
Abstract
Patients who newly start prescription medications for chronic conditions are often in need of additional support related to both their condition and treatment. When patients initially fill their prescriptions, the offer of pharmacist counseling is considered standard practice from a professional and regulatory standpoint, but little is known about how well this offer actually satisfies patient needs. This was the focus of our study: Within a few weeks of newly starting medications, 100 patients were contacted telephonically by a nurse to engage them in a support program for their conditions. During those calls, the nurse used a brief questionnaire to determine each patient's recollection of the offer of local community pharmacist counseling at the time that they filled their prescription, and their current receptivity to immediate telephonic pharmacist support. Fifty-eight percent of patients did not recall being offered counseling at their local community pharmacy, and 11% declined the offer at that time, yielding 69% of patients who did not receive local pharmacist counseling when filling their initial prescription. An additional 12% (39% of patients counseled) were not satisfied with the information received. Among the 81% of surveyed patients who did not receive counseling or were dissatisfied with the counseling they did receive, 75% accepted the offer of telephonic support by a specialist pharmacist. Our findings suggest that many patients with chronic conditions have a need and a desire for pharmacist counseling about new medications that is unmet in the local community pharmacy setting. Telephonic pharmacist support can help address this need if offered within weeks of the new prescription. (Population Health Management 2010;13:189–193)
Introduction
The period after a new diagnosis or after starting a new long-term medication also represents an important “teachable moment,” when the patient may actually be most in need of counseling and support. 2 This is a time when patients are highly focused on their own health and therapy. Successful outreach in this critical time window has the potential to positively impact long-term patient care. 3,4
State pharmacy regulations, as well as professional practice obligations, often require that the pharmacist offer to provide clinical support at the time of dispensing. However, verbal counseling by the pharmacist appears to occur infrequently and with considerable variability. A 1995 study exploring pharmacist–patient communication found that the frequency of direct interaction varied from 30% to 100% of all dispensing events, and included clinical as well as administrative topics. 5 In a recent study that utilized “trained shoppers” for data collection, patients were proactively offered verbal counseling by their pharmacist during 27% of dispensing interactions; an additional 16% received verbal counseling after prompting it themselves. 6 A similar earlier study that evaluated counseling practices in 306 community pharmacies in 8 states found that 63% of the trained shoppers were provided verbal drug information, with considerable pharmacy-to-pharmacy variation. 7
Given the importance of providing clinical support to patients around the time they begin new therapies for chronic conditions, the current study was undertaken to explore the opportunity further, including whether patients would be receptive to immediate offers for telephonic support from a pharmacist who specializes in their condition, soon after they received their prescription from their local pharmacy.
Methods
Patients were identified for this survey study through their eligibility for a program offered by their employer or health plan to support and optimize self-care for their chronic conditions. Such patients were identified for an “early engagement” form of outreach in June 2009, through daily monitoring of pharmacy claims that represented new prescriptions filled. When patients newly filled a medication in a drug class suggestive of a chronic condition addressed by the program (Table 1), telephonic outreach by a nurse was initiated as an introduction.
The survey itself, shown in Table 2, was offered consecutively to all patients who were successfully contacted for the “early engagement” outreach, and who had recently filled their new prescriptions in a local community pharmacy setting. The survey questions were asked by a nurse at the conclusion of the program's call. The study design required consecutive patients to be surveyed, generating complete and usable data for 100 respondents. (Responses were deemed unusable if they were incomplete or followed a logically impossible flow, such as proceeding from Question 1 with a “no” response to Question 2, instead of Question 5.) Any unusable survey attempts were discarded, and additional patients were consecutively surveyed until the prespecified goal of 100 was met.
Results
In order to achieve the planned objective of 100 consecutive unique patients with complete and usable data, the survey was attempted during calls to 123 patients, because 23 were excluded as described in the Methods section.
Demographic and medication-related characteristics of the surveyed patients are presented in Table 3. Of particular note is the magnitude of medication usage for these patients in the prior year, suggesting considerable chronic condition complexity.
Patient responses to the survey questions are displayed in Figures 1 and 2. A key finding is that 69% of patients did not receive in-person counseling from their local pharmacist. This group was comprised of 58% who did not recall being offered an opportunity to speak with the pharmacist about their new medication, and 11% who recalled the offer but did not accept it. In addition, 12% of the population surveyed and 39% of the patients who were counseled were not satisfied with the information they did receive. Among the 81% who either were not counseled or were not satisfied with the information, 75% were receptive to an immediate offer of telephonic counseling from a specialist pharmacist. Of the patients who accepted telephonic support, 84% received it immediately as part of the same call and 16% requested a callback from the pharmacist.
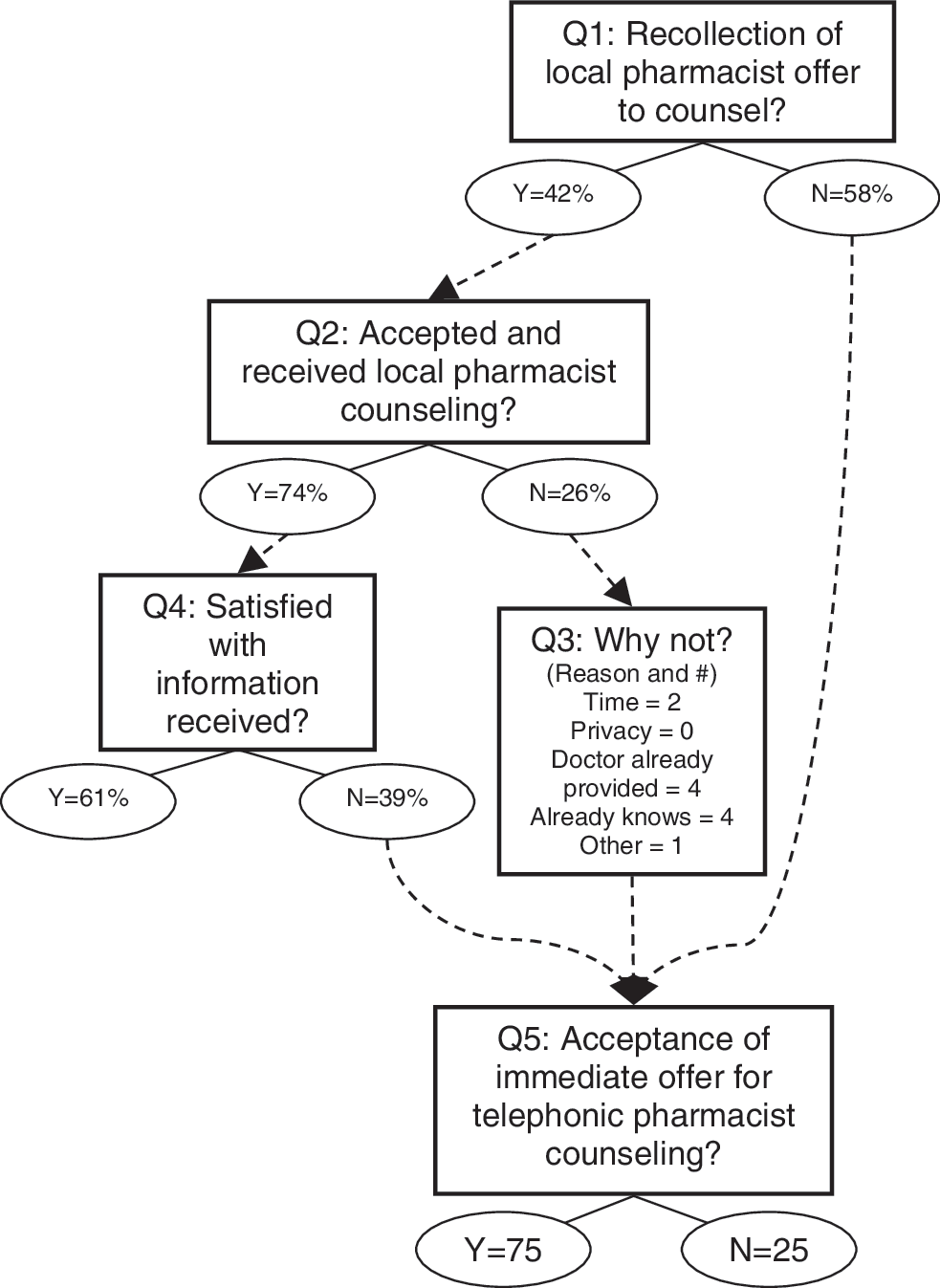
Survey flow and responses to each question.
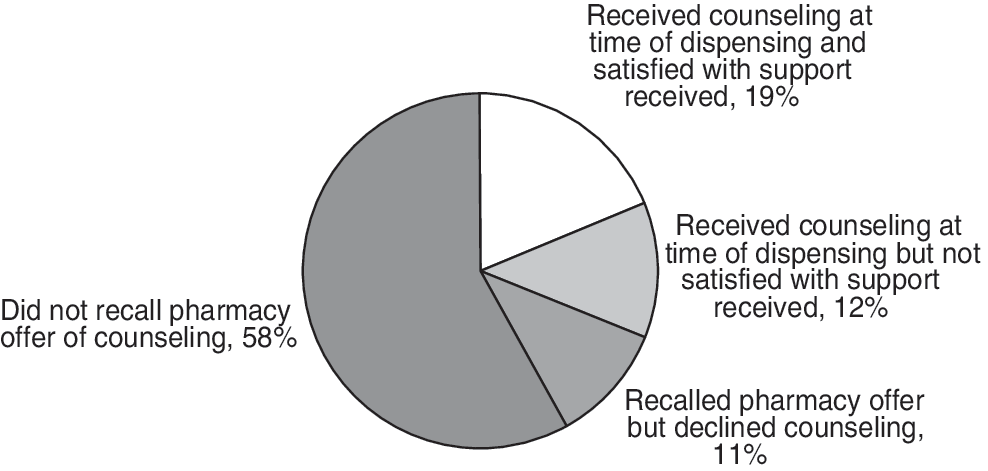
Summary of survey responses.
The survey nurses also asked patients about their reasons for not accepting the initial offer of counseling from their local pharmacist. The distribution of responses is shown in Table 4.
Discussion
Pharmacist counseling at the time a new medication is started represents a crucial opportunity to help patients be more successful with their therapy. The period after a new drug is started is a time when many patients become nonadherent. In a large managed care population, it was found that 16%–22% of patients who were prescribed medications essential to treat various chronic conditions never refilled these medications after the initial dispensing event, despite pharmacy access and plan coverage. 8
Improving medication adherence through pharmacist counseling at the start of therapy can positively impact subsequent health care utilization and cost. Various estimates suggest that 33%–69% of medication-related hospital admissions are caused by nonadherence, resulting in approximately $100 billion in health care costs per year. 9 The authors of a study that examined the impact of medication adherence on hospitalization risk and health care costs found that higher adherence was associated with significantly lower disease-related medical costs for diabetes, hypercholesterolemia, and hypertension. 10
Pharmacist counseling may also help prevent adverse drug events (ADEs) among new prescription users. A study that evaluated ADEs in the outpatient setting found that 25% of patients experienced ADEs, 28% of which were ameliorable. Of these ameliorable ADEs, 37% involved the patient's failure to inform their physician. 11 By having a pharmacist review potential side effects as a component of new prescription counseling, patients may be more attuned to such symptoms and more inclined to report them to the physician at an earlier time.
In addition, pharmacists are well positioned to address cost barriers to adherence that patients may not have discussed with their physicians. In a large survey study, 17% of older adults with chronic illness reported cost-related medication underuse in the prior year. Of these, 67% never told their prescriber that they planned to underuse medication because of cost, and 35% never discussed cost at all. Common reasons cited for not discussing the issue were not being proactively asked by their prescribers, and not thinking their prescribers could help. Yet when prescribers did discuss cost with patients, 72% found the conversations helpful. 12 Pharmacists can help address this important unmet patient need by proactively asking patients about financial barriers to adherence, and by working with patients and their physicians to address these barriers.
These issues are particularly pronounced and important in the period immediately following hospital discharge, when patients often transition to new medication regimens. 13 Project RED (Re-Engineered Discharge) has actively studied the issue and found that, when patients were contacted telephonically by a pharmacist in the days after hospital discharge, 52% of them had medication problems that required active intervention. 14
Despite the importance of providing robust support when new medications are started, and despite offers by community pharmacists to provide clinical counseling, 69% of patients in the current study did not receive such care. Although some reports suggest that community pharmacists are now providing more counseling about medications than they did in past decades, significant opportunity remains unaddressed. 15,16
An important contributor to this problem is the significant time pressure experienced by local pharmacists who are required to fit patient counseling into a busy environment that already requires fast, high-volume prescription fulfillment and medication dispensation. 7 When surveyed, 59% of pharmacists reported that they did not have enough time to provide important adherence counseling. 17
Furthermore, even when local pharmacists are able to find the time to counsel, their patients often do not accept that offer at the time of dispensing. In fact, the assessment of patient motivation is reported by pharmacists to be one of the greatest determinants of the amount and type of counseling offered. 18
Patient responses to the question of why they declined local counseling suggest that they may not perceive the need for support at the time they pick up their new prescriptions. Yet many of these same patients are highly receptive (75%) to subsequent offers of telephonic pharmacist counseling. A possible explanation is that patients sometimes require more time to process the implications of being prescribed a chronic medication and formulate their questions. Another possible contributor is that patients may be uncomfortable discussing certain issues face-to-face in a pharmacy environment, compared with telephonically. Further research is necessary to understand the best methods, venues, and timing of patient support. This study suggests that telephonic pharmacist outreach soon after a new prescription is filled may be an excellent solution.
Limitations
The primary limitation of this study is that it involved only patients who were successfully engaged in a telephone call by a nurse who invited them to participate in a care support program, because the survey was added to these calls. These patients may be intrinsically more receptive to counseling offers such as the opportunity to receive immediate telephonic pharmacist support. However, one would anticipate such patients to be receptive also to local pharmacist counseling offers at the time of dispensing, which the data do not demonstrate, thereby mitigating the impact of this limitation.
Other limitations involve recollection bias and respondent bias, which may have inflated the percent of patients who stated they recalled the local pharmacist counseling offer, and also inflated the percent who stated they received local counseling.
Conclusion
Among the 69% of patients who do not receive counseling from their local pharmacist and 12% who are not satisfied with the counseling received, 75% are receptive to subsequent offers of immediate telephonic pharmacist counseling. This demonstrates that an important clinical need is unmet at the time of dispensing, and that patients are interested in and willing to address this need through subsequent personalized telephonic outreach by a specialist pharmacist.
Footnotes
Author Disclosure Statement
Drs. Feifer and Greenberg, Ms. Rosenberg–Brandl, and Ms. Franzblau–Isaac disclosed no conflicts of interest.