
Abstract
Worksite-based wellness programs can be a means to improve employee health awareness and potentially reduce health care costs. The “BP Success Zone: You Auto Know” program was a worksite-based intervention to reduce the incidence of hypertension among auto workers at Chrysler LLC. This 6-month program comprised an intervention consisting of education, awareness, and support intended to intensify the engagement of Chrysler employees at moderate-to-high cardiovascular risk who were not adequately controlling their blood pressure. The 539 participants had systolic blood pressure of ≥120 mmHg, diastolic blood pressure of ≥80 mmHg, or were told by a health care provider that they had hypertension. Questionnaires compared awareness and knowledge of hypertension and lifestyle choices before and at the end of the intervention. After the 6-month intervention, mean systolic blood pressure had decreased from a baseline value of 133 mmHg to 129 mmHg (P < 0.0001) and mean blood diastolic pressure had decreased from 85 mmHg to 82 mmHg (P < 0.0001). The proportion of participants with controlled blood pressure increased from 52% to 62% (P < 0.0001) over the course of the intervention. Eighty-six percent of the participants reported that the program helped them to better understand and control their blood pressure and 84% reported that they had a better understanding of their treatment options. In conclusion, a program of hypertension awareness, education, and lifestyle modification helped to improve blood pressure control among a group of Chrysler LLC employees. (Population Health Management 2011;14:257–263)
Introduction
Worksite health promotion programs are increasingly being used to improve the health of workers with chronic diseases such as hypertension. One fourth of all employers provided some kind of wellness program in 2007, and an additional 50% reported that they planned to add wellness programs. 7
These programs have been successful at improving the health profile of employees. A program at Daimler Chrysler in Canada showed improvement in the overall cardiovascular risk profile among participants in their “Tune Up Your Heart Program.” 8 Although the majority of the patients in this program were at low cardiovascular risk at the beginning of the program, the additional shift toward lower risk was significant: At baseline, 68.5% of participants were low cardiovascular risk, 21.6% were moderate risk, and 9.9% were high risk. At the end of the study, 71.1% of the intervention group were stratified as low risk, 21.6% were moderate risk, and 7.3% were high risk. These shifts also resulted in substantial cost savings.
Employees of the Coors Brewing Company who participated in a worksite health promotion program recognized small but significant improvements in systolic blood pressure (BP) levels after the program (123 mmHg before vs 121 mmHg after, P < 0.05). 9 Another employer-based hypertension program in a Georgia public utility company resulted in a 9% net increase in the percentage of employees with a normal BP over a 3-year period (P < 0.01). 10 Employees within this company whose BP improved also improved their health, driving safety, and recertification rates, which promoted a more stable and productive workforce and reduced the long-term costs of treating hypertension for the employer.
In an effort to improve hypertension management among their employees, Chrysler LLC, the Auburn Hills, Michigan-based car manufacturer, implemented a health promotion initiative in the workplace called “Blood Pressure Success Zone: You ‘Auto’ Know.” The program combined education, awareness, and support intended to intensify the engagement of Chrysler employees at moderate-to-high cardiovascular risk who were not adequately controlling their BP.
Methods
Study design and objective
This study was a prospective, pre/post assessment to determine improvement in BP after implementation of the BP Success Zone (BPSZ) Program, an education, awareness, and support program to help participants reach BP goals based on national standards. 11 The program was instituted in a mature wellness program (>25 years) that already provided focused BP screenings 4 times per year. It was designed to address participants' specific needs and offered access to a free member Web site containing information and tools, ongoing support materials, and a “Healthy Lifestyle Action Plan.” The objective of the 6-month assessment (Fig. 1) was to measure the impact of the BPSZ Program on employees' awareness of hypertension, lifestyle modifications, and hypertension control. The program included a baseline visit, educational intervention phase, and a follow-up visit. Data collected at the baseline visit were compared with data collected at the follow-up visit to measure the impact of the program.
Timeline of the BP Success Zone (BPSZ) Program.
Employees provided informed consent for the study, which was approved by the New England Institutional Review Board, an independent institutional review board for sponsors, contract research organizations, and individual researchers across the United States.
Participant enrollment and baseline screening assessment
The study was implemented at all 32 sites of Chrysler LLC in the United States. Employees at any of the sites were eligible if they met the criteria in the screening assessment. The inclusion criteria were: age ≥18 years, completion of a consent form, and previous diagnosis of hypertension by a health care professional or a BP measurement of ≥120 mmHg (systolic) or ≥80 mmHg (diastolic) at the time of the health screening (a systolic BP between 120 and 139 mmHg and diastolic BP between 80 and 89 mmHg is defined as prehypertension by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure [JNC 7]). 11 Eligible participants were asked to complete questionnaires to measure their baseline awareness of and knowledge about hypertension and to assess their lifestyle choices including diet, exercise, tobacco use, and hypertension medication use. Participants' weight and BP measurements were also recorded. BP was measured by a member of the wellness staff per American Heart Association recommendations. 11
Intervention
This program consisted primarily of education-based interventions. Participants received 4 mailings over a 4- to 5-month period that included information on BP control, JNC 7 guidelines, 11 and checklists of questions to review with their physicians. In addition to the mailings, participants were provided with materials to help them create action plans to develop more healthy lifestyles. Web sites specific to the program provided detailed motivation for joining the program, key features of the program, a BP goal, frequently asked questions, and success stories. During the program, educational materials were offered at each worksite, and promotional banners and posters were displayed. Finally, various incentives, such as golf towels, measuring tapes, and emergency auto kits, were offered to participants through drawings at enrollment and at 6-month follow-up.
Follow-up visit
A reminder postcard was sent to all participants 2 weeks before a scheduled follow-up visit 6 months after program enrollment. At the follow-up visit, participants completed questionnaires to assess their post-intervention knowledge and awareness of hypertension and related risk factors, and their current lifestyle choices. Participants' weight and BP were measured to assess their post-intervention level of BP control and their overall cardiovascular health risk. Participant satisfaction with the BPSZ program was measured through a questionnaire that assessed their overall satisfaction and their perceived value of the program.
Subgroups
Two subgroups of participants received more intensive intervention—nutritional counseling or home BP monitors—to evaluate the impact of these interventions on BP control. Enrollment was on a first-come basis among the pool of participants with a BP value of ≥140 (systolic) or ≥90 mmHg (diastolic) (defined as hypertension by the JNC 7) at the screening visit. 11
The nutritional counseling group consisted of 100 participants from 4 Chrysler sites. These participants were to receive three 1- to 1.5-hour dietary counseling sessions with a registered dietitian and were offered an additional incentive if they participated in all 3 sessions. The other subset of 150 study participants received self BP monitors that could be used to measure BP at home.
Data collection and statistical analyses
Data collected at the baseline screening assessment and the 6-month follow-up visit were compared to assess the impact of the intervention on awareness of hypertension, lifestyle modifications, and BP control. Hypertension awareness was measured through 5 questions that assessed relevant knowledge such as hypertension prevalence and risk factors. Each question was worth 20 points for a possible high score of 100. A nonresponse was considered equivalent to an incorrect response. Mean scores were compared from baseline to follow-up. Lifestyle modifications were evaluated using questionnaires that assessed various indicators of health such as type, duration, and frequency of weekly exercise; weekly consumption of fruits, vegetables, and whole grains; and tobacco use in the previous 30 days. Means and frequencies of the responses were compared from baseline to follow-up.
The JNC 7 criteria 11 were used to define BP control. Control of systolic BP was defined as < 140 mmHg for participants without diabetes and < 130 mmHg for participants with a self-reported diagnosis of diabetes (as established by a health care provider). Control of diastolic BP was defined as < 90 mmHg for participants without diabetes and < 80 mmHg for hypertensive participants with self-reported diabetes. BP control was stratified according to whether the participant had a previous diagnosis of hypertension by a health care professional.
BP measurements were also used to assess the risk of coronary heart disease using cardiovascular risk scores based on the Framingham Heart Study. 12 Scores were calculated separately for men and women and were based on the following: systolic and diastolic BP, diagnosis of diabetes by a health care professional, smoking status in the previous 30 days, and age. Possible scores ranged from −3 to ≥14 and corresponded to a 10-year coronary heart disease risk of 2% to ≥6%. Cholesterol scores are typically included as a part of the risk assessment but were not available for this study. Therefore, the calculated score is likely a low estimate of risk in this study.
Program satisfaction was evaluated using questionnaires at the follow-up visit. Subanalyses were conducted among the nutritional counseling and home BP subgroups. Data input, validation, and statistical analyses were conducted using SAS version 9.2 (SAS Institute Inc., Cary, NC).
Results
Demographics
A total of 3675 Chrysler employees were screened for the study, and 1125 (30.6% of the screened population) participated in the program. At the end of the 6-month study, 539 (47.8%) returned to complete the follow-up survey and were included in the study. The participants were predominantly white men, married, aged ≥50 years old, and college educated (Table 1).
539 participants were included in this study. Each demographic characteristic was evaluated based on the number of participants who had complete data for that characteristic. The denominator for each characteristic is specified in the table.
Awareness of hypertension
Hypertension awareness, assessed based on 5 general knowledge questions regarding hypertension, increased over the course of the intervention. The mean score (scale 1 to 100) for all participants was 77 at the baseline survey and 80 at the follow-up survey (P < 0.01).
Lifestyle modifications
The number of participants who reported diet, exercise, and/or medication use as methods to manage hypertension increased over the course of the study. Exercise was the most common lifestyle modification (Fig. 2) at baseline and follow-up. The percentage of participants who engaged in at least 30 min of moderate exercise at least 3 times per week increased from 57% at baseline to 67% at follow-up. The average number of days participants exercised increased from 2.9 to 3.3 days per week (P < 0.0001). Use of dietary modification as a means of controlling high BP also increased significantly over the course of the study. At the end of the study, 37% of participants reported enrolling in a weight loss program, compared with 28% at baseline (P < 0.0001). Antihypertensive medication use also increased significantly over the course of the study. Monotherapy was the most common approach, used by 31.9% of participants at baseline and 34.2% at follow-up. Tobacco use decreased from 15% at baseline to 11% at the follow-up visit (P = 0.001).
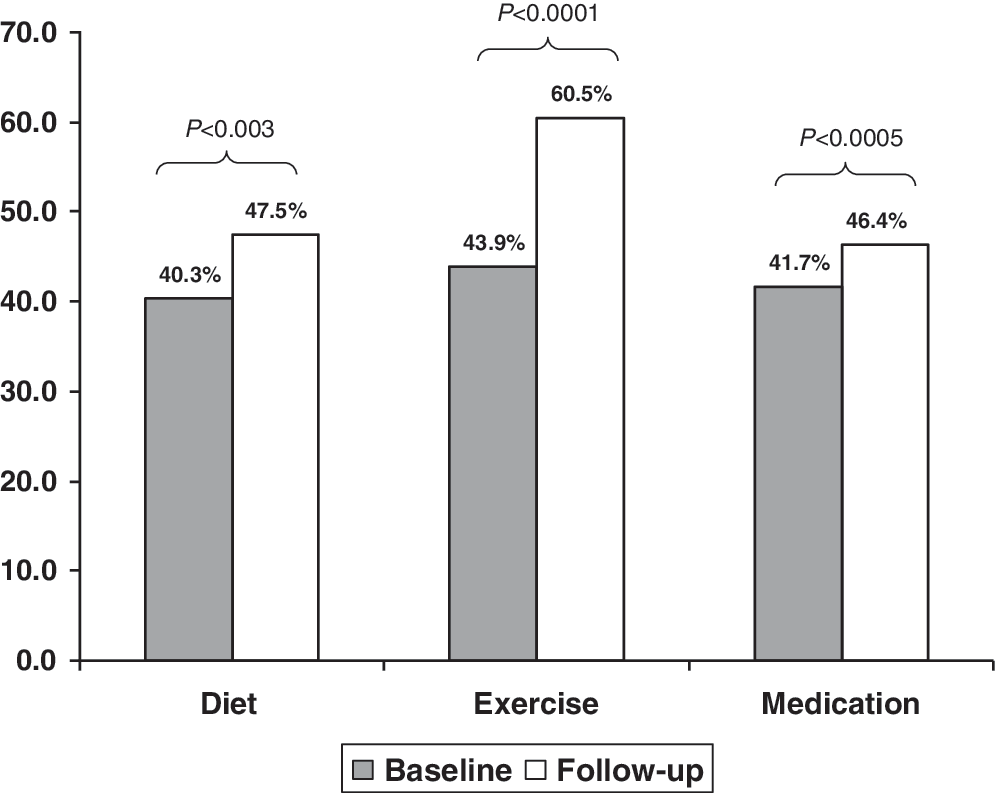
Lifestyle modifications: Methods of managing hypertension.
Blood pressure control
Mean systolic BP decreased from 133 mmHg at baseline to 129 mmHg at follow-up (P < 0.0001) and mean diastolic BP decreased from 85 mmHg to 82 mmHg (P < 0.0001). As a result, the proportion of participants with controlled BP increased from 52% to 62% (P < 0.0001) over the course of the intervention (Fig. 3). The magnitude of change in BP control was greater among participants who indicated that they had been diagnosed with hypertension by a health care professional (46% at baseline vs 59% at follow-up, P = 0.001) compared with those who had not been diagnosed by a health care professional (65% at baseline vs 74% at follow-up, P = 0.04). Among participants who were taking medication both at baseline and follow-up, the BP control rate increased from 49% to 57% (P = 0.06).
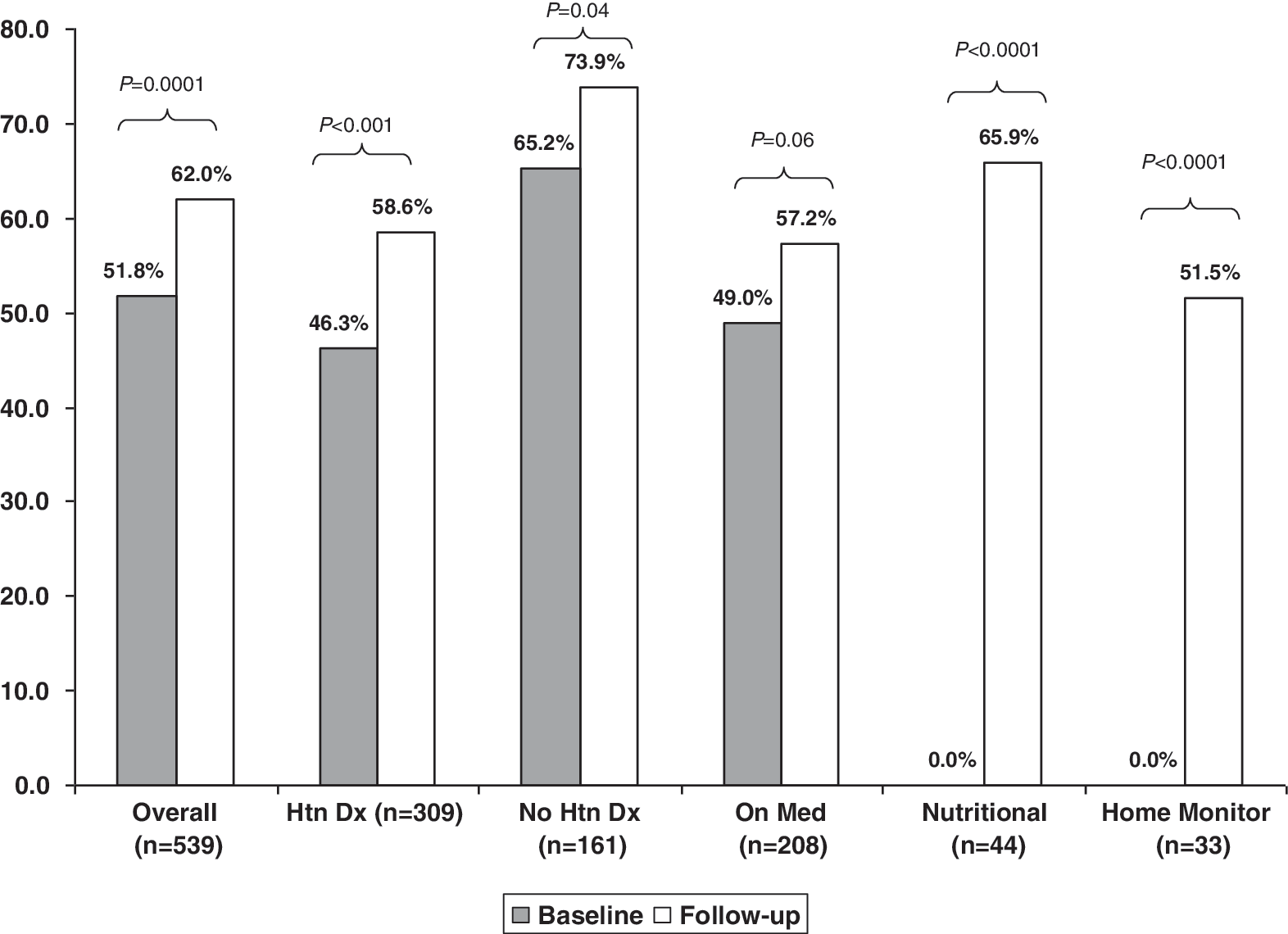
Blood pressure control comparison between baseline and follow-up.
BP measurements were used to assess the change in likelihood of coronary heart disease. Change in risk was calculated using separate score sheets for men and women based on the experience of the Framingham Heart Study using systolic and diastolic BP, diagnosis of diabetes, smoking status in the previous 30 days, and baseline age. 12 For both men and women the risk score decreased significantly (P < 0.001 for men, P = 0.03 for women) from baseline to follow-up (Fig. 4).
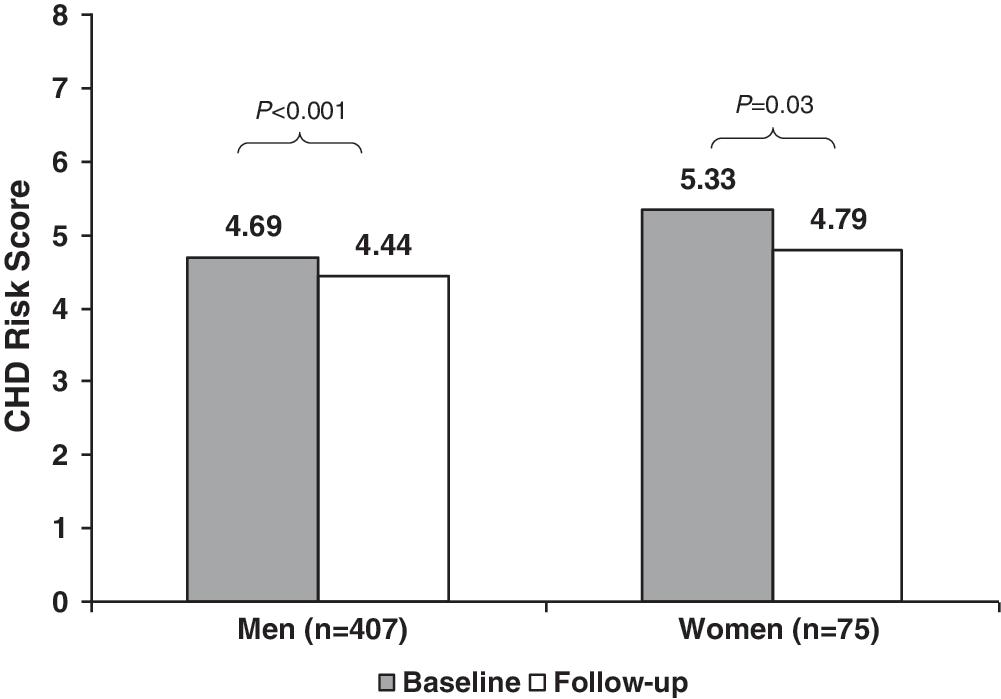
Change in coronary heart disease (CHD) risk score of Chrysler participants from baseline to follow-up.
Subgroup analyses
BP control among participants who received nutritional counseling, all of whom had uncontrolled hypertension at baseline, was 66% at follow-up (P < 0.0001 vs baseline) (Fig. 3). A total of 72% of nutritional counseling participants reported that they had decreased their sodium intake, and 82% reported that they had improved their diet as a result of the nutritional sessions. In addition, 53% reported that they had increased their exercise. Overall satisfaction with the program was reported by 84% of these participants.
Among participants who received a home BP monitor, all of whom were hypertensive at baseline, 52% had their BP controlled at follow-up (P < 0.0001 vs baseline) (Fig. 3). A total of 68% of participants reported that the monitor was helpful in tracking their BP, and 66% reported that the monitor was easy to use. Sixty-eight percent of the home BP monitor subgroup participants reported that they planned to continue using the monitor.
Satisfaction
A total of 93% of participants reported that they were satisfied with the quality of the BPSZ program and the benefits it provided. Specifically, 86% reported that the program helped them to better understand and control their BP, and 84% reported that they had a better understanding of the treatment options to improve their cardiovascular health as a result of the program. Ninety-five percent reported that the program was a good benefit offered by their employer and 94% would recommend it to a coworker or family member.
Discussion
This study was a prospective, pre/post assessment of the BPSZ Program, conducted among employees of Chrysler LLC, one of the largest auto manufacturers in the United States. The program was designed to intensify the engagement, education, and mobilization of moderate-to-high risk employees at US worksites who were not adequately managing their cardiovascular risk factors and controlling their BP. The program showed that employees who received educational interventions regarding hypertension increased their awareness of their general health status, diet, and exercise at the conclusion of the 6-month study period. More importantly, they improved their treatment and BP control.
The value of worksite-based BP control programs is supported by a 1992 study of 692 employees of the Coors Brewing Company who participated in a worksite-based health promotion called LIFECHECK. 9 One fifth of the participants had elevated BP levels. Among the 499 who completed a follow-up screening, there were small but significant improvements in systolic BP (from 123.18 ± 13.62 mmHg before the intervention to 121.33 ± 13.71 mmHg afterward) (P < 0.05). 13
Results of another employer-based study of drivers for a Georgia public utility company revealed that the proportion of employees with controlled BP increased from 71.7% to 80.0%, (P < 0.01); these results are particularly interesting in a notoriously hard-to-treat population of commercial drivers. 9 In the BPSZ program, the proportion of participants with controlled BP increased from 51.8% to 62% (P < 0.0001). Participants in the BPSZ program had a lower overall BP control rate at baseline. However, the BPSZ program participants had an absolute 10% higher prevalence of diabetes compared with the Georgia public utility company employee participants. This difference in diabetes may signify a higher comorbid population, but, more importantly, the rate of BP control in patients with diabetes is typically lower than that in patients without diabetes. 14
Participants in the BPSZ program realized a statistically significant reduction in coronary heart disease risk score. Although the changes in the risk scores were numerically small, even small differences in the risk of cardiac events can result in substantial cost implications. For example, the cost of a stroke has been shown to be $10,000, and the cost of a myocardial infarction has been reported to be in excess of $7,000. 15,16 Although the cost implications of reducing cardiac risk are well documented, the cost-effectiveness of the BPSZ program was not evaluated in this study. Previous literature indicates that the cost to implement a health promotion program at Coors Brewing Company was $22,163 for the operational budget. 9 Lowering BP by even modest amounts would be expected to overcome the operational costs resulting from reductions in costly events.
There have been limited studies published on the effectiveness of worksite health promotion programs offered by automakers. The Canadian Tune Up Your Heart Program, 8 described earlier, proved an effective intervention. A 2001 study of participants in the United Auto Workers–General Motors LifeSteps Health Promotion Program showed that improvements in health risks correlated with an increase in program participation. 13 The baseline risk of participants and their eligibility for more intensive interventions (ie, screenings, wellness programs, materials resources, health coaching, and vouchers for medical office visits) were the 2 most important factors in determining the program-related health risk changes. The authors concluded that, for a comprehensive worksite wellness program to generate favorable health outcomes and be most successful, emphasis should focus on both reducing risk factors in participants considered at higher risk of health problems and maintaining health status in persons considered to be at lower risk of health complications. Maintaining health status, as opposed to improving health status, can be considered a positive result in companies with an aging workforce or with other predominant traits that place employees at higher risk for health problems. 13
The BPSZ evaluated 2 subgroups: one that received additional nutritional counseling, and one that was provided with take-home BP monitors. To be included in these subgroups, participants were required to have uncontrolled BP (≥140/≥90 mmHg) at baseline. At follow-up, 65.9% of participants who received nutritional counseling had controlled BP. The impact of more intensive interventions is well documented. A 2003 study showed that an educational program that included multifaceted lifestyle modifications had a greater impact on BP control compared with a program that focused solely on BP control. 17 Adding a nutritional component, the Dietary Approaches to Stop Hypertension (DASH) diet, had an even stronger positive effect on BP control than providing advice only. 17 Participants in the BPSZ home BP monitoring cohort had marked improvement in control at follow-up (0% vs 51.5%, P < 0.0001). Use of home BP monitors is supported by a 2008 endorsement from the American Heart Association, American Society of Hypertension, and Preventive Cardiovascular Nurses Association. 18
The satisfaction scores from this study underscore the success of the BPSZ program. About half (48%) of participants completed the program, and 93% of these reported that they were satisfied with the quality of the program. Patient satisfaction is important in managing hypertension. A recent study designed to assess factors associated with treatment satisfaction concluded that the ability to effectively treat hypertension depends on a patient's satisfaction with antihypertensive therapy. Additionally, patient satisfaction may be improved by achieving BP control. 19
Economic impact of health intervention programs
The economic impact of health intervention programs, such as the BPSZ, are difficult to quantify over the short term, although there have been a few studies that have demonstrated cost savings through improved worker health, reduced benefit expense, and enhanced productivity. Most research to date indicates positive clinical and cost outcomes with worksite-based programs. 20,21 The Tune Up Your Heart Program at Daimler Chrysler estimated an annual cost savings of Can$793 per employee, which, when projected to the entire workforce of 13,629, amounted to Can$18,461. Although the economic impact was not determined for the BPSZ program, a cost-savings assessment of the BPSZ program based upon prior work from Towers Perrin (unpublished data, 2005) suggests that the increase in the rate of BP control (proportion of patients with BP < 140/90 mmHg) may yield a reduction in events that would save $856 per person reaching goal.
Limitations of the study
This study has limitations that must be acknowledged. About half of the study participants did not complete the follow-up visit and, therefore, were not included in the analysis. However, this was an observational study, not a clinical trial. In educational programs, dropout rates usually exceed 50%. The potential impact of this attrition on the study findings is not known; however, baseline BP control was assessed between participants included in the analysis and those who were lost to follow-up, and no significant difference was found (52% vs 50%, respectively, P = 0.5). The study also limited the follow-up analysis to 6 months; thus, the sustainability of the program is not known. Many of the study findings were based on self-reported data, which have inherent limitations such as recall bias and missing data. There is a potential confounder between employees assigned to one of the 2 subgroups and those who were not. Only patients who had an established diagnosis of hypertension were given nutritional counseling or received a home BP monitor. Presumably, these patients would have been encouraged by their physicians to use a home monitor and improve their diet, so assignment to a subgroup would not necessarily change their behavior. The study did not include a control group of nonparticipants; therefore, extraneous factors that could have affected BP status were not controlled for in this study. Finally, this was an employer-specific study, and the generalizability of the study findings to other employers and industries is not known.
Conclusions
Hypertension awareness, education, lifestyle modifications to manage hypertension, and BP control all improved following implementation of the BPSZ program among a group of Chrysler LLC employees. The participants reported high satisfaction with the program. As population health or disease management programs are increasingly being offered by employers, the findings from this study are useful in understanding the impact of these programs.
Footnotes
Author Disclosure Statement
Dr. Jackson, Ms. Kohn–Parrott, Ms. Parker, Mr. Levins, Ms. Dyer, Ms. Hedalen, Ms. Frank, Ms. Bramer, Ms. Brandt, and Mr. Doyle disclosed no conflicts of interest.