
Abstract
Purpose:
The study’s main objective was to assess the efficacy and safety of TANIT, a platform combining functional dermal stimulation with damped bioactive current and mechanical stimulation to reduce adipose tissue (AT) in patients with stage I (SI) or II (SII) lipedema.
Methods:
A single-center, before–after clinical trial without a control group was conducted on adult women diagnosed with SI or SII lipedema. Patients underwent a treatment protocol for 5 weeks, with weekly sessions. Blood tests, AT thickness, pain threshold, and anthropometric measurements were assessed at baseline and the end of the study, and a satisfaction survey was conducted after treatment.
Results:
Twenty-three women were enrolled with a mean age of 44.91 (standard deviation 11.58) and a median of 46.00 (Q25 = 36.50, Q75 = 51.50). Seven (30.4%) patients had SI lipedema and 16 (69.6%) had SII. The pain threshold increased in 78.3% of patients at the knee level and 80.0% at the ankle level. Lower limb volume decreased in 78.3% of patients. AT thickness decreased in all treated areas, with a mean decrease of 26.1% at the ankles, 14.5% at the knees, and 17.4% at the trochanter level. Patients reported high satisfaction with the results obtained after the treatment sessions, and no unexpected adverse effects were found.
Conclusions:
The TANIT platform provided an effective and safe conservative treatment option for patients with S and SII lipedema, reducing leg volume, AT thickness, and pain. However, additional randomized clinical trials and standardized assessment tools would be necessary.
Introduction
Lipohyperplasia dolorosa, or lipedema, is a little-known adipofascial disorder that symmetrically affects the distribution of adipose tissue (AT), mainly in the lower extremities, and almost exclusively affects women. 1 In 2018, the World Health Organization recognized lipedema as a disease, defining it as a nonpitting diffuse “fatty” swelling, usually confined to the legs, thighs, hips, and upper arms. 2 Lipedema is associated with adipocyte hypertrophy that progresses with the disease stage, interstitial fibrosis that worsens as the stage advances, and an increased proportion of M2-like macrophages. 3 The estimated prevalence of lipedema is 10%, 4 although epidemiological data are scarce, heterogeneous, and vary among publications. 2 In Spain, the only registry conducted to date reported a prevalence of 18.8%. 5
Lipedema has three main components: hereditary, with evidence of familial involvement, 6 estrogenic, and inflammatory, 4 which differs from primary obesity. 3 Pain, as the main symptom of lipedema in approximately 70% of cases, 2 can have far-reaching implications as a physical deterioration that can eventually even affect patients’ health, basic mobility, and the ability to perform physical activity. 7
The etiology and pathophysiology of lipedema are unknown and the diagnosis is essentially clinical. 5 Differential diagnosis includes obesity, lymphedema, or lipohypertrophy. 4,8 Lipedema is classified into four stages 9 –11 and based on the anatomical location of fat distribution, it is classified into four types. 12,13
The most widespread treatment for stage I (SI; skin with normal appearance, smooth to palpation, with nodules that may be palpable and may be associated with pain or easy bruising) and stage II (SII; uneven skin surface over hypodermal masses resulting in irregular tissue texture) is manual drainage, compression stockings, an anti-inflammatory diet, and exercise. 3 Manual drains are usually poorly tolerated because the fatty tissue of patients with lipedema is painful. In addition, the variability of the procedure’s applied force, time, and intensity depends on the operator. Therefore, effectiveness varies and may be compromised. A device designed to stimulate the dermal functions and apply uniform drainage in terms of pressure and intensity would reduce intraprocedural variability and eliminate intertreatment variability. Advanced devices with these requirements can effectively treat edematous fibrosclerotic panniculopathy 14 and thus may offer a new conservative treatment option in managing patients with lipedema. TANIT platform combines the effects of a patented shape-in 3D technology based on low-level light therapy (LLLT) with infrared (IR) technology and damped bioactive current (DBC), together with a Slaag Motion (SM) for mechanical stimulation. TANIT reduces AT, favoring microcirculation and venous return. The decompression improves lymphatic vessels’ capacity, increasing the patient’s functional capacity and mobility.
The study’s main objective was to assess TANIT’s efficacy and safety, which combines DBC and mechanical stimulation on the same platform to reduce AT in patients with SI or SII lipedema. Secondary objectives were to analyze patient metabolic changes, 15 –17 pressure pain threshold (PPT), volume reduction of the lower limbs, and patient satisfaction.
Materials and Methods
Study design and participants
A single-center, before–after clinical trial without a control group was conducted at Doctor Randolfo Medicina y Cirugía Estética Medical Center (Barcelona, Spain) in patients clinically diagnosed with SI or SII lipedema to evaluate the efficacy and safety of the TANIT platform for their treatment. TANIT is a device classified as aesthetic equipment, not a medical device. It is not regulated by the Royal Decree 1090/2015 of December 4, which regulates clinical trials with medicines and medical devices, the Ethics Committees for Research with medicines, and the Spanish Registry of Clinical Studies (BOE-A-2015-14082).
The study adhered to the revised Declaration of Helsinki and Good Clinical Practice guidelines and followed all applicable laws and regulatory requirements concerning the use of devices in Spain; however, an IRB did not evaluate it. Data collection and management followed Spanish Organic Laws and European Parliament and Council regulations related to protecting individuals in the processing and free movement of personal data. All patients signed an informed consent before undergoing any study procedures.
Selection criteria
Inclusion criteria
Adult women aged 18–68 years old, diagnosed with SI or SII lipedema.
Bilateral leg swelling.
Negative Stemmer’s sign (inability to pinch the skin of the second toe in orthostatic position).
At least one secondary criterion (lower extremity pain, family history of lipedema, nonpitting lower extremity edema, or easy bruising or hypermobility).
Exclusion criteria
Patients with a history of decompressive surgery for lipedema.
Pathologies associated with lipedema.
Current skin infections or other signs of acute inflammation.
History of uncontrolled hypertension, diabetes, or arthritis.
Study visits, variables assessed, and treatment procedure
Before enrollment, a lymphedema specialist confirmed the lipedema diagnosis, including stage and type, to ensure that patients met eligibility criteria.
Study visits
The study included 12 visits: one baseline visit that included a blood sampling 24–72 h before the first treatment session, 10 treatment visits, and one final study visit the day after the last session with a blood sampling 24–72 h after the last treatment session. Before the first treatment session and after the initial blood sampling, a detoxification regimen was performed lasting up to 15 days, with the TANIT treatment starting on the 17th day. The treatment duration was 5 weeks, with two sessions per week. Figure 1 details the study flowchart and procedures. All patients were instructed to maintain healthy habits during the study with an equilibrated diet and moderate exercise.
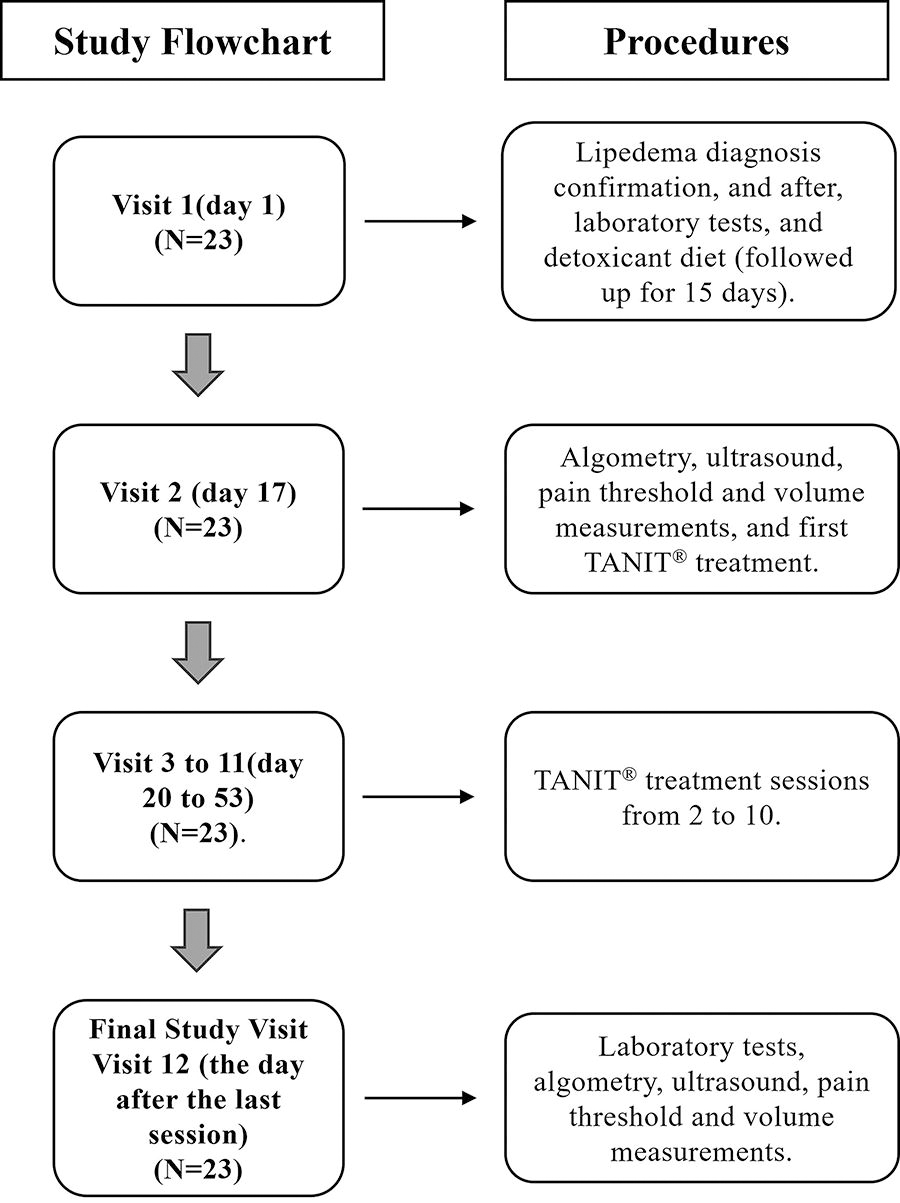
Study flowchart.
Variables assessed
A clinical evaluation was performed at baseline and the end of the study, including pain threshold, anthropometric and ultrasound measurements, and hematological and biochemical blood parameters. All laboratory tests were conducted 24 and 72 h before the first ultrasound examination, before starting the treatment, and between 24 and 72 h before the last ultrasound assessment at the end of the last treatment session. Efficacy measures were the increase in pain threshold, leg volume reduction, AT decrease in the legs at the end of the study, and the satisfaction survey results.
The pain threshold of both legs was measured in triplicate with the patient supine, using the Beslands SF-500 Digital Force Gauge algometer push-and-pull tester to determine the PPT expressed in kilograms. The PTT was measured at two locations: at the level of the inner side of the knee (3 cm distal to the inner side of the tibial head, above the fat fold) and at the ankle, at the distal third of the leg (4 cm proximal above the internal side of the tibial malleolus). The minimum value was 5 N/0.51 kg, the maximum value was 500 N/50 kg, and the precision was ±0.5%. Anthropometric measurements of the treated area of both legs were taken by the Bodytronic® Body Scanner (Bauerfeind®, Zeulenroda-Triebes, Germany), Model 600, expressed in volume (mL) with the patient in a standing position. The exact points for each anatomical measurement were automatically determined by the Bodytronic® Body Scanner for each patient and were kept the same for all visits. Ultrasound measurements for the areolar, lamellar, total, and deep surface of subcutaneous AT were conducted using the Series 7410 Model MyLabSigma with the linear probe L4-15 MHz (Esaote S.p.A., Genoa, Italy). The patient was positioned supine with the muscles relaxed. The probe was directed longitudinally and transversally, with measurements taken at the following locations: the external side of the ankle (on the external malleolus), the internal side of the knees, and the trochanteric area. The results were expressed in millimeters (mm), and the decrease was expressed in percentages (%). The points of maximum projection of AT (internal side of knees and trochanters) and the ankle were analyzed to assess morphological changes in the bracelet sign because, in these locations, the greatest volume of AT is found, resulting in the largest diameter at the level of the lower limbs. The measurements were taken at the outset of the first session and after the final session. At the final study visit, patients completed a satisfaction survey with 12 questions about treatment outcomes, safety, number of sessions required before seeing initial results, overall satisfaction, and compliance with study recommendations.
Treatment procedures
Once baseline assessments were completed, the first session with the TANIT platform (
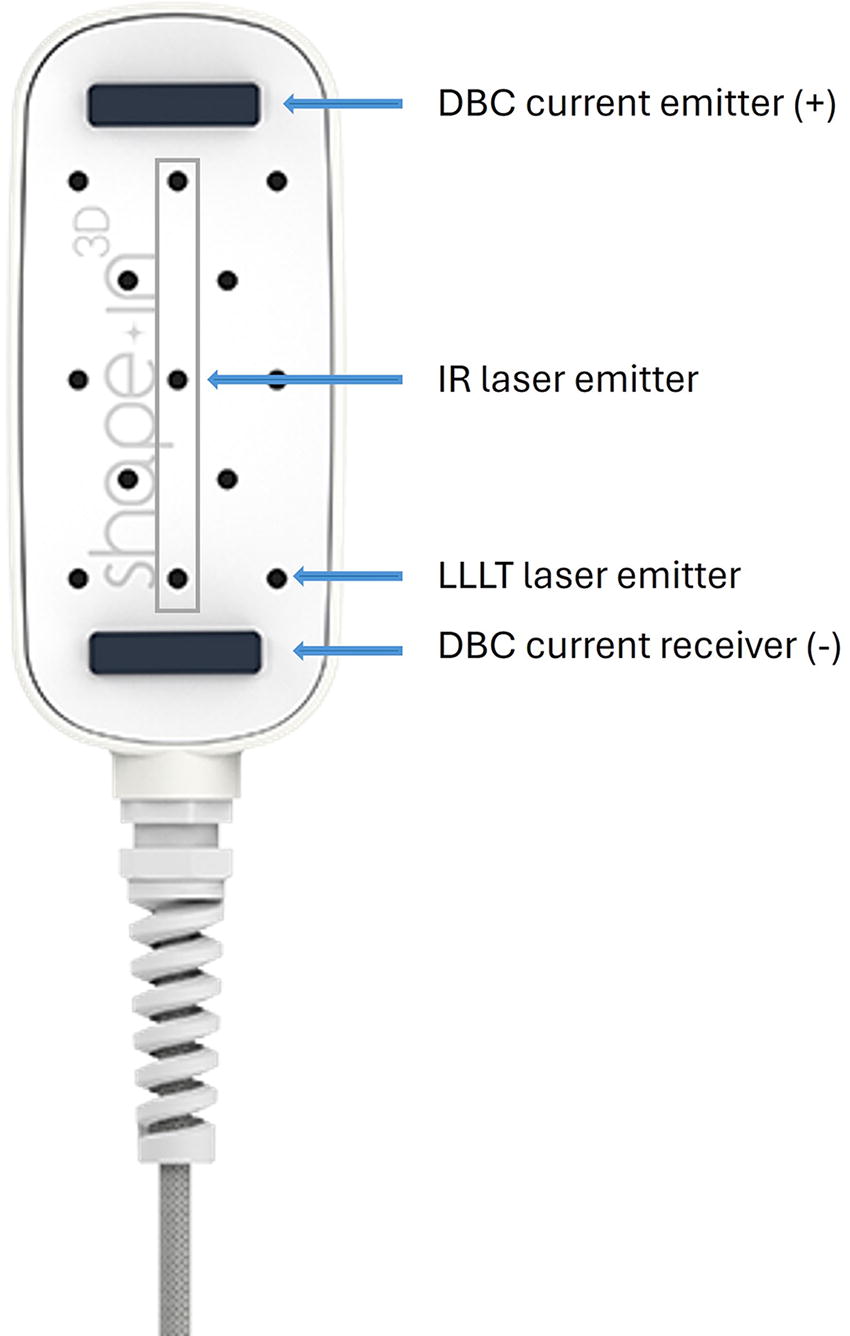
The shape-in 3D pad. DBC, damped bioactive current; IR, infrared; LLLT, low-level light therapy.
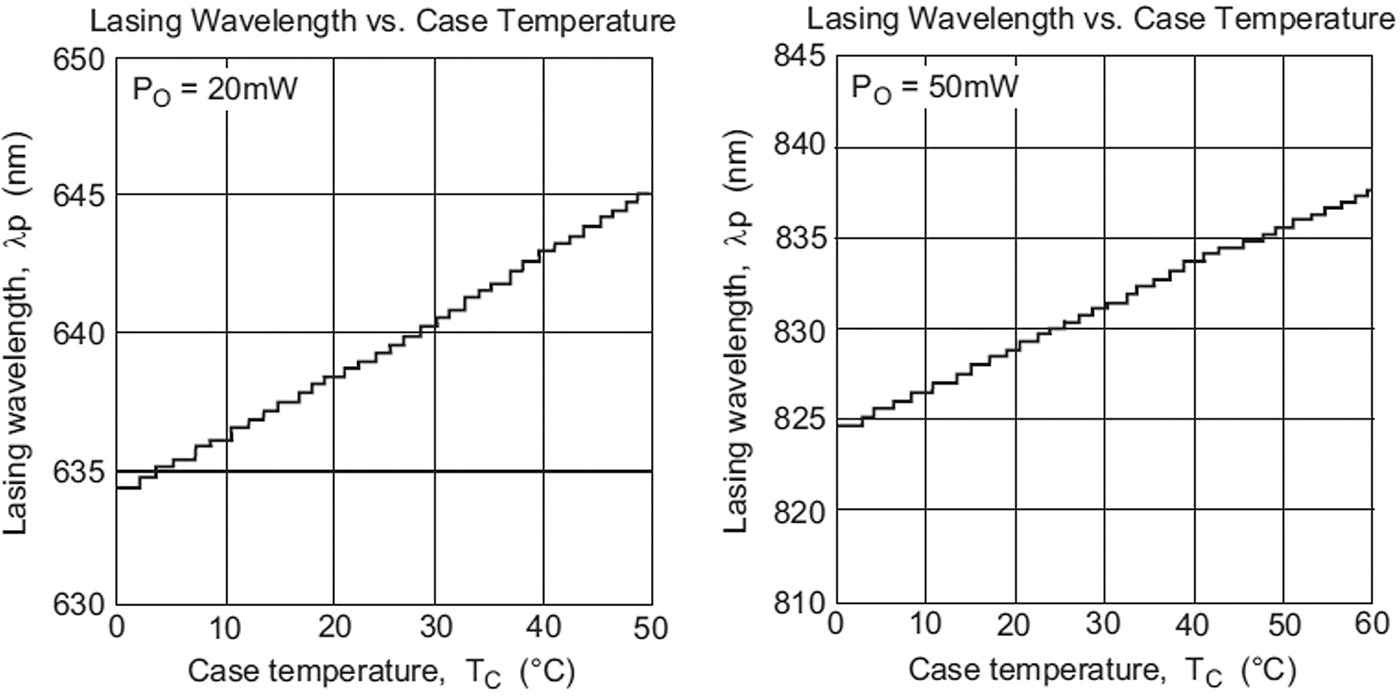
Wavelengths deformation in response to changes in the temperature of the encapsulated.
SM was applied for 20 min per leg, 10 min on the anterior side and 10 min on the posterior side. Slaag Wave/Slaag Up maneuvers were performed at a speed of 200 rpm, with superficial pressure in the area to be treated. After treatment with SM, the pads were placed on the treated area. Each laser treatment was performed for 10 min with 100% LLLT and DBC intensity on the front and back of each leg.
The three energies applied (LLLT, DBC, and SM), due to their individual properties, produce a quadruple action that can be translated into (1) stimulation of blood microcirculation 18 ; (2) reduction of inflammation 19 ; (3) activation of the cellular metabolism of adipocytes, causing a lipolytic effect that releases fat 20 –22 ; and (4) tissue regeneration, 19 increasing the production of collagen, 23 elastin, and hyaluronic acid. Also, with the rotation movement, the SM helps activate natural physiological processes from the skin to the muscles with a firming, draining, and remodeling effect.
Safety assessments
All complications and side effects during the study were collected and all methodological and procedural complications during the treatments were analyzed.
Statistical analysis
Quantitative variables for each leg were described as mean and standard deviation (SD), median, and quartiles 25 and 75 (Q25, Q75). Categorical variables were expressed as percentages. Efficacy outcomes were assessed as the change in percentage of the corresponding variable from baseline to the last treatment session.
Before and after treatment, pain threshold, lower extremity volume, and AT thickness measurements of both legs were compared using the Wilcoxon signed-rank test to assess the significance of differences. For all hypothesis tests, statistical significance was defined as p ≤ 0.05.
Results
Patient characteristics
Twenty-three women were enrolled, ranging in age from 23 to 67 years, with a mean age of 44.91 (SD 11.58) and a median of 46.00 (Q25 = 36.50, Q75 = 51.50). Seven (30.4%) patients had SI lipedema, and 16 (69.6%) had SII. All patients completed the study. The blood tests at the beginning and end of the study showed that most patients had metabolic parameters within normal limits during the evaluation. After the intervention, patients who initially exhibited high cholesterol, triglycerides, and/or fibrinogen levels experienced notable improvements without statistically significant differences. However, the group was small and no changes were observed in the evaluated parameters (Supplementary Table S1).
Pain threshold
The average pain threshold measured before and after treatment showed an increase in 18 (78.3%) patients at the knee level (p = 0.19706) and in 20 (80%) at the ankle level (p = 0.00386). The statistical results of pain threshold by stage of lipedema are detailed in Table 1.
The Percentage of Increase in Pain Threshold at the Inner Side of the Ankle and Knee Levels After the Treatment
Patients with at least one leg with pain threshold increase.
N, number of patients; % percentage; SI, stage I; SII, stage II.
Anthropometric measurements
The legs volume in milliliters was analyzed before and after treatment. After treatment, the differences in both legs were statistically significant (p = 0.0035). The results are detailed in Table 2, which includes the volume measurements per leg before and after treatment in patients with SI and SII lipedema. Post-treatment, 18 (78.3%) patients had a volumetric leg decrease, 6 (85.7%) patients with SI lipedema with a mean volumetric decrease of 3.8% (range 0.9–6.5%), and 12 (75.0%) patients with SII with a mean decrease of 3.7% (range, 0.2–9.6%). After treatment, averaged differences of both legs in area A (thigh) were statistically significant (p = 0.00116) and not in the averaged area B (lower leg) (p = 0.12852). Six (85.7%) patients with SI lipedema had a mean volumetric decrease of 4.3% in the thigh area (range, 1.4–7.5%) and 2.9% in the lower leg area (range, 0.6–5.7%). Patients with SII had a mean decrease of 4.2% in the thigh area (range, 1.2–11.3%) and 3.1% in the lower leg area (range, 0.6–9.0%). As examples of the external changes, Figure 4 shows the pre- and post-treatment results of three patients with SI lipedema and three with SII lipedema.
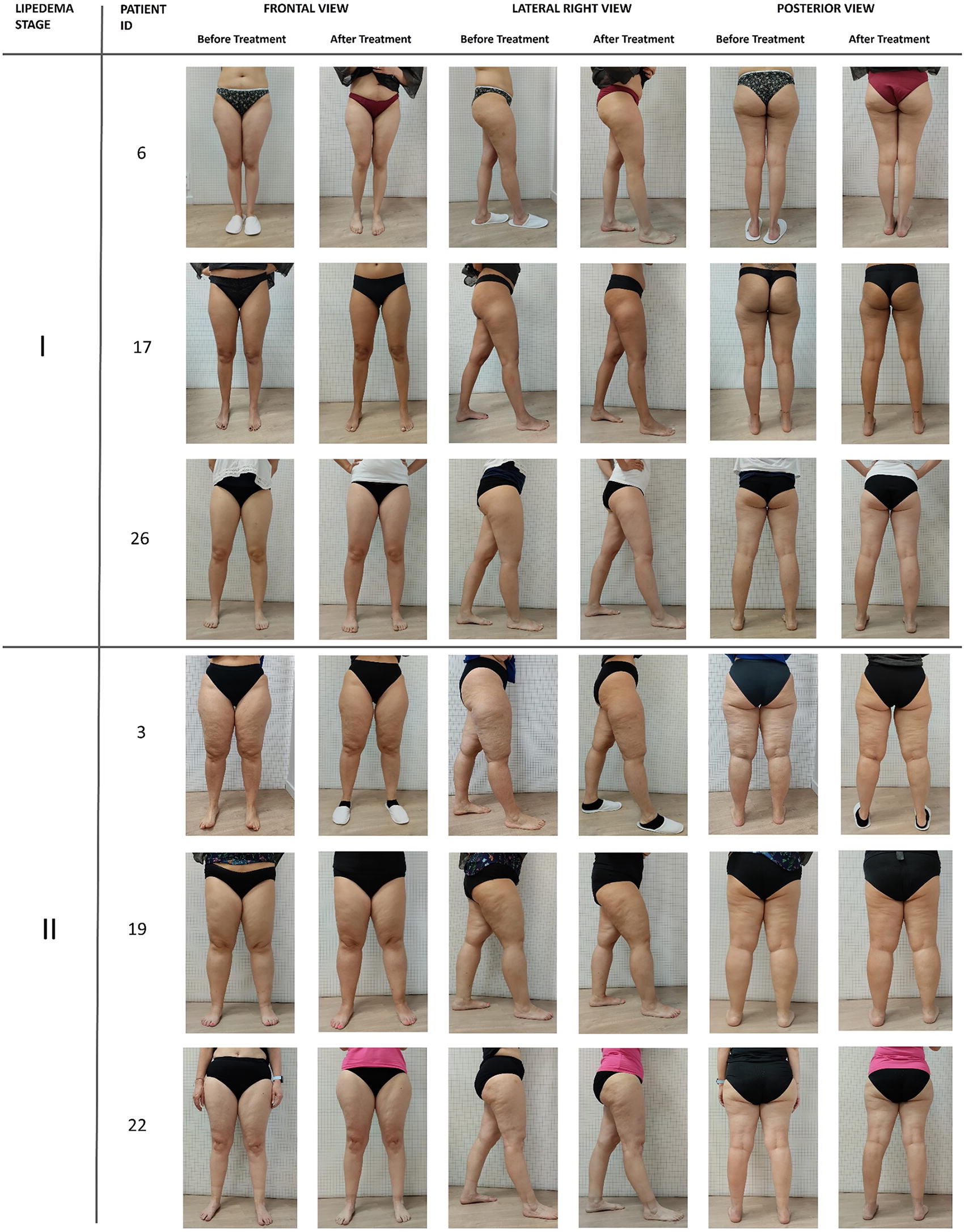
Pre- and post-treatment images of three patients with SI lipedema and three with SII lipedema. SI, stage I; SII, stage II.
Leg Volume by Area A (Thigh) and B (Lower Leg), in Milliliters, Measured at Baseline and After Treatment
RLPre, right leg pre-treatment; RLPost, right leg post-treatment; LLPre, left leg pre-treatment; LLPost, left leg post-treatment; Diff, difference; A, thigh; B, lower leg; SD, standard deviation; WS-R, Wilcoxon signed-rank test.
Ultrasound measurements
After treatment, a decrease in AT thickness was detected in all treated areas, with a mean decrease of 26.1% (range of 1.1–69.0%) at both ankles, 14.5% (range, 1.3–48.2%) at both knees, and 17.4% (range, 0.6–68.4%) at both trochanter levels. Ankle ultrasound measurements: After the treatment, differences after treatment were statistically significant at the areolar surface (p = 0.0008), at the lamellar surface (p = 0.00278), and at the total surface (p < 0.00001). Knee ultrasound measurements: After treatment, we found statistically significant differences at the areolar surface (p = 0.00048), the lamellar surface (p = 0.0009), the total surface (p < 0.00001), the deep layer (p < 0.00001), and the total (p < 0.00001). Trochanter ultrasound measurements: After treatment, differences were statistically significant at the areolar surface (p = 0.0251), the total surface (p = 0.00096), and the total (p = 0.00012), and were not significant at the lamellar surface (p = 0.15272) and the deep layer (p = 0.06876). Figure 5 shows patients’ 17 and 23 ultrasound images of the areas treated with the highest reduction. Other statistical results of ankle, knee, and trochanter ultrasound measurements are detailed in Table 3.
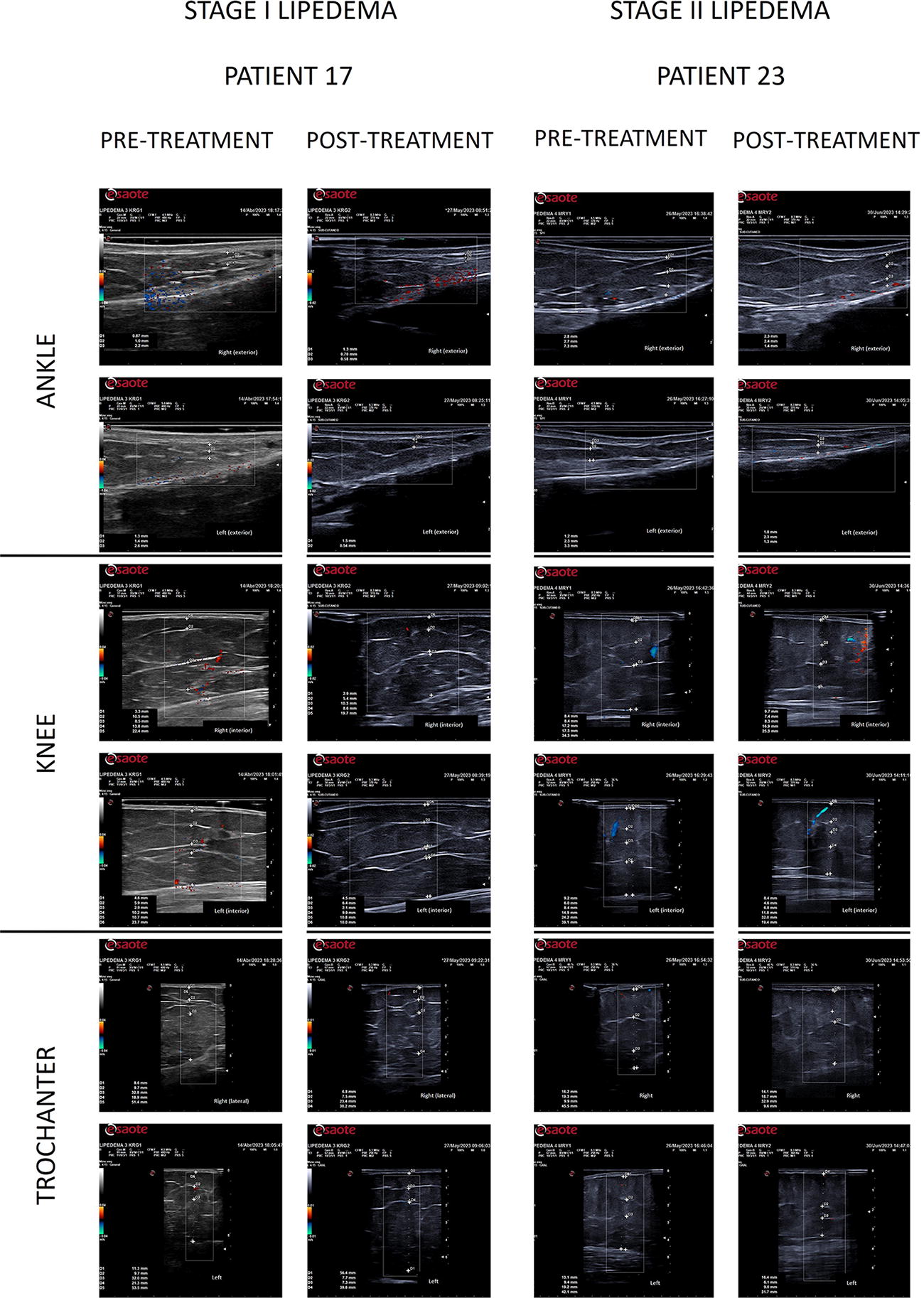
Ankles, knees, and trochanters ultrasound images of patients 17 and 23 before and after treatment.
Adipose Tissue Decreases After Treatment at the Ankle, Knee, and Trochanter Levels Measured by Ultrasound of Patients with Lipidemia Stages I and II
Patients with at least one leg with decrease.
Satisfaction survey
Patient responses regarding the decrease in edema, changes in skin texture, skin firmness, and decrease in volume (Fig. 6). The greatest changes are evident from the fifth session, consistent with the survey response, where the percentages show the changes from session 5, with the maximum being in the last session. Further, the satisfaction percentage was high. Eighteen (78.3%) patients followed the diet and 16 (69.6%) exercised. All patients would recommend the treatment.
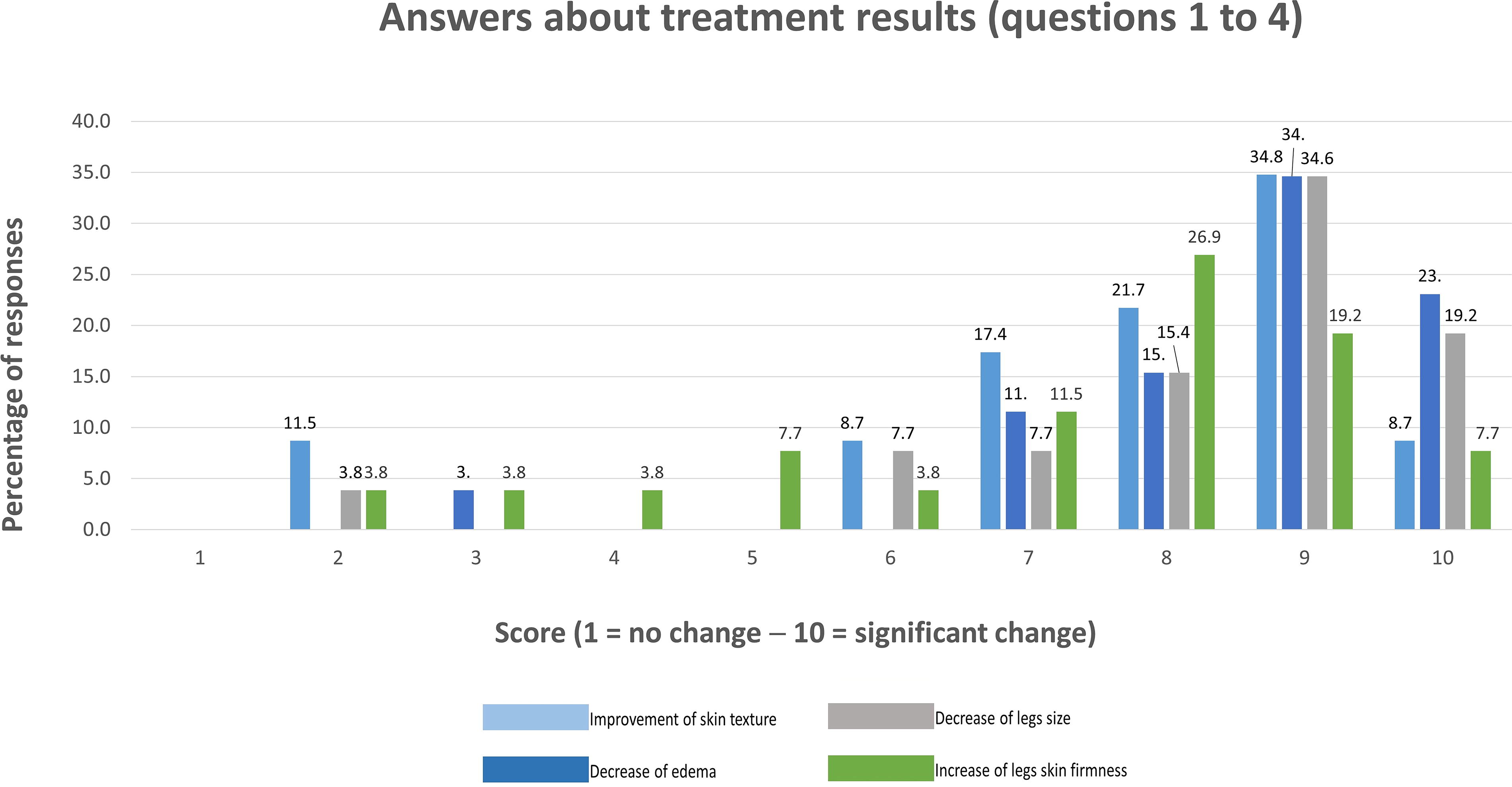
Answers to survey questions 1–4 about treatment results.
Safety findings
No patients required analgesia/anesthesia before or after treatment. Twelve (52.2%) patients had no annoying or limiting bruises after the first and second sessions. One (3.4%) patient presented post-treatment hematomas that decreased in number and size. Nineteen (82.6%) patients had post-treatment pain after the first session. Eleven (47.8%) patients had pain during the first and second sessions and no pain in the successive sessions. One (4.3%) patient reported pain during the first five sessions, disappearing in subsequent sessions. No other treatment complications or adverse effects were associated with TANIT treatment (Fig. 7).
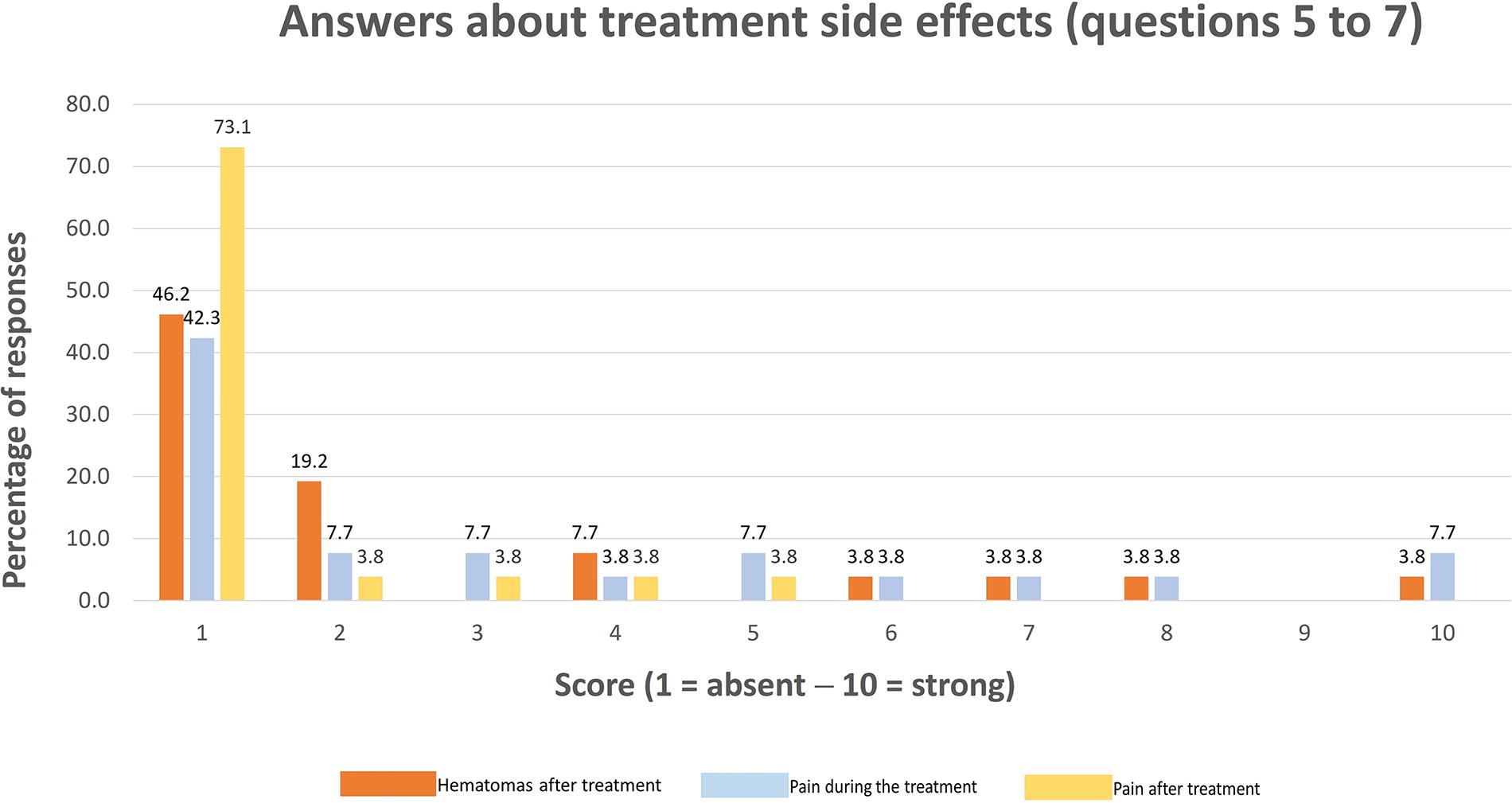
Answers to survey questions 5–7 about treatment side effects.
Discussion
The reduction of AT decreases the compression of lymphatic vessels and the associated inflammatory response in the affected area. These changes aim to improve blood flow, alleviate lipedema symptoms, and enhance skin appearance. The combined properties of the three energies comprised in the device, LLLT (light), DBC (electrical energy), and SM (mechanical), have demonstrated efficacy in reducing AT and pain. The proposed potential mechanisms for the obtained results were microcirculation activation, 18 inflammation reduction, 19 fat tissue reduction, 20 –22 and tissue regeneration, 19,23 with a remodeling effect. The treatment protocol in this before–after clinical trial, without a control group, was developed as a conservative alternative for lipedema patients. The study results showed that TANIT treatment improved the pain threshold, especially at the knee and ankle level, and reduced the volume and AT of the lower limbs with statistically significant changes in the thigh area. Further, treatment was safe and well tolerated by patients, who were satisfied with the results, an advantage over other currently proposed treatments for lipedema, which often encounter low tolerance among patients.
Some studies have also assessed new strategies to increase the efficacy of standard care with a superiority of effectiveness for combined treatments. 24,25 A nonrandomized clinical trial found a statistically significant reduction in the volume of both limbs with CDT. 26 A study found that the ketogenic diet could be a handy tool to consider in the management of lipedema. 27 Few studies had used ultrasound to measure AT thickness and evaluate the effectiveness of specific treatments. However, ultrasonography could be valuable for evaluating treatment outcomes. 28 Only one relevant study was identified in this context with a nonstatistically significant decrease in the thickness of fatty tissue. 29 The limited number of clinical trials that address conservative lipedema treatments and the scarcity of studies using ultrasound to quantify AT thickness made it difficult to compare our results with the existing literature. 28 Our patients, with biochemical parameters within normal values, remained normal during treatment regardless of the degree of lipedema. In those patients with high cholesterol levels, complement and fibrinogen improved, maybe due to the detoxification diet, without significant differences. In some patients, no appreciable improvement was observed, possibly linked to a lack of diet and physical activity adherence. These findings highlight the importance of considering and promoting adherence to nutritional guidelines and physical activity in the management and comprehensive treatment of patients with lipedema.
Among study limitations are the low number of patients with SI lipedema, which decreased the sturdiness of some of the formulas used, the noninclusion of a control group, randomization, or a long-term follow-up. Additionally, AT reduction by diet and exercise could have slightly modified our results. Although lipedema does not improve with diet and exercise alone, it is important to include a common diet and exercise guidelines for all patients in future studies to avoid possible bias. Another limitation is the need for a standardized questionnaire to assess the patient’s quality of life, and for future studies, genetic, hormonal, and inflammatory parameters would be relevant to include.
Conclusions
TANIT platform offers promising advances in conservative treatment for patients with SI and SII lipedema. It addresses the reduction of leg volume and AT thickness, pain relief, and improved quality of life. However, additional controlled randomized clinical trials and standardized assessment tools would be necessary.
Footnotes
Acknowledgments
The authors thank Ortopedia Grausoler S. A. for measuring with Bodytronic® the patients’ lower limbs, Teletest for carrying out the laboratory analyses, Linfacal and Adalipe for their valuable contribution in disseminating the study, thus facilitating the identification and participation of patients, Novasonix Technology for providing the equipment and training the technical staff for this study, and Martha Hernández Gonzalez for her valuable collaboration along the study. Additionally, the authors thank the i2e3 Procomms team for providing medical writing support during the article preparation phase.
Authors’ Contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published. Conceptualization, methodology, data acquisition, and analysis: Y.C.C.Q., J.d.D.P.B., R.J.F.P., and A.S.H. Writing—original draft preparation and writing—review and editing: Y.C.C.Q. and J.d.D.P.B.
Author Disclosure Statement
Y.C.C.Q. and R.J.F.P. have no conflict of interest or financial ties to disclose. J.d.D.P.B. and A.S.H. are external collaborators of
Funding Information
This study was funded by Novasonix.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.