
Abstract
Limited information is currently available about medication adherence for common chronic conditions among the Medicaid population. The primary objective of this study was to assess medication adherence among Medicaid recipients with depression, diabetes, epilepsy, hypercholesterolemia, and hypertension. Factors influencing adherence were determined. The authors also assessed whether adherence influences the utilization of acute care services. The target population included nonelderly adult recipients (ages 21–64 years) who were continuously enrolled in the Mississippi (MS) Medicaid fee-for-service program from January 1, 2006 to December 31, 2007. Recipients were identified who had a medical services claim with a diagnosis of depression, diabetes, epilepsy, hypercholesterolemia, or hypertension in calendar year 2006. Within each chronic disease sample, medication adherence was determined using calendar year 2007 data for recipients who met inclusion and exclusion criteria. Recipients with adherence ≥80% were classified as adherent. Logistic regression analyses were used to determine the factors that predict medication adherence and the effect of adherence on concurrent all-cause acute care service (ie, hospitalization, emergency room visit) utilization. Approximately 24% of recipients with depression, 35.9% with diabetes, 53.6% with epilepsy, 32% with hypercholesterolemia, and 42.2% with hypertension were adherent. Within each chronic disease sample, males and whites had higher adherence than females and blacks. After controlling for demographic and disease-related covariates, recipients who were adherent had lower concurrent acute care service utilization than nonadherent recipients. Given the inverse relationship between adherence and acute care service utilization, policy makers should consider implementing educational interventions aimed at improving adherence in this underprivileged population. (Population Health Management 2012;15:253–260)
Introduction
For individuals with chronic conditions, poor medication adherence could have an adverse effect on morbidity and mortality. 5 –10 Each year, an estimated 125,000 deaths occur in the United States because of poor medication adherence. 11 In addition, poor adherence to medications has a considerable financial impact on patients, payers, and society. 2,12,13 In their study of the impact of medication adherence on health care costs in a commercially insured population, Sokol and colleagues found an increase in total health care costs for lower levels of adherence in individuals with diabetes, hypercholesterolemia, and hypertension. 13 The total economic burden of poor medication adherence is estimated to be ∼$300 billion (US) annually. 14 Factors such as cost, medication side effects, poor patient-provider relationships, patient belief systems, complexity of treatment regimen, lack of access to care, and lower levels of health literacy and English proficiency have been found to impact adherence. 15,16 Further, studies have found a relationship between socioeconomic status and adherence, with lower levels of adherence seen among individuals with a greater degree of socioeconomic disadvantage. 17
Though a great deal of literature has been devoted to studying medication adherence in general, limited information currently exists in terms of adherence in the Medicaid population. 18 Medicaid is the primary health insurance program for low-income individuals and families in the United States. Compared to the general population, individuals enrolled in Medicaid have a higher likelihood of premature mortality and hospitalization, lower literacy levels, and a higher prevalence of obesity, smoking, and alcohol consumption. 19,20 Nonelderly adult Medicaid recipients are sicker and have a greater chronic disease burden compared to the general population. 21 More than 50% of nonelderly adult Medicaid recipients have at least 1 chronic disease; more than 25% have 2 or more chronic diseases. 21 In recent years, a few studies have assessed medication adherence for different chronic diseases in the Medicaid population. 18,22 –25 These studies provide useful information concerning medication adherence in a Medicaid population; however, all of them have focused on a single disease and used different measures of adherence, a limitation that holds true for medication adherence literature in general. 26,27 In their review of administrative database-based studies of medication adherence, Andrade and colleagues highlighted the difficulty of making uniform comparisons across adherence studies because of differences in terminology, study design, and adherence measurement. 28 To overcome these limitations, a couple of recent studies have examined adherence using uniform measures across a range of chronic diseases in the commercially insured population. 26,29 A thorough review of the literature did not reveal any such previous study in the Medicaid population, wherein a consistent measure of medication adherence is used across a range of chronic diseases.
Assessing medication adherence and the common factors that influence adherence across common chronic diseases in an underprivileged population is the key first step toward developing effective and appropriate educational interventional strategies aimed at improving adherence. The purpose of this study was to determine medication adherence in nonelderly adult Medicaid recipients across 5 chronic diseases: depression, diabetes, epilepsy, hypercholesterolemia, and hypertension. Factors predicting medication adherence among Medicaid recipients were studied. The authors also studied the role of adherence in influencing the utilization of all-cause acute care services.
Methods
The study was approved by the University of Mississippi institutional review board.
Data source
This study used the 2006–2007 Mississippi (MS) Medicaid Analytic Extract (MAX) files from the Centers for Medicare and Medicaid Services (CMS) Chronic Condition Warehouse. The MAX data include claims for medical services (hospitalizations, emergency room [ER] visits, and office visits) and prescription medications for the MS Medicaid fee-for-service (FFS) program. The MAX medical services files have institutional and noninstitutional claims-level information for recipients, and include variables such as first and last date of service, amount billed and paid, diagnosis code based on International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), and Current Procedure Terminology codes. The Medicaid prescription file was used to study claims for medications dispensed in the outpatient setting. Demographic information, including age, sex, race, and location of residence, was available through the MAX personal summary file. This summary file also included monthly eligibility information for all recipients. The medical services, prescription, and personal summary file were linked using a unique common identifier. To protect patient privacy, all data were available with encrypted recipient identifications that linked claims without identifying individual recipients. The study protocol was approved by the University of Mississippi Institutional Review Board under exempt status, and data access was covered through a data use agreement executed with CMS.
Study sample
The target population for the study included all individuals who were continuously enrolled in the MS Medicaid FFS program for a period of 2 years from January 1, 2006 and December 31, 2007, and who were at least 21 years of age on January 1, 2006 and younger than 65 years of age on December 31, 2007. The year 2006 data served the purpose of sample identification, while the year 2007 data served as the medication adherence study period. From the target population, recipients were extracted who had 1 or more medical services claims (hospitalization, ER visit, or office visit) with a primary or secondary diagnosis of diabetes (ICD-9-CM 250.xx), depression (ICD-9-CM 296.2x, 296.3x, 300.4, or 311), epilepsy (ICD-9-CM 345.xx), hypercholesterolemia (ICD-9-CM 272.x), or hypertension (ICD-9-CM 401.xx-405.xx) during calendar year 2006. Among these, recipients were identified who had at least 1 prescription drug claim associated with the respective disease in the calendar year 2006. This was done to prevent the inclusion of any incident users of medications in study year 2007. Further, recipients in each of the 5 chronic disease groups who did not have any disease-related prescription fill in 2007 were excluded from analysis. Therapeutic drug classes that were considered for each of the 5 chronic diseases are listed in Table 1. Drug classes relevant to the diseases studied were identified based on the input of a practicing pharmacist and general drug literature. There were a total of 5 chronic disease study samples, which were not mutually exclusive.
Measures
Medication adherence during study year 2007 was measured across each of the 5 chronic disease samples using the methodology outlined by Hepke and colleagues. 12 Prescription claims data from October 1, 2006 to December 31, 2007 were used to assess adherence. Analyzing data from October 1, 2006 enabled the capture of disease-related medications that were filled on or after that day and carried over into 2007 (maximum 90-day fills). Two variables, “date of dispensing” and “number of days supplied,” in the prescription claims file were used to determine the possession of medication. For each day during the adherence measurement period (January 1, 2007–December 31, 2007), recipients across each of the 5 chronic disease samples were coded based on whether they possessed a medication relevant to the disease. If a recipient possessed an excess of the same drug at any given time, which could have occurred if a medication was refilled early, then the number of overlapping days were added to the subsequent fill period. For each day during the year, if the recipient possessed 1 or more disease-related medication(s), a score of “1” was given; however, if the recipient did not possess any medication related to the underlying disease, then a score of “0” was given. 12 To determine the total number of days a recipient possessed disease-related medication during the study year 2007, the medication possession outcome (1 or 0) was summed for the entire year. 12 It was assumed that if a recipient had a hospitalization claim at any time during 2007, then he or she would have received all medications for the underlying disease of interest during the hospitalization period. Therefore, the number of days the recipient was in the hospital was added to the days' supply available for relevant disease-related medications. Medication adherence percentage was calculated by dividing the summated score of the medication possession outcome by 365, and multiplying this factor by 100. 12 As is the general norm in the adherence literature, we classified recipients in each chronic disease sample into adherent or nonadherent based on whether their adherence was ≥80%.
Other variables included in the study were age, sex, race, location of residence, Charlson comorbidity index score (CCI), 30 and prior disease-related hospitalization or ER visit. For the purpose of the study, age was included as a continuous variable. Sex was classified as male and female. Race was divided into 3 categories: white, black, and other. Location of residence was defined as rural or urban, and was based on the US Department of Agriculture rural–urban continuum codes. The comorbidity profile of recipients was ascertained using the CCI score (D'Hoore modification). The calculation of CCI score (continuous variable) for recipients across each chronic disease sample was based on the ICD-9-CM diagnosis listed in the medical services claims file, and received by recipients during the calendar year 2006. Because there are no clinical indicators available in the Medicaid data, a proxy measure of disease severity was created for the purpose of this study. The authors used the medical services claims data for calendar year 2006 to determine whether recipients in each disease sample had a prior hospitalization or ER visit with a primary diagnosis of that disease. This variable was coded as “yes” or “no” depending upon the presence or absence of a prior disease-related hospitalization/ER visit. To determine whether adherence influences the utilization of acute care services, a variable indicating concurrent (calendar year 2007) all-cause hospitalization or ER visit use also was created for recipients in each of the 5 chronic disease samples. Recipients were classified into 2 categories based on whether they had a concurrent all-cause hospitalization or ER visit (coded “yes”) or not (coded “no”) in 2007.
Statistical analysis
Means and standard deviations have been reported for continuous variables, and frequencies and percentages for categorical variables. For bivariate analysis, means were compared using the Student t test, and categorical variables were compared using chi-square (or Fischer exact) test. Within each chronic disease sample, the adherent and nonadherent recipients have been compared by age, sex, race, location of residence, CCI score, prior disease-related hospitalization/ER visit, and average adherence. For each chronic disease, a logistic regression model was fitted to identify predictors of medication adherence. After controlling for other variables, the effect of medication adherence on concurrent all-cause hospitalization or ER visit use also was tested using logistic regression analysis. Odds ratios with 95% confidence intervals have been reported for the results of logistic regression. Statistical significance was considered to be P<0.05. Data management and analyses were performed using SAS, version 9.2 (SAS Institute Inc, Cary, NC).
Results
The final sample comprised 4351 recipients with depression, 7655 with diabetes, 1105 with epilepsy, 3709 with hypercholesterolemia, and 16,961 with hypertension. Figure 1 depicts the proportion of adherent and nonadherent recipients within each chronic disease sample in the MS Medicaid FFS program. Recipients with depression had the lowest adherence rate; less than one fourth were adherent (adherence rate ≥80%). The highest rate of adherence was observed among recipients with epilepsy.
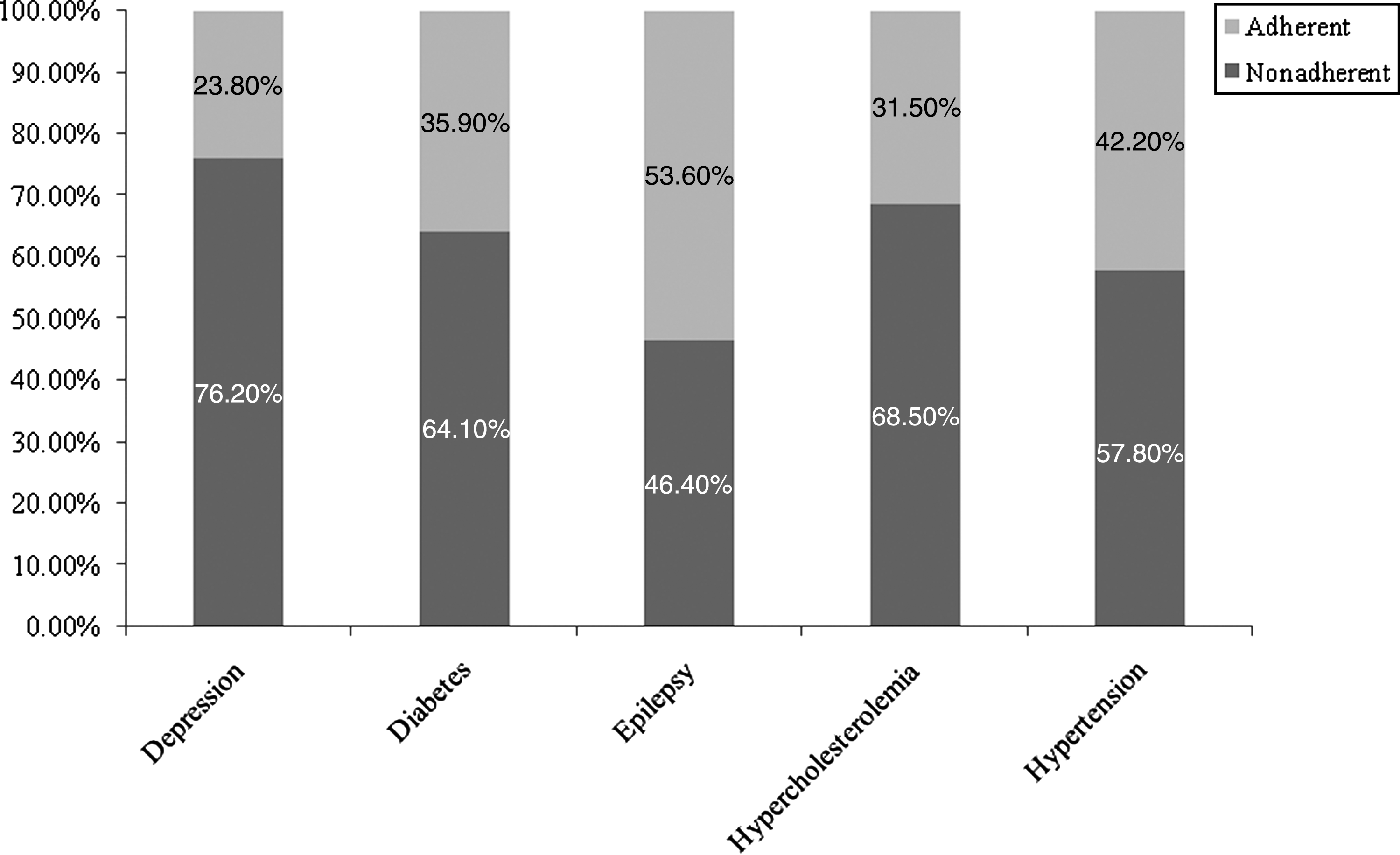
Percentage of adherent and nonadherent Mississippi Medicaid beneficiaries by disease states (2007).
Table 2 describes the results of comparisons between adherent and nonadherent recipients within each chronic disease sample by different characteristics. Significant differences between adherent and nonadherent recipients were observed for the factors of age, sex, race, CCI score, and prior disease-related hospitalization/ER visit. The average adherence score also differed between adherent and nonadherent recipients.
CCI, Charlson comorbidity index score; sd, standard deviation. 1Others include American Indians/Alaskan Natives, Asians, Hispanic/Latinos, Native Hawaiian/Pacific Islanders, and unknown. 2 P<0.05; 3 P<0.01; 4 P<0.001.
Table 3 presents the results of logistic regression analyses conducted to identify the factors predicting medication adherence. Consistent with the bivariate results, age, sex, race, CCI score, and prior disease-related hospitalization/ER visit emerged as significant predictors of adherence in the regression models.
CCI, Charlson comorbidity index score. 1Others include American Indians/Alaskan Natives, Asians, Hispanic/Latinos, Native Hawaiian/Pacific Islanders, and unknown. 2 P<.05; 3 P<.01; 4 P<.001; 5Reference category for ratios.
Table 4 summarizes the results of logistic regression analyses aimed at determining whether adherence predicts all-cause concurrent health care resource utilization. After controlling for age, sex, race, location of residence, CCI score, and prior disease-related hospitalization/ER visit, adherence emerged as a significant predictor (P<0.001) of concurrent all-cause hospitalization/ER visit use in all 5 chronic disease groups. The likelihood of concurrent all-cause hospitalization/ER visits among recipients who were adherent in comparison to those nonadherent was 41% lower in depression, 40% lower in diabetes, 37% lower in epilepsy, 44% lower in hypercholesterolemia, and 35% lower in hypertension.
CCI, Charlson comorbidity index score. 1Others include American Indians/Alaskan Natives, Asians, Hispanic/Latinos, Native Hawaiian/Pacific Islanders, and unknown. 2 P<0.05. 3 P<0.01. 4 P<0.001; 5Reference category for ratios.
Discussion
This study provides information about medication adherence among nonelderly adult recipients with common chronic conditions enrolled in a state Medicaid FFS program. Factors influencing adherence were ascertained. Further, this study highlights the prominent role played by adherence in influencing the utilization of acute care services. By using a consistent measure of adherence across 5 common chronic conditions, this study attempts to bridge the gap of measurement uniformity in the adherence literature.
With the passage of the Patient Protection and Affordable Care Act, Medicaid eligibility will be extended to adults younger than 65 years of age with income less than 133% of the federal poverty level from 2014 onward. 31 As a result, millions of low-income adults who currently are uninsured will gain coverage through Medicaid in the next few years. With increasing enrollment, it is highly likely that the cost burden of chronic diseases in state Medicaid programs will increase in the next few years. Already facing budget shortfalls because of the tough economic climate, states across the nation have employed strategies such as prior authorization and prescription caps over the past few years to save Medicaid dollars. 32 However, studies have suggested that these strategies may have unintended consequences on patient health outcomes, and are not cost-effective. 33 –35 As indicated by the results observed in this study, policy makers should focus their efforts on factors such as medication adherence, which have the potential to positively influence patient health outcomes and reduce the utilization of acute care resources.
Medication adherence was found to be highest among recipients with epilepsy (53.6%), followed by those with hypertension (42.2%), diabetes (35.9%), and hypercholesterolemia (31.5%). In a previous study of medication adherence among Medicaid recipients, Faught and colleagues found 74% of individuals with epilepsy to be adherent. 18 In their study of medication adherence across a range of chronic conditions in a commercially insured population, Briesacher and colleagues found ≥80% adherence in 72.3% of patients with hypertension, 65.4% of patients with diabetes, and 54.6% of patients with hypercholesterolemia. 26 In another study of a commercially insured population, Sokol and colleagues observed ≥80% adherence in 72.7% of patients with hypertension, 55.2% of patients with diabetes, and 58.8% of patients with hypercholesterolemia. 13 The lowest rate of adherence in this study was found among recipients with depression (23.8%). When studying adherence to antidepressant therapy among individuals with depression and/or anxiety enrolled in managed care, Cantrell and colleagues found an adherence rate of 43.3%. 36 The results of this study suggest that medication adherence is lower among individuals with chronic conditions enrolled in the MS Medicaid program compared to individuals enrolled in other state Medicaid programs or private insurance as indicated in these previous studies.
There are some plausible explanations for the low rate of adherence observed in this study compared to prior research. The current study was based on residents of a state that is one of the poorest in the country. MS has a largely rural population; 65 of its 82 counties have been designated rural. 37 Further, 75 counties in MS are officially designated as health professional shortage areas. 37 The residents of MS have one of the worst health outcomes in the country, and there is a high prevalence of chronic conditions such as diabetes, obesity, and cardiovascular diseases. Given these factors, it is no surprise that MS has consistently been ranked as the unhealthiest state in the country. 38 The unfavorable socioeconomic and environmental factors prevalent in the state are generally magnified in a Medicaid population, and could have contributed to the lower adherence seen in this study. Further, MS Medicaid has a 5-prescription cap policy, which allows recipients (with few exceptions) to fill a maximum of 2 brand-name and 3 generic medications each month. 39 Prescription caps have been shown to reduce medication adherence and negatively impact patient health outcomes. 33 –35,39 When studying the relationship between socioeconomic disadvantage and medication nonadherence, Wamala and colleagues found that individuals between ages 21 and 64 years with severe economic disadvantage were 2–5 times more likely not to fill their prescribed medications compared to those with no economic disadvantage. 17 There is a need to further study the relationship between socioeconomic status and medication adherence, especially in the context of the Medicaid population. Future studies could compare adherence for common chronic conditions among the commercially insured and Medicaid populations using a consistent measure.
When studying the factors influencing adherence based on bivariate and multivariate statistical analyses, some interesting results emerged. Across all 5 chronic conditions, male sex and white or other race were associated with being adherent. The role of sex in influencing medication adherence seems to be inconsistent. Though some studies have shown females to have lower adherence, 12,18 others have found the opposite. 22 Some studies have found that the sex of the patient does not influence medication adherence. 25,26 In this study, a lower proportion of females were found to be adherent than males in all 5 disease samples. Factors such as lack of time and limited access to specialists have been reported to be important barriers to care among females of lower socioeconomic status and/or those enrolled in Medicaid. 40 Further research is needed to identify differences between the sexes with regard to access factors in a Medicaid population, and the role these factors play in influencing medication adherence. Consistent with prior literature, 18,23,25 blacks were found to have lower adherence than whites across all 5 disease samples in this study. Given the chronic nature of the diseases included in this study, it is likely that black patients enrolled in MS Medicaid will experience faster disease progression and poorer outcomes as a result of lower adherence. Policy makers should consider targeting these 2 high-risk demographic groups (females and blacks) for interventions aimed at enhancing medication adherence.
Across all chronic conditions, medication adherence was found to be a significant predictor of concurrent all-cause acute care utilization (hospitalization/ER visit) after controlling for potential confounding factors such as age, sex, race, CCI score, and prior disease-related hospitalization/ER visit. In general, recipients who were adherent were 35%–44% less likely to have a concurrent all-cause hospitalization/ER visit. Though prior studies have reported similar results, 12,13,18 this is the first study to document the consistently inverse relationship between adherence and acute care utilization across a range of chronic conditions in a Medicaid population. As Medicaid enrollment increases in the next few years to accommodate millions of currently uninsured adults, the consumption of already scarce health care resources and the associated costs will increase. The results of this study highlight the urgent need for public payers to proactively engage in education and interventions to improve medication adherence. Policy makers could consider implementing incentive programs for health care providers to proactively engage in promoting medication adherence among Medicaid patients. Further, an increasing emphasis should be placed on the establishment of the patient-centered medical home model for care delivery, wherein patients have an interaction with a health care provider on a regular basis. Studies have suggested that the medical home model of care delivery can improve medication adherence among patients, and contribute toward lowering medical costs. 41
This study had a few limitations. The administrative claims data used for the study could have been subjected to misclassification or coding errors during claims processing. The MS Medicaid managed care data were not available for this study, thereby limiting our ability to study adherence among all MS Medicaid recipients. Also, the sample was restricted to those younger than 65 years of age because Medicare data for elderly dual-eligible recipients were not available. The adherence measure used in the study was based on prescription fills, which may or may not have translated into actual consumption of medications. The exclusion of recipients with chronic conditions of interest who had zero prescription fills in the study period (calendar year 2007) could have biased (overestimated) our results. The relationship between adherence and concurrent acute care utilization was based on cross-sectional analysis of study data; therefore, causal inferences cannot be made. Lastly, recipient demographics and prescription benefits vary from one state to another; hence, the results of this study may not be generalizable to other state Medicaid programs.
To the best of our knowledge, this is the first study to use a uniform measure of adherence across a range of chronic conditions in a Medicaid population, thereby addressing the need for standardization in adherence literature. Medication adherence was found to be low among recipients enrolled in the MS Medicaid program. Less than half of the recipients with depression, diabetes, hypercholesterolemia, and hypertension were adherent. Across all 5 chronic conditions, a lower proportion of females and blacks were adherent compared to males and whites, respectively. The impact of adherence on the utilization of acute care services also was quantified. Recipients who were adherent had a lower probability of concurrent all-cause hospitalizations or ER visits. State policy makers must focus some of their resources on identifying and removing barriers to medication adherence among this socioeconomically underprivileged population.
Footnotes
Author Disclosure Statement
Drs. Khanna, Pace, and Banahan, and Mr. Mahabaleshwarkar, Mr. Basak, and Ms. Datar disclosed no conflicts of interest.