-type E. coli, combination treatments of CW-405 and SSD (1 μg/mL) induced a 1 log CFU reduction compared with the light-treated samples (Fig. 3a). However, the same treatment applied to the catalase-negative mutant E. coli
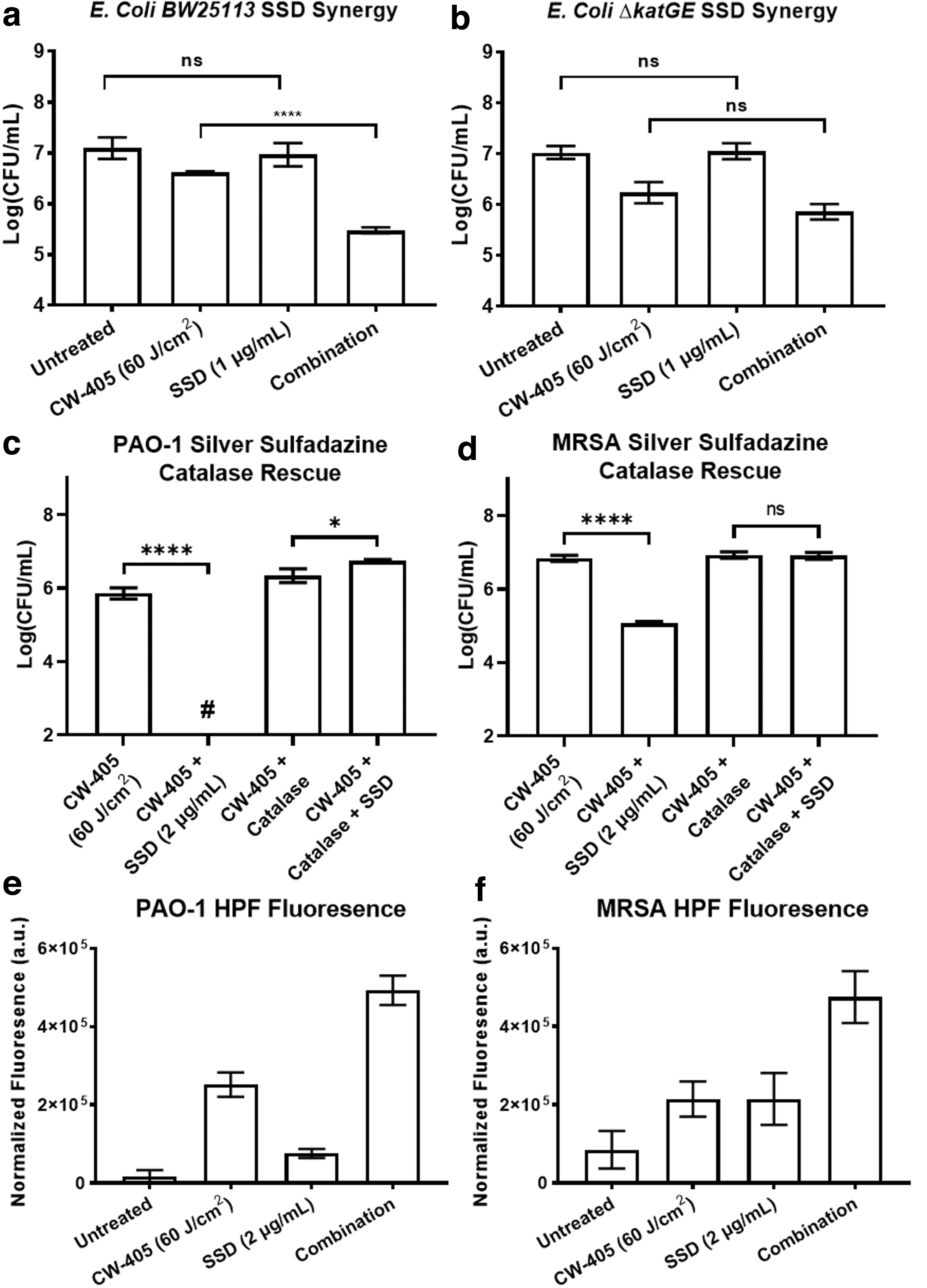
Mechanisms of CW-405 and SSD synergy. The combination of CW-405 (60 J/cm2) and low concentration SSD results in
For MRSA, while the combination treatment alone resulted in a 2 log CFU reduction, the addition of catalase resulted in no differences between the light- and combination-treated samples (Fig. 3d). These results indicate that increased ROS presence contributes to the increased antimicrobial activity of SSD, which exogenous catalase can neutralize. To confirm this, ROS levels were measured through an ROS-detecting HPF dye. In PAO-1, individual treatments of CW-405 and SSD increased HPF fluorescence by a factor of 13.7 and 3.4, respectively. In comparison, the combination treatment increased fluorescence by a factor of 27.7 (Fig. 3e). For MRSA, both CW-405 and SSD individually increased fluorescence by a factor of 1.5, whereas the combination treatment increased fluorescence by a factor of 4.6 (Fig. 3f).
In vivo murine model
A murine infected abrasion model was used to determine the effectiveness of blue light and SSD within in vivo conditions. Infected wounds (Fig. 4a) were fully covered with SSD to maximize exposure (Fig. 4b). CFU counts of MRSA wounds (Fig. 4c) indicate that while the light treatment alone had no significant effect on the bioburden of the MRSA wounds, SSD-treated MRSA wounds saw a near fourfold increase in bioburden. Despite this, the combination treatment resulted in an 85% decrease in MRSA bioburden (Fig. 4d). For PAO-1-infected wounds, CFU measurements (Fig. 4e) indicated that individual CW-405 or SSD treatment had no significant effect on the bioburden. Combination-treated wounds, however, experienced a 98% reduction in CFU bioburden, constituting a significant improvement in effectiveness (Fig. 4f).
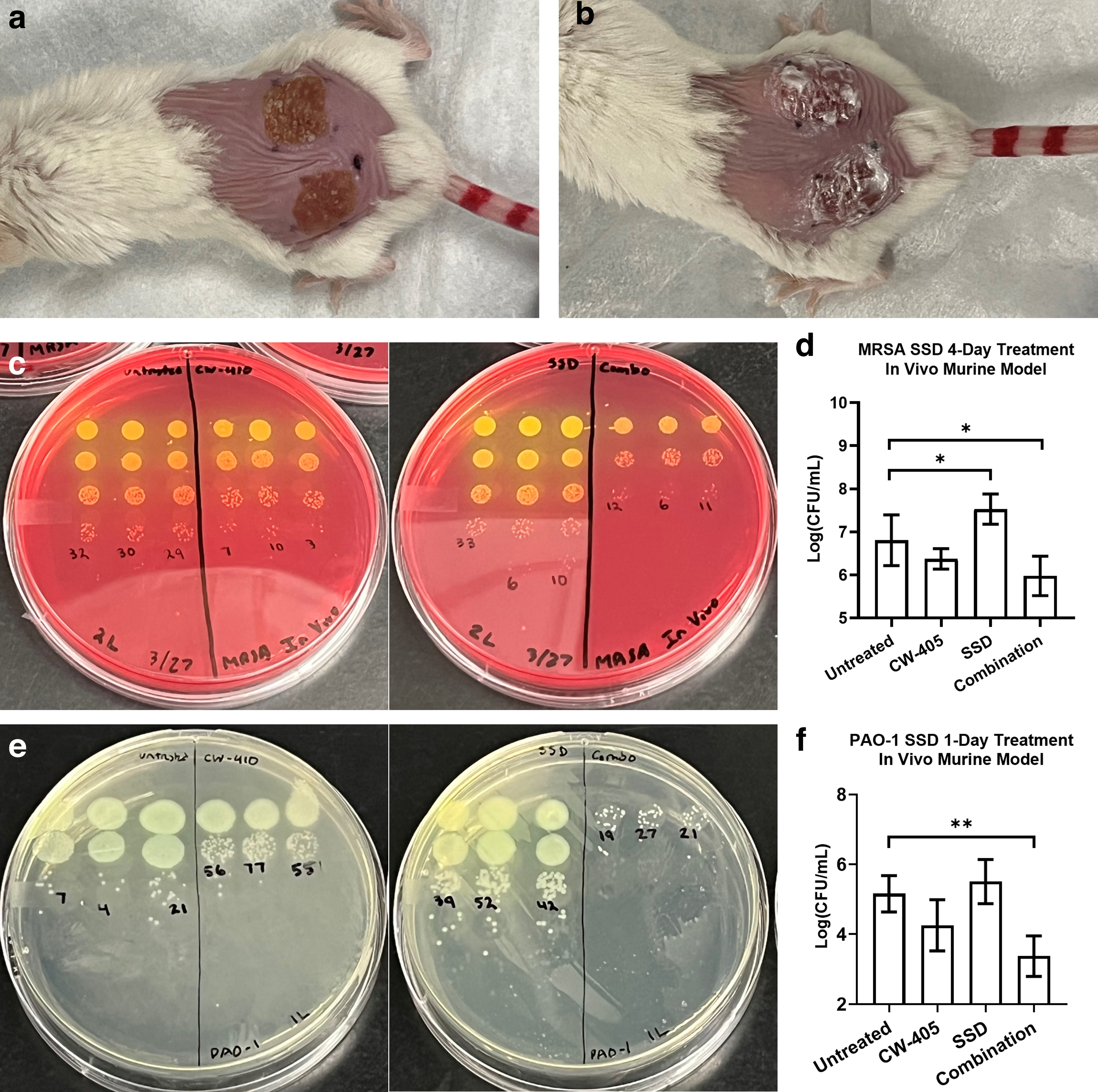
MRSA- and PAO-1-infected murine abrasion wound models were used to evaluate the effectiveness of blue light and SSD combination treatment.
Discussion
Based on their FICI, the combination of catalase-deactivating blue light and SSD exhibited strong synergistic interactions. The effectiveness of this treatment was further validated by the complete eradication of multiple bacterial strains within PBS upon treatment with both light and low dosage SSD. In comparison, the individual treatments of light or SSD exerted minimal impact on the bacteria, at most exerting a CFU log reduction of 0.5. These observed interactions between CW-405 and SSD behaved identically to the synergy observed between light and H2O2, indicating that SSD can act as a viable alternative to H2O2. 10
Like H2O2, catalase deactivation allowed for bacterial eradication through SSD at sub-MIC concentrations, with P. aeruginosa reported to have an MIC range of 16–32 μg/mL while MRSA strains have a range of 64–128 μg/mL. 27 Even within nutrient-rich environments, the improved efficiency of SSD by CW-405 was found to remain, although requiring higher concentrations of SSD. The greater SSD dosage needed to achieve improved efficiency can be attributed to the active metabolism of bacteria within the media, as exposure to sublethal ROS sources would trigger the overexpression of oxidative stress defense genes in response. 28 –30 Despite this, CW-405 incorporation significantly improves the performance of SSD by 3–4 log compared with the antibiotic alone.
The fact that light had no impact on the SSD activity in catalase-negative E. coli mutants indicates that it is the specific removal of catalase that contributes to the synergy between light and SSD. This is supported by the complete neutralization of the combination treatment observed by the addition of exogenous bovine catalase, which not only demonstrates the importance catalase plays as a defense mechanism against SSD but also indicates that the intracellular ROS produced indirectly by SSD can diffuse out of the cell into the exterior environment. 21
Without catalase presence, the intracellular ROS produced by light- and SSD-treated cells are likely increasing ROS levels within the bacterial environment, further propagating oxidative damage to surrounding cells. This increased ROS concentration caused by catalase removal is supported by the higher ROS levels detected within combination-treated bacteria. For PAO-1 and MRSA, the combination treatment fluorescence increased 62% and 53% over the added individual fluorescence of CW-405 and SSD, respectively. The increased ROS availability caused by the absence of catalase would provide more opportunities for the ROS to exert their antimicrobial activity on the cell, therefore increasing the efficiency of SSD following exposure to light.
Interestingly, the MRSA HPF fluorescence was found to be significantly lower than the PAO-1 fluorescence. The lower fluorescence is likely caused by the presence of additional antioxidants such as the membrane-bound staphyloxanthin pigment in MRSA neutralizing the ROS before they can react with HPF. 31,32 This pigment also likely contributes to the higher SSD resistance observed in MRSA.
While light and SSD exhibited clear synergy within an in vitro environment, in vivo studies showed promising results as well. Combination treatment in both MRSA- and PAO-1-infected wounds significantly enhanced the antimicrobial activity of SSD and achieved significant bioburden reduction compared with their untreated counterparts. In contrast, individual light treatments did not significantly differentiate from untreated samples for both bacterial models. While SSD only treatment had no effect on PAO-1-infected wounds, MRSA wounds treated with SSD alone were observed to experience a 401.1% increase in bioburden. This increase in MRSA population can likely be attributed to a combination of factors, such as the tendency for mice to lick their own or other mice's back in response to cream application. 33 Such interference would significantly reduce the SSD concentration available on the wound and lead to subinhibitory dosages, resulting in potential growth driven by the hormetic effects of subinhibitory antibiotic concentrations. 34,35
Regardless, infected wounds exhibited greater vulnerability to combination treatment, with PAO-1 infections demonstrating greater sensitivity to the treatment, achieving a near 2 log CFU reduction compared with the less than 1 log CFU reduction observed in MRSA. The sensitivity of PAO-1 to the combination treatment suggests that catalase deactivation may provide a way of resensitizing SSD-resistant P. aeruginosa to the drug, reviving the usage of the drug against previously resistant strains. 36,37 In addition, the increased effectiveness of SSD with light can allow for lower dosages and durations of SSD to be used against infected wounds, further minimizing potential side effects such as wound healing inhibition. 22 The effectiveness of this treatment can also provide a strong foundation for additional studies examining the effectiveness of this treatment on other types of infected wounds, such as chronic wounds or diabetic ulcers. 38,39
Conclusions
Overall, by combining catalase-deactivating blue light with SSD, we have established a nondrug-reliant method of sensitizing pathogens to an established clinical antibiotic. The improved effectiveness of SSD with CW-405 was found within a broad spectrum of pathogens in both PBS and nutrient-rich conditions. Application of CW-405 and SSD was also found to be effective within in vivo environments, providing a foundation for the incorporation of light into traditional treatments. By establishing SSD as a viable alternative to H2O2 in blue light synergy, we can provide a potential direction for the development of new antimicrobial agents that could be created to specifically synergize with light-induced catalase deactivation.
Footnotes
Authors' Contributions
S.J. and J.-X.C. conceived the idea of combining catalase deactivation with SSD. S.J. designed and conducted all experiments. J.-X.C. oversaw all experiments. S.J. and J-X.C. co-wrote the article.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a grant from the National Institutes of Health (R01AI141439) to J.-X.C.