
Abstract
Venous malformation is acongenital vascular system structure malformation caused by abnormal vascular endothelial cell morphology, which can occur in any tissue or organ of the oral and maxillofacial region. Laser treatment is currently a commonly used minimally invasive treatment. In this case, the patient with congenital multiple venous malformation was treated with Nd:YAG laser for the visible submucosal part, and the subcutaneous part under the chin tip was treated with ultrasound. The chin tip was treated with ultrasound guided by the chair to achieve the purpose of minimally invasive laser treatment. In this case’s diagnosis and treatment process, we hope to provide a new idea for laser treatment of oromaxillofacial vein malformations.
Introduction
Venous malformation (VM) is a kind of congenital structural malformation of the vascular system due to abnormal vascular endothelial cell morphology, 1 which can occur in any tissue or organ of the oromaxillofacial region. Most of them are detected in infancy, and if there is no intervention treatment, they will be migrated to become more significant with growth and development. When the body’s immune system is low or complicated with infections, the lesion often manifests as swelling and pain in the focal area and even deformity and dysfunction in the affected part. 2 Oral and maxillofacial VM treatment currently includes sclerotherapy, surgical resection, laser intervention, and other modalities. 3 Literature 4,5 results show that in the first surgical resection, it is difficult to avoid the risk of trauma and bleeding. Second, local injection sclerotic therapy is difficult to accurately control because of the dose of the drug and the quantitative and qualitative effect relationship between the diseased tissues, and local necrosis of the tissues and other side effects are often seen. In recent years, Nd:YAG laser can selectively and accurately treat VM lesions through unique photothermal and biological effects and minimally invasive treatment, and at the same time, it can significantly reduce postoperative complications such as postoperative swelling and pain in soft tissues in the operated area. 2 It has gradually become one of the hotspots for the clinical treatment of superficial oral and maxillofacial VM.
Medical Records
The patient, a female, 30 years old, presented to the Department of Stomatology, Air Force Specialty Medical Center, on August 18, 2022, with the chief complaint of “scattered dark purple lumps on the lips, tongue, and chin for 30 years with progressive enlargement.” After birth, the patient was found to have dark purple bump-like changes in the tongue, lip, and cheek mucosal tissues in the mouth. In addition, in recent years, the swelling under the chin has been raised, accompanied by swelling and discomfort, which affects facial esthetics.
Specialized examination
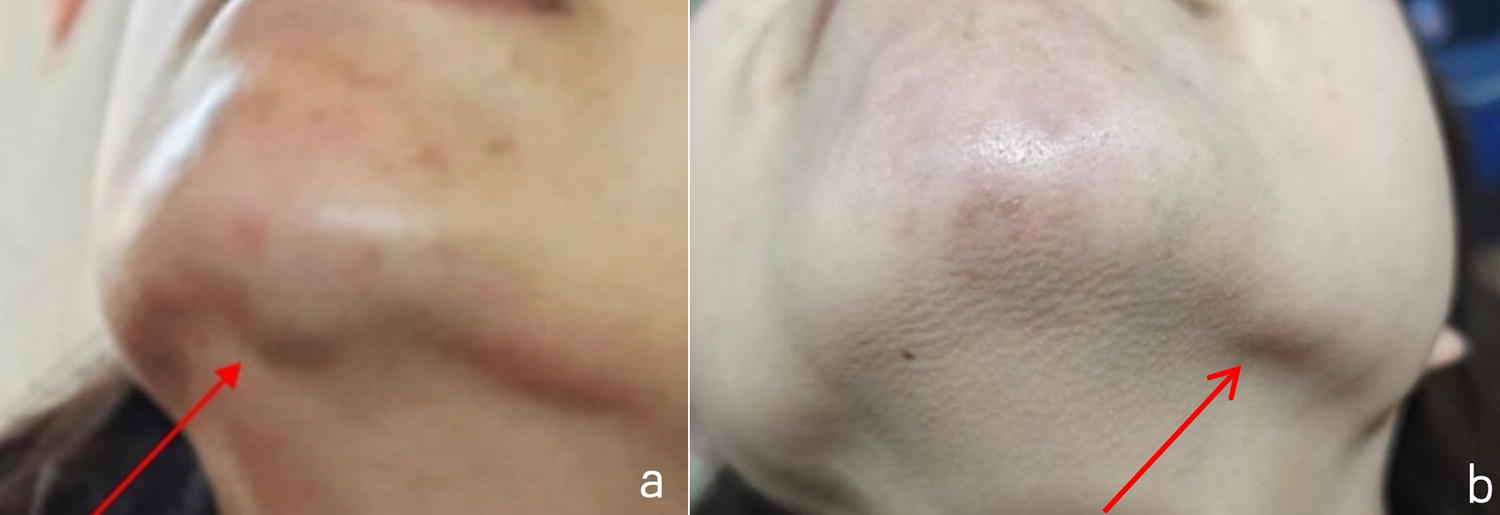
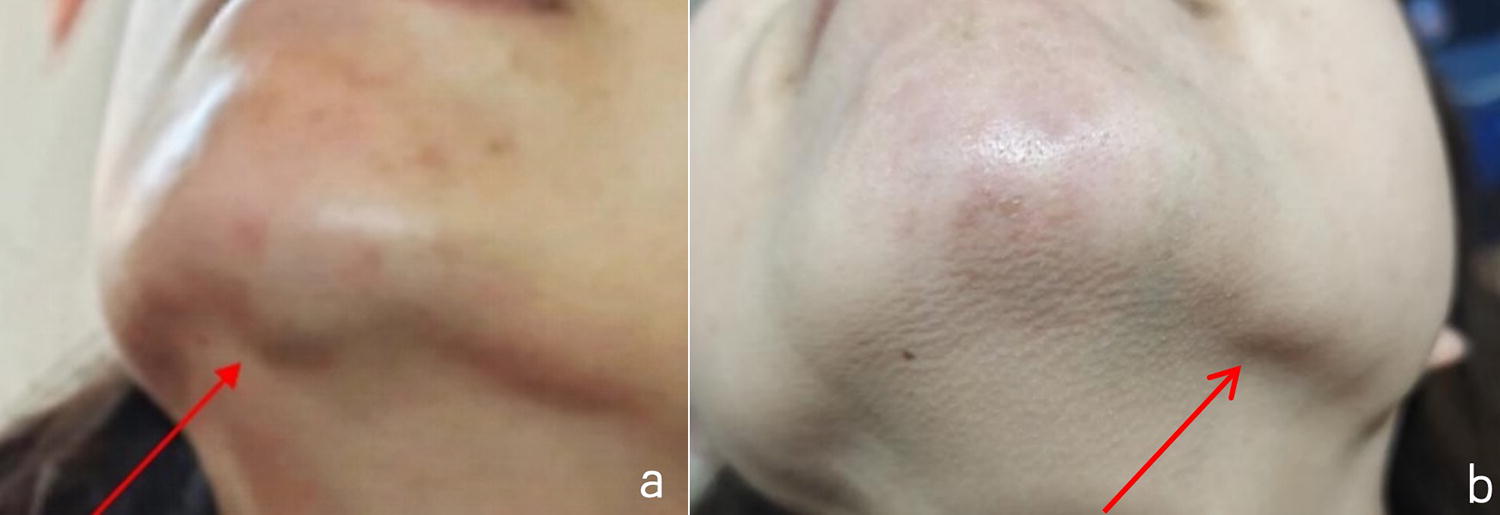
A dark purple raised mucosal mass on the left side of the lower lip, surface area, 10 × 20 mm, extending intermittently into the mouth to the mucosa of the vestibular region, with a clear border and irregular margins. A translucent fluid-like protuberance of 1 × 2 mm with well-defined borders is visible under the mucosa in the region of the vestibular mass, which is considered secondary to the retention of secretions from the mucous glands. The tongue’s ventral and lateral margins and the tongue’s dorsum near the root of the tongue showed a large scattered dark purple mass with a clear boundary and soft texture and no sign of pressure and pain (Fig. 1). The skin contour under the right side of the chin is slightly raised. The skin was vaguely bluish, with unclear borders, soft to touch, and tender to palpation (-). After instructing the patient to bend low for 30 sec, the skin contour of the lesion in the under-chin area became more pronounced (Fig. 2a). The patient denied having systemic systemic disease and had no family history of disease.

Preoperative intraoral situation with invasion of the vestibular mucosa visible at the point indicated by the arrows.
Imaging
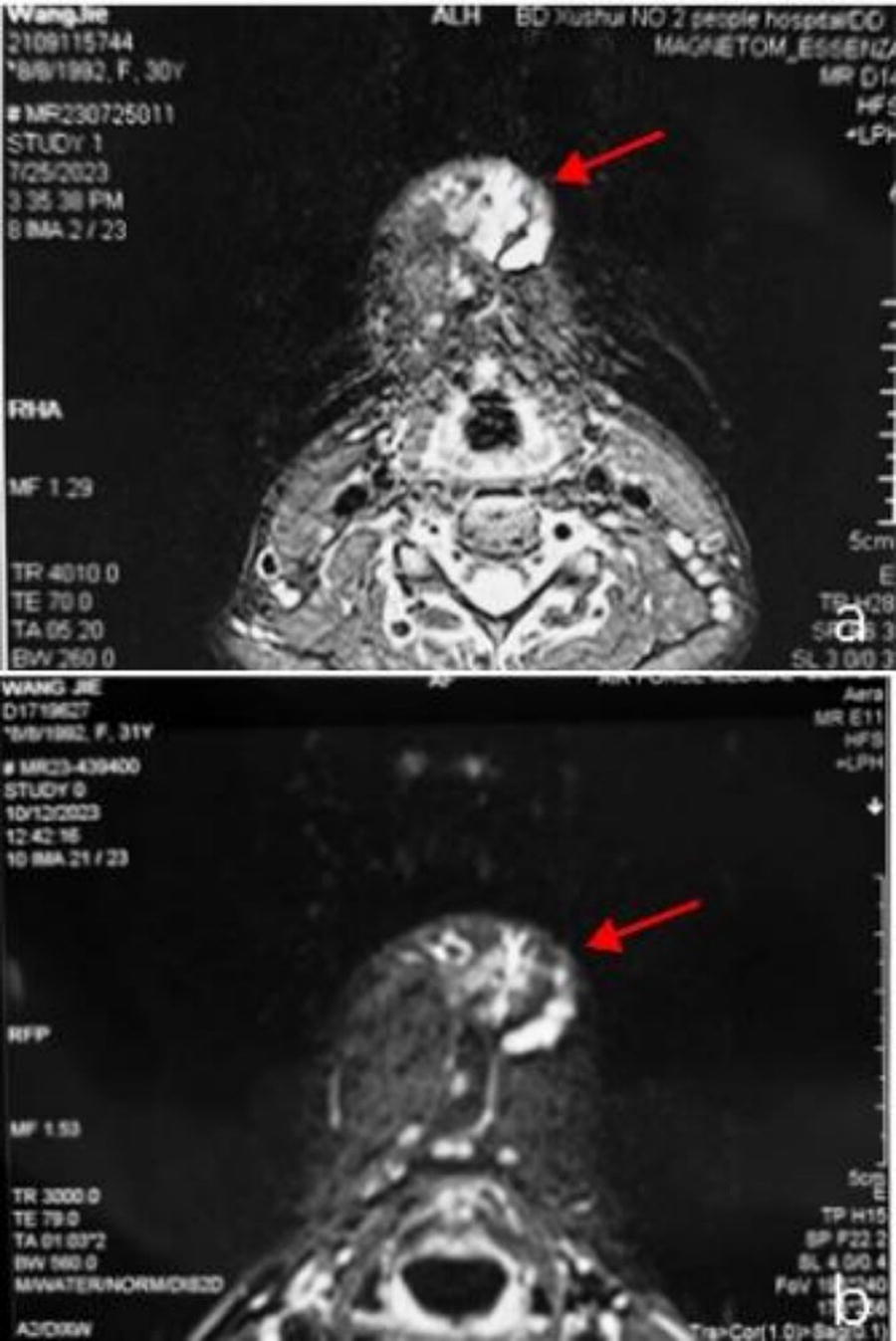
Color Doppler acoustic diagnostic instrument (Philips EPIQ7, USA) showed a cystic elevated echogenic area on the tongue’s left side and lower lip. A liquid dark area was seen under the skin under the chin, the translucency of which was still apparent, and obvious deformation was seen when the probe was lightly pressed; color Doppler showed that there was abundant blood flow in it, and spectral Doppler showed that it showed a venous blood flow spectrum (Fig. 3a). Oral Cone-beam computed tomography (CT; Kawasaki I CAT, Germany) showed that the mandibular margins were intact, and no erosion of the cortical bone surface was observed (Fig. 4). Magnetic resonance imaging (MRI, Siemens MAGNETOM Area 1.5T, Germany) showed that the mandibular sweep and range of the bone did not show any abnormal change. The subcutaneous soft tissues under the chin and anterior to the mandible showed multiple irregularly shaped abnormal signals, with a low signal in T1WI and a high signal in T2 pressure lipids, with uneven signals (Fig. 5a).


CBCT shows no bone defect in the mandible. CBCT, cone-beam computed tomography.
Clinical diagnosis
VM of the submucosal tissue of the lip and tongue (multi-focal spots). VM of subcutaneous tissue in the under-chin region. Mucinous cyst of the lower lip mucosa.
Treatment steps
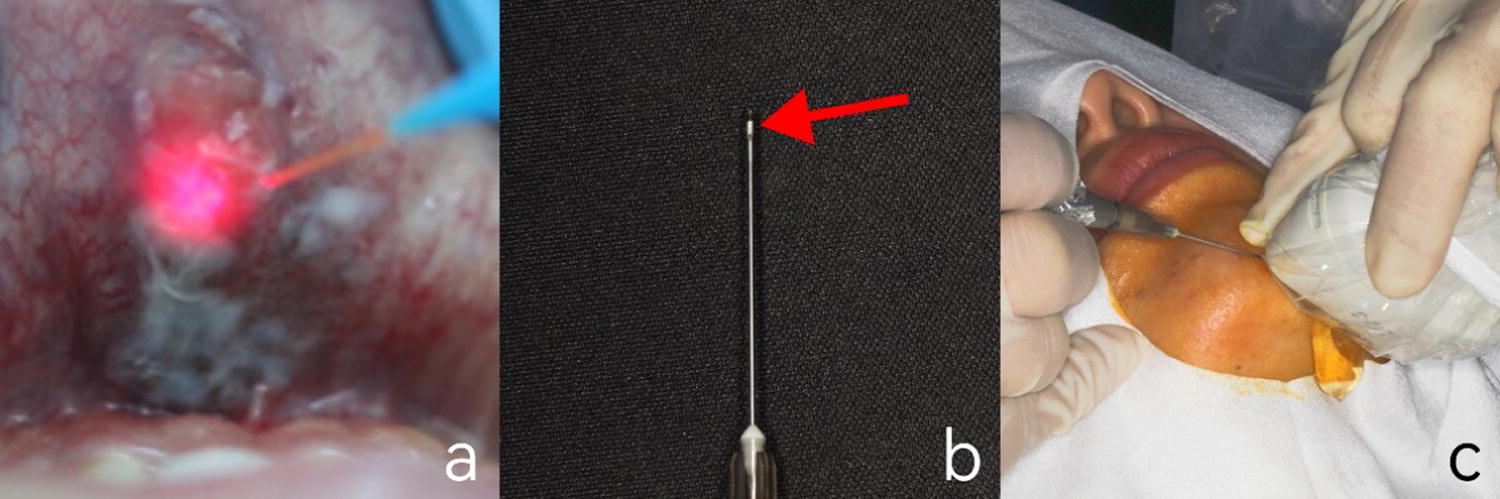
In this case, Nd:YAG laser noncontact, sequential treatment of focal submucosal tissue of the lower lip and tongue. Treatment date: August 28, 2023. Treatment process: the oromaxillofacial and intraoral iodine disinfection, 1 mL ativicaine local infiltration anesthesia. First, the laser treatment VM mode parameters were matched (Table 1, frequency 20 Hz, average power of 6 W, pulse width of 200 ms, and the diameter of the optical fiber 300 μm). The fiber optic tip is kept 1 mm away from the surface of the tumor body and starts to stimulate the laser instrument, and then the fiber optic tip moves at a speed of 2 mm/sec. The laser fiber movement irradiation to the treatment area of the tumor color was white, and the volume no longer changed. Then, the Nd:YAG laser was stopped. The assistant held a frozen wet swab to follow the fiber optic moving path, placed it in the whitened treatment area for 30 sec, and then removed it, which immediately lowered the local temperature and prevented the occurrence of thermal injuries. Next, the Nd:YAG laser photobiomodulation therapy (PBMT) mode parameters (frequency 15 Hz, average power 1.5 W, pulse width 100 ms, and 300 um fiber) were selected. The laser fiber tip maintains the distance from the surface of the tumor by 1 mm, and the hand with the fiber tip moves, keeping the speed of 1 mm/sec. The mucosal irradiation of the VM lesion area was performed for about 2 min, and the operation was completed (Fig. 6a). Parameters of Laser Therapy PBMT, photobiomodulation therapy; VM, venous malformation.
Recovery 12 weeks after treatment: clear cysts can be seen at the marks as mucous gland cysts.
Ultrasound-guided, Nd:YAG laser fiber optic interventional, sequential treatment of subcutaneous VM in the under-chin region of the case. Treatment date: October 8, 2023. Treatment process: oromaxillofacial and intraoral iodine disinfection, 1.7 mL ativicaine local infiltration anesthesia. First, the VM mode parameters of the laser treatment were matched. The Nd:YAG laser fiber tip is sterilized with iodine, built-in set in the 5 mm syringe needle, and the laser fiber tip and syringe fiber tip can be kept at the same level (Fig. 7b) (Fig. 6b). After the ultrasound probe is sterilized with iodine, the ultrasound technician operates the ultrasound probe to probe the specific site of the patient’s VM lesion under the chin. The dentist holds the cannula device containing the Nd:YAG laser fiber tip and syringe to make the cannula tip puncture the skin of the under-chin area in the direction parallel to the direction of the ultrasound probe and then enter into the VM lesion tissues (Fig. 7c) (Fig. 6c). The shape and specific location of the puncture needle with high signal in the lesion can be seen on the ultrasound screen (Fig. 8a). Guided by the ultrasound screen under direct vision, the dentist accurately places the fiber optic head and syringe cannula device into the distal region of the VM lesion and begins to excite the Nd:YAG laser. The instantaneous vaporization of the lesion into a blurred hypoechoic image can be seen on the ultrasound screen after laser irradiation (Fig. 8a). The fiber optic tip was moved uniformly from the distal end of the VM lesion to the proximal end while irradiating the movement speed at 1 mm/sec. The ultrasound screen showed no apparent blood flow in the lesion, and the laser was stopped. The fiber optic tip and the syringe cannula device were extracted from the subcutis. The assistant held a frozen wet cotton swab on the skin surface and immediately followed the trajectory of the fiber optic tip, placing it sequentially on the irradiated area of the skin surface for 30 sec. Afterward, the assistant used gauze to compress the gauze at the skin site of the puncture point for 1 min to stop the hemorrhage. Then the Nd:YAG laser PBMT mode parameters were selected: the laser fiber tip to maintain a distance of 1 mm from the skin surface of the lesion under the chin, the speed of movement of the fiber optic tip of the hand to maintain a 1 mm/sec, and noncontact uniform speed of laser irradiation of the skin outside the under-the-chin VM lesion surgical area. The irradiated area was finished after 5 min (Fig. 8b).


Postoperative 4 weeks’ clinical visit: the patient consciously had no pain and swelling in the operated area. Specialized examination: there was no bulge-like change in the VM lesion area of the skin under the chin, and the color, texture, and morphology of the local skin returned to normal, with no keloid-like change (Fig. 9) (Fig. 2b). Ultrasonography: the fuzzy hypoechoic image of the mucosal area of the mouth had become significantly lighter and was close to normal tissues (Fig. 3b). MRI: subcutaneous soft tissues under the chin and anterior mandible showed thin strips of long T2 signals with clear borders (Fig. 5b). On follow-up 12 weeks after surgery, there was no swelling or discomfort in the soft tissues of the VM lesion area under the chin, and the patient was delighted with the results of the laser treatment.
Postoperative intraoral condition.
Discussion
Oral and maxillofacial VMs may involve single or multiple tissues, organs, and bones. Thrombosis within the VM can trigger an inflammatory response, with the primary syndromes being recurrent, chronic pain, and a swelling response in the tissues adjacent to the lesion. 6 Oral mucosal VM can be roughly diagnosed based on clinical manifestations alone. However, some subcutaneous VM lesions in the oromaxillofacial region are not visible to the naked eye and may contain phleboliths, which should be differentiated and diagnosed from maxillofacial tumors, lymphatic malformations, and salivary gland stone disease based on clinical manifestations and imaging examinations such as ultrasound, CT, and MRI. 7,8
In the oral and maxillofacial VM ultrasound examination, the vascular lumen will be deformed after the probe squeezes the lesion site, increasing blood flow signals, which has become prevalent in the adjunctive diagnosis of superficial vascular diseases in the head and neck region. In this case, ultrasound was also chosen to examine the VM lesion area first, and the results showed that there was abundant blood flow in the area, which was consistent with the typical features of VM ultrasound imaging. 9 Due to the wide range of lesions in this case and involving the deep subcutaneous tissues of the chin, ultrasound alone could not accurately detect the depth and extent of the lesion area. MRI has no ionizing radiation, and three-dimensional reconstruction tomography can quantify the image data, which is used to localize deep soft tissue lesions more accurately than ultrasound. It is considered the gold standard of auxiliary imaging for diagnosing VM. 10,11 Therefore, in this case, we applied for a preoperative MRI examination of the VM lesion.
The Nd:YAG laser is one of the mainstays of clinical practice for the precise and minimally invasive treatment of oral and maxillofacial hemangiomas. This is due to its selective absorption by the hemoglobin and melanin components of the tissue it acts on. Laser light energy can be converted into heat energy, and direct thermal radiation on the endothelial lining of the malformed blood vessels of the VM causes the tumor to rapidly coagulate and then shrink, which is gradually metabolized and absorbed by the body. 12 In this case, when completing the noncontact or interventional treatment of the VM lesion with the Nd:YAG laser, at the same time, the physical cooling of soft tissues of the operated area with ice cotton was carried out to minimize the complications of thermal damage caused by the Nd:YAG laser. In addition, the PBMT mode of Nd:YAG laser is based on photobiological effect, light energy in the state of nonphotothermal effect, at the cellular and molecular levels on the acted tissues, which can promote wound healing in the operation area and play a role in reducing the inflammatory effect to relieve pain. 13,14 Therefore, in this case, applying Nd:YAG laser thermal and biological effect sequences to treat VM lesions can effectively reduce the signs of soft tissue hemorrhage, edema, or ulceration in the operated area and alleviate the pain symptoms in the operated area. In addition, based on the accumulation of clinical laser interventional therapy for VM cases in the previous period of our group, the parameters of laser pulse width, average power, and laser irradiation time were thus determined. 15
The efficacy of Nd:YAG laser on superficial venous malformations has been clinically verified, but for deep skin or submucosal lesions, most of the laser energy has been absorbed by the superficial skin or mucosa at the early stage of irradiation, resulting in insufficient penetration of the laser beam to the lesion tissues. Increasing the power will make the covering epidermis absorb too much heat energy converted to light energy, and the local tissues will be severely burned due to coagulation or carbonization, quickly leaving scars after healing. 16 Therefore, the laser can be exposed through the fiber delivery system directly on the thick and deep lesion tissue for the deep venous malformation lesion tissue. On the one hand, it can maximize the laser on the deep lesion tissue contact with the maximum thermal result of therapeutic effect. On the other hand, direct contact between the laser and the skin, mucosal surface, and other parts can be avoided, minimizing side effects such as epithelial tissue damage. 17,18
In this case, the lesion in the under-chin area was located in the subcutaneous area. If a clinician unthinkingly performs a puncture based only on operational experience and preoperative imaging references, problems such as incorrect or skewed needle entry points can quickly occur. These problems often result in poor laser irradiation, damage to adjacent typical tissue structures, and missed treatment of the VM lesion area. In addition, since interventional therapy is a blind procedure, excessive laser irradiation can cause a large amount of thermal energy converted from light energy to accumulate in the lesion area contacted around the fiber optic tip, resulting in localized necrosis of the lesion tissue, whereas normal or low-dose irradiation is not therapeutically effective for the lesion tissue. 18 Therefore, the surgery was carried out in this case by visualizing the image with ultrasound guidance. The irradiation position could be dynamically positioned, the laser irradiation point and irradiation time could be adjusted, and the Nd:YAG irradiation could be stopped immediately after the disappearance of the colored blood flow signals in the lesion and the change of the local lesion into a fuzzy hypoechoic image, thus completing the Nd:YAG laser interventional therapy procedure. 19,20 Regular postoperative follow-up, ultrasound, and MRI examinations were performed, and a quantitative assessment of the curative effect of VM could be accomplished by comparing the preoperative and postoperative imaging data and combining them with specialized clinical examinations.
In summary, ultrasound-guided Nd:YAG laser intervention is used to treat oral and maxillofacial VM, and the lesions in the operative area can be imaged with a clear field of view. The intraoperative ultrasound instrument guided the laser fiber irradiation in real time, significantly improving the subcutaneous puncture’s accuracy and effectiveness for treating VM lesions. However, ultrasound-guided fiber-optic laser intervention for oral and maxillofacial VM is a new treatment mode. This treatment protocol needs the corresponding operation specifications and expert consensus standards and requires the accumulation of more experience in laser intervention for oral and maxillofacial VM cases. In addition, due to the diversity of clinical manifestations, locations, and extent of involvement of VM, we need to be prepared to provide individualized treatment plans. For example, the mucous gland cyst of the lower lip, in this case, can be excised with the Er:YAG laser. If scarring or hyperpigmentation occurs, it is necessary to consider combining traditional local surgery or Er:YAG laser excision with other combined treatment options.
Footnotes
Authors’ Contributions
J.J.: Writing—original draft, validation, conceptualization, resources, visualization, data curation, and investigation. M.F.: Investigation, data curation, and visualization. J.L.: Visualization. P.W.: Methodology and formal analysis. W.W.: Software and resources. B.M.: Methodology and term. H.L.: Funding acquisition, writing—reviewing and editing, supervision, resources, and project administration
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
Air Force Equipment Comprehensive Research Program (KJ2023B01097).
Supplementary Material
Supplementary Video S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.