
Abstract
Background:
Rhinophyma, an advanced form of rosacea, primarily affects older men and is characterized by nasal hypertrophy and irregular surface texture. Traditional treatments include pharmacologic interventions and various surgical techniques.
Objective:
To present the clinical outcome of a novel combined treatment using fractional carbon dioxide laser (FCL) and fractional microneedle radiofrequency (FmRF) in a patient with rhinophyma.
Methods:
A 62-year-old male with prominent nasal seborrhea, hypertrophy, and surface irregularities underwent combined treatment with FCL and FmRF. The treatment sessions were performed under topical anesthesia with post-procedure care including emollients and sun protection.
Results:
The patient experienced marked cosmetic improvement, including reduced nasal bulk and smoother surface texture, without adverse events such as scarring or pigmentary alteration. The recovery period was short, and patient satisfaction was high.
Conclusions:
This case represents the first report of combining FCL and FmRF for the treatment of rhinophyma. The favorable clinical and cosmetic outcome suggests this method may be a promising alternative to conventional surgical approaches. Further studies are needed to validate its efficacy and safety in broader populations.
Introduction
Rhinophyma is a benign yet cosmetically disfiguring condition and is recognized as the most frequent manifestation of phymatous rosacea. 1 It typically arises in conjunction with erythematotelangiectatic or papulopustular subtypes of rosacea and is disproportionately observed in middle-aged and older male patients. 1–2 The exact pathogenesis remains unclear; however, it is frequently linked to longstanding rosacea. 2 Clinically, rhinophyma is characterized by progressive sebaceous gland hyperplasia, connective tissue proliferation, and dilation of cutaneous vasculature, primarily affecting the lower two-thirds of the nose. 2 Although histopathological assessment is not routinely performed, rapidly enlarging or ulcerative lesions should prompt consideration of malignant entities, including squamous cell carcinoma and basal cell carcinoma. 1,2 Pharmacologic interventions, such as low-dose isotretinoin, may reduce glandular hypertrophy but do not restore normal skin contours. 1 –3 Surgical modalities remain the primary treatment, aiming to excise excess sebaceous tissue and restore nasal contour. 1 Techniques include electrocautery, radiofrequency surgery, dermaplaning, dermabrasion, cryosurgery, carbon dioxide (CO2) laser surgery, and erbium: yttrium aluminum garnet laser therapy, among others. 1 –4 This report presents a case of mild rhinophyma successfully treated with a combination of FCL and FmRF, offering a promising alternative to conventional interventions.
Although FCL and FmRF both aim to remodel dermal tissue, their mechanisms are distinct and complementary. FCL creates controlled epidermal and superficial dermal ablation, improving surface irregularities and promoting collagen synthesis. In contrast, FmRF delivers focused thermal energy into deeper dermal layers via insulated microneedles, modulating sebaceous gland activity and enhancing dermal tightening. This dual approach targets different pathological components of rhinophyma, offering synergistic benefits in texture refinement, glandular remodeling, and overall contour correction.
Case Report
A 62-year-old male attended our dermatology clinic with complaints of excessive sebum production, nasal thickening, and surface irregularities. The patient had previously undergone topical and systemic therapies, including metronidazole and low-dose isotretinoin, with minimal improvement. Clinical examination revealed sebaceous gland hypertrophy, prominent seborrhea, dilated pores, and pronounced textural abnormalities (Fig. 1a). After a thorough discussion regarding therapeutic options, anticipated outcomes, potential risks, and alternative strategies, the patient consented to combination therapy with FCL and FmRF.
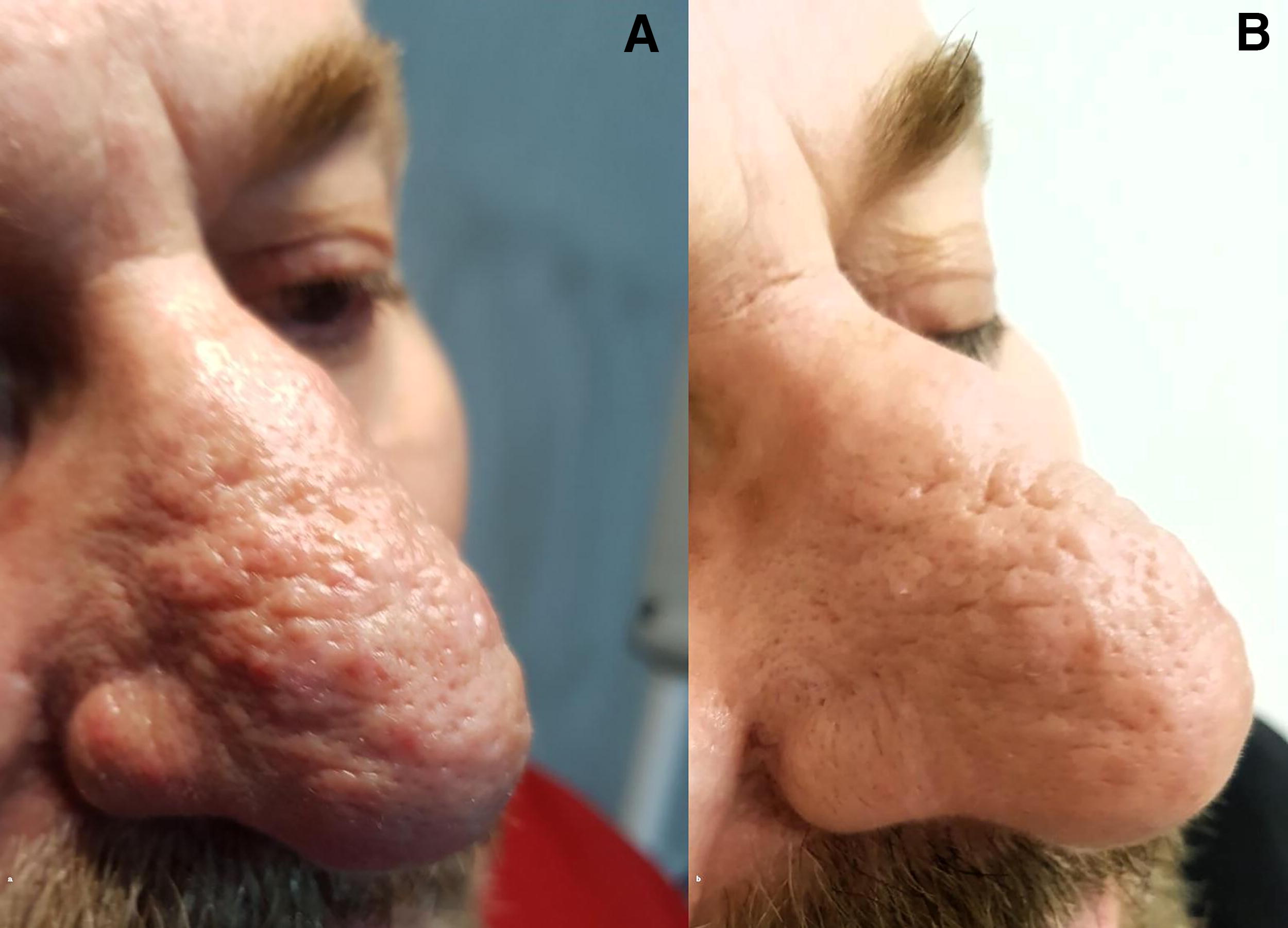
Topical lidocaine/prilocaine cream was applied under occlusion before the procedure. Both treatments were well tolerated, and the patient did not report significant pain or require systemic analgesia. Treatment was administered using the Fraxis Duo® system (Creative Ilooda, Korea). The Fraxis Duo® device includes both FCL and FmRF modalities on a single platform; therefore, both treatments were delivered using the same equipment. FCL was delivered via a 20 × 20-mm handpiece at a 30 mJ energy setting with a 0.2-ms pulse duration, employing two passes with 10%−20% overlap (2). Subsequently, FmRF was applied with a handpiece containing 25 microneedles, set at 100% RF energy intensity for 90 ms with a 150-ms delay, achieving a penetration depth of 2.2 mm in 0.2-sec mode (5). In our case, both procedures were deliberately performed in the same session to maximize treatment efficiency and achieve optimal clinical outcomes. Posttreatment erythema was mitigated with cold compresses, and a centella asiatica-containing ointment, recognized for its epithelializing, wound-healing, and antimicrobial properties, was prescribed. A broad-spectrum SPF 50 sunscreen was applied, with instructions for continued use alongside the ointment twice daily for 10 days. The patient was clinically assessed on the 1st and 4th weeks post-procedure to monitor for adverse effects and evaluate treatment efficacy. Follow-up photography (Fig. 1b) was obtained at the 4-week visit to document clinical response. The patient achieved remarkable aesthetic improvement without postoperative complications, such as scarring, hypopigmentation, or hyperpigmentation.
This case report did not require approval from the institutional review board in accordance with local regulations for single-patient case reports. However, written informed consent for publication of clinical details and images was obtained from the patient.
Discussion
Rhinophyma treatment strategies range from complete excision of affected tissue to partial excision facilitating epithelial regeneration from residual glandular structures. 1 Partial excision techniques encompass cryosurgery, electrosurgery, dermabrasion, and laser ablation. 1 –3 While cryotherapy is an accessible and cost-efficient option, it is associated with suboptimal hemostasis and scarring. 1 Electrosurgical techniques, though effective, generate substantial thermal damage, risking cartilage necrosis, extended healing durations, and atrophic scarring. 1,2 FCL has demonstrated advantages over traditional modalities, offering superior cosmetic outcomes, precise tissue ablation, and reduced complication rates, making it suitable for outpatient settings under local anesthesia. 2 The 10,600 nm wavelength of FCL targets water as the principal chromophore, facilitating controlled tissue vaporization. 2 This mechanism produces microthermal treatment zones that promote collagen synthesis, dermal remodeling, and wound healing, extending from the epidermis into the reticular dermis. 3,4 Compared to conventional CO2 lasers, this controlled vaporization minimizes post-inflammatory pigmentary alterations and scarring. 2 –4
FmRF complements FCL by generating controlled thermal energy that stimulates fibroblast activity, enhances collagen production, and facilitates dermal restructuring. 5 The therapeutic mechanism of FmRF is thought to involve sebaceous gland modulation and anti-inflammatory effects, potentially reducing angiogenesis in rosacea. 6 The observed full reepithelialization within 2 weeks aligns with previously reported recovery timelines, reinforcing the efficacy of this approach. In our case, both procedures were intentionally performed during the same session to enhance treatment efficiency and optimize clinical outcomes. Performing FCL first enables precise superficial debulking, while immediate FmRF application targets the deeper dermis during the same inflammatory cascade. This sequence may potentiate collagen remodeling and tissue regeneration, reduce the number of visits, and shorten the total recovery period. Our findings suggest that the combination of FCL and FmRF represents a compelling alternative to conventional rhinophyma treatments, providing improved cosmetic outcomes, reduced recovery time, and high patient satisfaction with a favorable safety profile. To date, this is the first reported case of rhinophyma managed with this dual-modality treatment. Further prospective studies are necessary to substantiate these findings and establish standardized treatment protocols.
Footnotes
Authors’ Contributions
G.I.K.: Conceptualization, investigation, methodology, writing—original draft, visualization. E.K.: Supervision, review, and editing—original draft. All authors have read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.