
Abstract
Objective:
The aim of this study is to investigate the effectiveness of pulsed Nd:YAG high-intensity laser therapy (HILT) on body weight (Wt), body–mass index (BMI), waist circumference (WC), forced vital capacity (FVC), and forced expiratory volume in 1 sec (FEV1) in young adults with abdominal obesity (AO).
Materials and methods:
Thirty-seven young adult males (age 19–25 years) with BMI >30 kg/m2 and WC >102 cm participated in this 12-week, randomized controlled study and were randomly allocated into either Group I [received pulsed Nd:YAG HILT plus moderate-intensity aerobic exercise training (AET) program] or Group II (received placebo pulsed Nd:YAG HILT plus the same AET program). The variables were evaluated pre- and poststudy.
Results:
Poststudy mean values and percentages of changes were calculated for Wt [83.7 ± 6.58 kg (−6.14%) and 88.71 ± 5.09 kg (−4.29%)], BMI [29.27 ± 1.06 kg/m2 (−6.14%) and 30.09 ± 1.23 kg/m2 (−4.24%)], WC [105.44 ± 5.84 cm (−3.78%) and 109.42 ± 4.9 cm (−1.74%)], FVC [4.79 ± 0.4 L (+13.6%) and 4.39 ± 0.66 L (+5.89%)], and FEV1 [4.04 ± 0.22 L (+16.4%) and 3.82 ± 0.39 L (+8.8%)] for Group I and Group II, respectively. Between groups, there were significant differences in mean values of Wt (p = 0.014), BMI (p = 0.04), WC (p = 0.03), FVC (p = 0.03), and FEV1 (p = 0.04) at the end of the study, but in favor of Group I.
Conclusions:
Utilizing the pulsed Nd:YAG HILT as an adjunctive therapeutic modality proved to be effective in improving the anthropometric indices and ventilatory functions in subjects with AO.
Introduction
Obesity is a global health problem associated with abnormal accumulation of body fat that results in impairment of an individual's health. 1 Abdominal obesity (AO) is the state of abnormal and excessive deposition of intra-abdominal fat 2 and is a rising and alarming problem among developed as well as developing societies. The abnormally accumulated abdominal fat in AO is an independent risk factor for cardiovascular disorders and all-cause mortality, 3 even more than generalized obesity. 4
The complex interactions of the abnormally increased intra-abdominal adipocytes, alongside their paracrine and endocrine functions, contribute to increased atherogenic and diabetogenic risks. 5 Majority of the stored excess fat in the state of AO is subcutaneous, while only a small percentage is stored as visceral fat. 6
Although general obesity is usually evaluated using the body–mass index (BMI) because it is an easy method and is closely correlated with obesity-related health hazards, 7 waist circumference (WC) is predominantly used as a measure of central obesity 8 because it is more accurate than BMI in evaluating AO where the anthropometric differences are of great importance and should be considered especially in subjects with Class I or II obesity. 9
Abnormally increased WC, the cornerstone factor in diagnosing AO, is a potent risk factor for serious health hazards. Increased WC values of more than 102 cm in men and more than 88 cm in women are indicative of a state of AO and highly associated with increased risk for cardiometabolic and cardiovascular disorders. 10 Increased BMI and WC values significantly contribute to the rising cases of metabolic syndrome, which is tightly correlated with a variety of cardiovascular disorders, 11 increased health costs, 12 and increasing rates of disability and mortality among subjects with obesity. 13
Disturbed pulmonary function (PF) is commonly encountered in patients with obesity, 14 and more impairments are clearly encountered in those with AO 15 since central obesity is more harmful to PF than overall obesity. 16 Abdominal fat disrupts the normal cephalic diaphragmatic excursion and therefore negatively affects lung volumes and capacities. 17 The PF should be considered when evaluating the impact of obesity on general health or when investigating the effect of a specified treatment on obesity. 18
Introducing laser therapy (LT) in the treatment of AO is not a new concern; low-level LT has yielded significant achievements in the treatment of localized obesity 18 and in reducing the WC in subjects with obesity. 19 LT proved to be an effective noninvasive therapeutic procedure for lysing excess fat in overweight and obese populations. 20 The high-intensity laser therapy (HILT) proved to be safe and effective in treatment of various health disorders such as osteoarthritis 21 and relief of postsurgical pain. 22
The higher irradiation dosage and penetration capacity of HILT can explain its better efficacy in treating different chronic conditions, so there is a growing interest in the use of HILT for treatment of a wider array of chronic disorders. 23 Laser, with its known obesity-counteracting effects, may assist in alleviating the obesity-related respiratory burden since weight change is usually associated with modulated lung volumes in health 24 and disease. 25
Although HILT has become the focus of recent years because of its higher intensity levels, more clinical studies are still warranted to clarify its effectiveness in various health situations 26 and across different age groups. 27 The effect of HILT in the treatment of AO has not yet been explored, so the objective of this study was to investigate effects of the pulsed Nd:YAG HILT on anthropometric variables and ventilatory functions in young adults with AO.
Materials and Methods
Study design and ethical approval
This 12-week study followed a single-blinded, randomized, placebo-controlled study design. This study was conducted in accordance with the principles of the 2013 version of the Declaration of Helsinki, approved by the Ethics Review Committee of the Faculty of Applied Medical Sciences, Umm Al-Qura University (Approval No. HAPO-02-K-012-2022-06-1138), and conducted at the Physical Therapy Department, Umm Al-Qura University, between May and September 2022.
A signed written informed consent was obtained from each participant at the beginning of the study, agreeing to participate and for publication of study results.
Study settings, participant recruitment, and randomization
The assessments and treatment methods utilized in this study followed standardized procedures. Interventions were conducted at the same time of the day, between 8 and 12 am, at an external temperature of 23°C. Instruments were periodically calibrated by the manufacturers to ensure result accuracy. To eliminate inter-rater variability, each variable was evaluated by the same assessor, and each treatment type was managed by the same therapist for all participants. All assessors and therapists were blinded to participant allocation throughout the study.
First, young adults with AO were invited to participate in this study. All subjects were initially screened by the same physician to confirm eligibility according to inclusion and exclusion criteria.
Second, a suitable sample size was initially determined using the G-Power program for Windows, GPowerWin_3.1.9.4 (
Forty-five, healthy, sedentary volunteer men with AO were eligible for enrollment in this study. Five subjects were initially withdrawn because of their inability to adhere to the scheduled study meetings and treatment sessions. Three subjects were excluded at the initial screening because they participated in another obesity treatment program.
Third, the remaining eligible thirty-seven participants were allocated using a simple random number allocation method to the Nd:YAG HILT group (Group I; n = 19) or placebo Nd:YAG HILT group (Group II; n = 18), using sealed envelopes prepared by an independent subject (with no other role in the study) who initially recorded the eligible participants and randomly encoded them with random numbers, each of which was secured in a closed envelope containing the name and number generated for the participant.
Random group allocation was then performed using the Random Number Generator program (
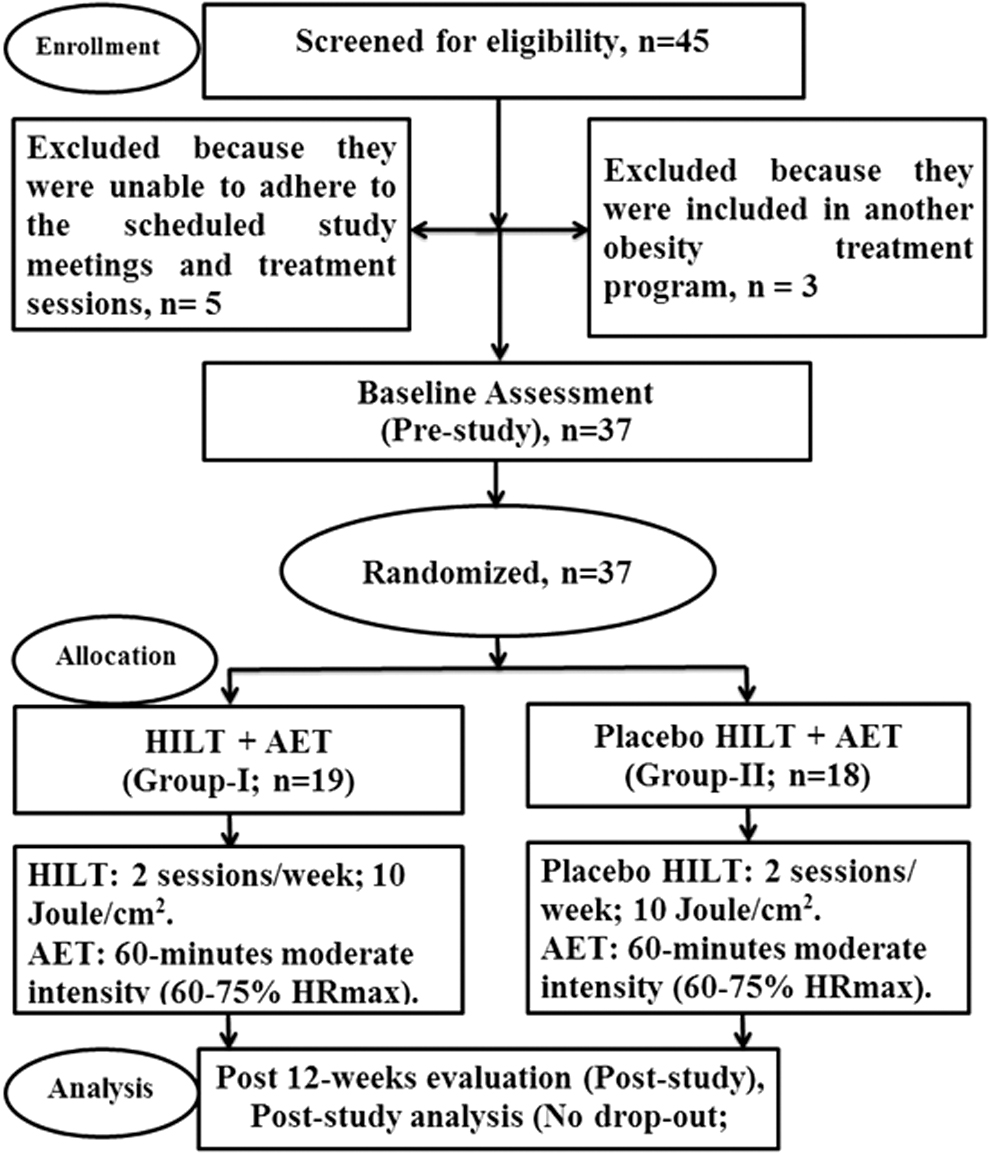
Patient's flowchart.
Inclusion and exclusion criteria
Nonsmoker young adult men aged 19–25 years, with BMI >30 kg/m2, WC >102 cm, and a sedentary lifestyle, and who are free of serious pulmonary, metabolic, or cardiovascular disorders were included in this study. Subjects were initially excluded if they refused to sign the informed consent or had BMI <30 kg/m2, WC <102 cm, or current or previous involvement in any obesity management program within the last 6 months.
Assessment and data collection
All participants underwent the same evaluation procedures. Data were collected using standard laboratory procedures. Variables were evaluated prestudy (Evaluation 1) and poststudy (Evaluation 2). Prestudy assessments were done 1 day before the first treatment session, and poststudy assessments were conducted 3 days after the last treatment session to avoid acute post-treatment effects.
Body weight, BMI, and WC assessment
The body Wt, to the nearest 0.1 kg, and standing height (Ht), to the nearest 0.01 m, were evaluated using a scale (Detecto's ProMed scale, USA). BMI was calculated as BMI (kg/m2) = Wt (kg)/Ht 2 (m). The subject's WC in cm was measured while standing, using a nonstretchable tape (Richter Measuring Tape; Seca Ltd., Germany), after normal exhalation at the point midway between the lower rib and the iliac crest, following a previously applied technique. 28
Ventilatory function assessment
After a 10-min rest, ventilatory functions were evaluated according to a previously published procedure. 29 The forced vital capacity (FVC) and forced expiratory volume in 1 sec (FEV1) were evaluated by performing maximal inhalation, followed by forced maximal prolonged exhalation, while standing using a portable computerized spirometer (Spirolab III Computerized Portable Spirometer MIR-Medical International Research, Inc., USA), which was regularly autocalibrated.
Evaluation steps were clearly explained before the test and maximum effort was emphasized while performing the test; three attempts were allowed, but only the best attempt's value was considered for statistical analysis.
Treatment protocols
Participants in Group I received the Nd:YAG HILT plus moderate-intensity aerobic exercise training (AET) program, while Group II participants received placebo Nd:YAG HILT plus the same AET program. All participants were directed to continue their normal dietary pattern and level of daily activities throughout the study.
A preliminary educational session was conducted for all participants regarding the AET treadmill walking protocol and safety measures.
AET program
All participants in both groups completed 12 weeks of a supervised, moderate-intensity, AET treadmill walking program (COSMED T150LC Treadmill, Italy) for 3 sessions/week. Each session included a 5–10-min warmup followed by 5–10-min cool down in the form of low-intensity pace walking (30–40% of predicted maximum heart rate, HRmax, calculated using the equation by Tanaka et al. [predicted HRmax = (208–0.7 × age)], 30 keeping the rate of perceived exertion at 10–12 on Borg's dyspnea scale during the warmup and cooling down periods.
After the warmup, each participant underwent a closely supervised moderate-intensity AET program for additional 60 min, on the “day after day” schedule, between 8 and 12 am. The AET intensity range was continuously maintained [at 60–75% (208–0.7 × age)] and continuously controlled by monitoring the subject's heart rate during training using a pulse oximeter device (Model: CMS50DL, China) that was secured on the subject's thumb throughout the AET session.
The AET program intensity started with 60% HRmax and then was modulated to follow a stepwise increase of 5% every 3 weeks, reaching 75% HRmax in the last 3 weeks. Subjects were continuously directed to maintain their rate of perceived exertion between 12 and 14 on Borg's dyspnea scale during the AET sessions. No serious events were recorded throughout the study.
The Nd:YAG HILT program (for Group I)
Participants in Group I received pulsed Nd:YAG HILT using the HIRO-3 apparatus (HIRO 3 ASA, Italy) that was regularly calibrated by the manufacturer throughout the study. Both the therapist and participant wear the manufacturer-provided protective eyeglasses during the Nd:YAG HILT sessions.
The abdominal area to be irradiated with the Nd:YAG HILT beam was regularly cleaned before Nd:YAG HILT application and carefully demarcated while the participant assumed a relaxed, supine lying position. The abdominal area to be treated was the whole area bordered by two horizontal and two vertical lines; the superior horizontal line extended between the lowermost points of the 10th ribs (10th costal cartilages) on the anterior chest wall and the inferior horizontal line extended between the anterior superior iliac spine (ASIS) points.
Each vertical line extended between the ASIS, inferiorly, till the lowermost point of the 10th ribs (10th costal cartilages), superiorly. This demarcation created a regular shaped area so that the abdominal surface area to be irradiated with the Nd:YAG HILT (A, in cm2) was then calculated for each participant.
Participants in Group I received pulsed Nd:YAG HILT (1064 nm wavelength, 10–30 Hz frequency, 510–1780 mJ/cm2 fluency levels, 10.5 W average power, 120–150 μsec pulse duration, a 0.1% duty cycle, and 0.2 cm2 spot size) for 24 sessions (12 consecutive weeks) during nonexercise training days, with an average fluency of 15 J/cm2. The total HILT energy in Joules was calculated depending on the total abdominal surface area to be irradiated (A, in cm2) [total Nd:YAG laser energy dosage = average fluency (joule/cm2) × surface area (A; cm2)].
After calculating the total Nd:YAG laser energy dosage, the therapist held the Hiro-3 handpiece perpendicularly in contact with the participant's abdominal skin while the participant assumed a comfortable, supine lying position and was wearing protective eyeglasses. Treatment was applied in two phases with equal doses; the first initial phase was in the form of fast manual scanning, while the second final phase was in the form of slow manual scanning. Scanning was applied both in horizontal (from side to side) and vertical (upward–downward, and vice versa) directions.
The placebo Nd:YAG HILT program (for Group II)
Participants in Group II followed the same protocol as that in Group I, except that the start button for the laser beam was turned off during the treatment.
Statistical analysis
Data analysis was performed using the SPSS package, version 20 (SPSS, Inc., Chicago, IL, USA). Data are presented as mean and standard deviation. Mean changes within and between groups were tested using one-way analysis of variance (ANOVA). The percentage of change in each evaluated variable was also calculated. The level of significance was set at p < 0.05.
Results
Between-group comparisons
At Evaluation-1, there were nonsignificant differences between groups in the baseline demographic characteristics. In addition, there were nonsignificant differences between groups in the mean values of Wt (p = 0.55), BMI (p = 0.16), WC (p = 0.97), FEV1 (p = 0.83), and FVC (p = 0.54). Poststudy results at Evaluation-2 showed that there were significant differences between groups in the mean values of Wt (p = 0. 01), BMI (p = 0.04), WC (p = 0.03), FEV1 (p = 0.04), and FVC (p = 0.03) (Tables 1 and 2).
Between-Group Comparison of Demographic Characteristics and Anthropometric Obesity Index Variables
HILT, high-intensity laser therapy.
Significant; **nonsignificant.
Between-Group Comparison of Ventilatory Function Variables
FEV1, forced expiratory volume in 1 sec; FVC, forced vital capacity.
Significant; **nonsignificant.
Within-group comparisons
At Evaluation-2, there were significant decreases in Wt (p = 4.39–14), BMI (p = 8.34–16), and WC (p = 2.7–18) in Group I, by 6.14%, 6.14%, and 3.78%, respectively, while in Group II, there were significant decreases in Wt (p = 1.45−11), BMI (p = 3.43−11), and WC (p = 1.58−13), by 4.29%, 4.24%, and 1.74%, respectively (Table 1).
At Evaluation-2, there were significant increases in the FEV1 (p = 2.61−9) and FVC (p = 2.68−7) in Group I, by 16.4% and 13.6%, respectively, while there were significant increases in the FEV1 (p = 1.64−9) and FVC (p = 0.001) in Group II, by 8.8% and 5.89%, respectively (Table 2).
Discussion
This study evaluated the effectiveness of the 12-week Nd:YAG HILT program on anthropometric indices and ventilatory functions in young adult men with AO.
There is a strong negative correlation between PFs and body fatness, with the most obvious biochemical and mechanical pulmonary impairments seen in AO. 31 Results of this study clarified that Nd:YAG HILT significantly improved the anthropometric and ventilatory function variables when used as an adjunctive therapeutic modality in the treatment of AO.
Exercise therapy is an important therapeutic option for subjects with AO. AET is a powerful procedure for enhancing the rate of body fat loss, 32 with the response to the prescribed exercise training program being dose dependent. 33
Significant achievements in health benefits can be obtained through involvement in a moderate-intensity exercise training program for at least 150-min/week, even without dietary restriction. 34 Moderate-intensity AET was chosen because of its proven effectiveness in maximizing oxidation of the skeletal muscle fat content and hence increasing the rate of fat loss. 35 The moderate AET intensity, with a stepwise increase of 5% every 2 weeks in the training intensity, was chosen because it proved to be an effective strategy in the treatment of obese patients. 36
Quite recently, HILT has been utilized as a therapeutic modality. Although many studies have been published on the effects of LT on different health aspects, studies reporting effects of HILT on health aspects are still limited, so lack of standard therapeutic protocols, definite case-related therapeutic dose, application time (duration), and detailed application steps are among the most commonly encountered limitations when utilizing HILT as a therapeutic modality. 37
Effects of the HILT can be attributed to its intense and deeper effects, 38 making it effective in controlling manifestations encountered in many chronic disorders. 21,39,40 The HILT works with high peak power that is able to stimulate deep tissues and organs that are difficult to reach by other therapeutic modalities. 41
Significant effects produced by the HILT can be attributed to the unique characteristics of the HILT and its capability to produce a photomechanical effect that can, alone or in combination with other known photochemical and photothermal effects, 42 produce extraordinary therapeutic effects. 39 Application of HILT, with its very short pulse duration and very high pulse intensity, can successfully trigger vascular and lymphatic system activation 43 as well as stimulation of several metabolic processes. 44
The obvious WC reduction in response to the HILT program was supported by McRae and Boris, who reported significant WC reduction in response to a 2-week diode LT program, 45 and by Roche et al., who reported safety and significant reductions in the thigh, hip, and abdominal circumferences in response to the low-level LT in obese subjects. 19
The synchronized application of LT and exercise training is an effective, noninvasive, nonpharmacological treatment option not only for obesity management but also to control obesity-related comorbidities. 27,46 More significant positive results obtained in the active LT group can be attributed to the combined AET and laser-based effects on the oxidative metabolic activities, which increase the lipolytic activity even from the first session. 47
There is more intense activation of lipid-hydrolyzing enzymes and lipid-targeting hormones when LT is combined with exercise training, 48 which in turn magnifies the oxidative capacity process and the rate of fatty acid uptake through the beta-oxidation gateway, resulting in significant depletion in the adipose tissue reserve and alterations in anthropometric variables. 49,50
The pronounced changes in anthropometric indices in response to LT can be also attributed to the lipid oxidation-augmenting effects either intracellularly, through assisting in triglyceride breakdown into glycerol and fatty acids by the activated cytoplasmic lipase enzyme, 51 or extracellularly, through increasing the adipocyte membrane permeability of intracellular lipids to extracellular spaces, 52 to facilitate their oxidation. 53
Local laser application is not only associated with localized responses but it also potentiates generalized modulation in enzymes and body responses far away from the laser application site, which can explain the favorable body system responses to laser application especially when accompanied with exercise training in obese subjects. 54
Increased abdominal fat impairs the ribcage and lung compliance and adds mechanical stress on the respiratory muscles and constraints on the pulmonary structures, 14 in addition to the persisted systemic inflammatory status. 55 Ameliorating these stresses and constraints through exercise training 35 and LT, 19 or their combination, can improve the normal pulmonary mechanics and functions by reduction in the body weight and BMI 56 since lung volumes and respiratory muscle strength are positively correlated with the amount of weight loss in obese subjects. 57
Although the results of this study have practical importance, the short study duration, limited sample size, and inclusion only of men participants in this study should be considered during the generalization of its results. Efforts were made to avoid bias. Patient randomization, group allocation, and assessment processes were performed blindly, but it was a hard task to blind the therapist to the type of applied therapy. Further studies in the field of HILT are still required to resolve these limitations.
Conclusions
Based on results of this study, Nd:YAG HILT can be utilized as an effective, adjunctive therapeutic tool in the treatment of AO. The Nd:YAG HILT proved to be an effective therapeutic modality that can positively modulate anthropometric indices and ventilatory functions in young adults with AO.
Footnotes
Acknowledgments
The author appreciates the nonauthorship participation and support of Dr. Mohamed Salaheldien Mohamed Alayat and Dr. Ehab Abdelkafy in conducting this study, supervising patients' performance, allocating participants into random groups, and recording of results.
Author's Contribution
A.A.M.A. contributed significantly toward the research in this study. The author takes responsibility for conceptualization, methodology, validation, formal analysis, investigation, data curation, article writing, and final draft approval, in addition to oversight and leadership for the research activity planning and execution.
Ethical Statement
The author declares that all assessments and therapeutic procedures applied on human subjects were conducted in accordance with the Declaration of Helsinki (
Disclaimer
The author declares that the article, including related data, figures, and tables, has not been previously published and that the article is not under consideration elsewhere.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.