
Abstract
Collaborative care management (CCM) for depression has been demonstrated to improve clinical outcomes. The impetus for this study was to determine if outpatient utilization patterns would be associated with depression outcomes. The hypothesis was that depression remission would be independently correlated with outpatient utilization at 6 and 12 months after enrollment into CCM. The study was a retrospective chart review analysis of 773 patients enrolled into CCM with 6- and 12-month follow-up data. The data set comprised baseline demographic data, patient intake self-assessment scores (Patient Health Questionnaire [PHQ-9], Generalized Anxiety Disorder-7, Mood Disorder Questionnaire, and Alcohol Use Disorders Identification Test), the number of outpatient visits, and follow-up PHQ-9 scores. To control for individual patient complexity and pattern of usage, the number of outpatient visits for 6 months prior to enrollment also was measured. With a logistic regression model for outpatient visit outlier status as the dependent variable, remission at 6 months (odds ratio [OR] 0.519, CI [confidence interval] 0.349–0.770, P=0.001) and remission at 12 months (OR 0.573, CI 0.354–0.927, P=0.023) were predictive. With this inverse relationship between remission and outlier status, those patients who were not in remission had an OR of 1.928 for outpatient visit outlier status at 6 months after enrollment and an OR of 1.745 at 12 months. Patients who improved clinically to remission while in CCM had decreased odds of outlier status for outpatient utilization at 6 and 12 months when controlling for all other study variables. Improvement in health care outcomes by CCM could translate into decreased outpatient utilization for depressed patients. (Population Health Management 2014;17:48–53)
Introduction
H
Previous work has demonstrated increased health care utilization for individuals with mental health disorders. In a US study of 3 health maintenance organization sites that identified “high utilizers” of outpatient health care (defined by more than 6 ambulatory visits in each of the previous 2 years) and screened 7203 willing participants for depression via the SF-20 Quality of Life Questionnaire and a modified version of the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 20% of the “high utilizers” were found to have current major depression or major depression in partial remission. When controlling for comorbidities, they found statistically significantly more ambulatory office visits, hospitalized days, and percentage of individuals hospitalized for participants with current depression compared to those with a past or no history of depression. 6
A 2001–2002 survey of 367 patients at 3 urban Boston family medicine practices (where lack of insurance did not directly impact ability to receive care) found increased use of primary care visits, emergency department visits, and nonpsychiatric hospitalizations among individuals with mental health disorders. 7 In a 2009 study of depressed veterans, those with post-traumatic stress disorder (PTSD) and depression demonstrated significantly more outpatient utilization than those who only had depression. 8 Although outcomes were not delineated, the group with PTSD had more severe depression symptoms and other comorbidities. The authors of the present study also have noted in their prior studies of patients in CCM that the patients who have increased depression severity and other comorbidities tend to have worse clinical outcomes. 9 –11
Using costs as a marker for health care utilization, a previous study has demonstrated that depression treatment makes a positive impact. A review of 9 studies in Washington state that included 1814 patients meeting criteria for depression found mean health service costs 6 months after treatment to be statistically significantly less for those who achieved remission ($2012) compared to persistent depression ($3094, P<0.001) or partial remission ($2571, P=0.007). 12 Of note, these studies utilized classic depression treatment strategies with no CCM. Total mental health per member per month costs were previously demonstrated to decrease over a 2-year period in those patients treated with CCM versus usual care. 13 This was in contrast to prior data from Washington that demonstrated long-term (4 year) cost savings, with increased costs in the first 2 years of CCM. 4
The focus of health care reform is based on the Triple Aim initiatives of the Institute for Healthcare Improvement (IHI). 14 Thus, improving clinical outcomes for the individual patient and for the population cared for in CCM must be evaluated in the context of health care utilization. The impetus for this study was to determine if outpatient utilization patterns in CCM would be associated with depression outcomes. The hypothesis was that depression remission (defined as a score on the Patient Health Questionnaire [PHQ-9 15 ] of <5) would be an independent predictor for outpatient utilization at 6 and 12 months after enrollment into CCM. Patients in CCM have improved clinical outcomes versus usual care but, within CCM, does clinical outcome affect the third IHI aim (utilization)? If remission impacts utilization, early identification and active management of those less likely to be in remission by 6 months could be implemented in an attempt to improve clinical outcomes and decrease utilization.
Methods
Patients who were enrolled in CCM in primary care clinics from March 1, 2008 through October 31, 2010 and had a complete set of intake data as well as 6- and 12-month follow-up data were included. The study cohort included 773 patients. Enrollment into CCM required a clinical diagnosis of major depressive disorder or dysthymia and a PHQ-9 score of ≥10. A clinical diagnosis of bipolar disorder was the only exclusionary criterion (not just a positive Mood Disorders Questionnaire [MDQ 16 ] screening).
After enrollment into CCM, a registered nurse care manager would review the patient with the supervising psychiatrist, who met with the care managers on a weekly basis. Any recommendations on therapeutic changes (medication or therapy) were communicated to the primary care provider (PCP). All treatment decisions were the responsibility of the PCP. Approximately 85% of patients in CCM were managed with medication therapy, generally a selective serotonin uptake reinhibitor (K.B.A., unpublished data, October 2012). Care manager to patient contact varied based on clinical need. Full details of the development and implementation of this CCM have been described previously. 5,17,18
The dependent variables were outlier status (>80th percentile) for the number of outpatient visits at 6 and 12 months. As this study was done with the primary care patients of an integrated tertiary care center, the ambulatory visits consisted of the sum of the primary, secondary, and tertiary care visits for the patient. The independent demographic variables were age, sex, race, and marital status. The clinical independent variables were baseline PHQ-9, Generalized Anxiety Disorder-7 questionnaire (GAD-7), 19 and Alcohol Use Disorders Identification Test (AUDIT) 20 score, if the MDQ score was negative (<7 on question 1 and negative on questions 2 and 3) or abnormal (any combination of a score >7, or affirmative responses), clinical diagnosis, and remission status at 6 and 12 months (PHQ-9<5). The clinical diagnosis usually was made by the patient's PCP prior to enrollment into CCM, with first and recurrent episode of depression differentiated by electronic medical record review or patient history. Previous research at the authors' institution regarding outpatient utilization had demonstrated that the individual patient's prior utilization was a significant factor in predicting subsequent outpatient utilization. 21 –25 Therefore, to control for individual patient complexity and pattern of usage, the number of outpatient visits for 6 months prior to enrollment also was measured.
Mann-Whitney testing was utilized for statistical analysis of the continuous variables and the categorical data were analyzed with chi-square testing. Multiple logistic regression modeling for outpatient visit outlier status was performed while retaining all independent variables studied. Calculations were performed on MedCalc software, version 12.3.0.0 (MedCalc Software bvba, Ostend, Belgium). This study was reviewed and approved by the Institutional Review Board of Mayo Clinic Rochester.
Results
For this cohort, the patients in remission at 6 and 12 months were older and married; sex and race were not significantly different in either grouping (Table 1). Patients in remission at either time frame tended to be diagnosed with first episode of depression, while those not in remission were more likely to be diagnosed with recurrent depression. All baseline clinical variables (PHQ-9, GAD-7, and MDQ scores) were lower in the remission group at both time frames except for the AUDIT score, which was not statistically significant in either time period. The number of outpatient visits prior to enrollment also was lower for those patients in remission at 6 months and for those patients in remission at 12 months compared to those patients not in remission at each time period.
AUDIT, Alcohol Use Disorders Identification Test; GAD-7, Generalized Anxiety Disorder-7 screen, MDQ, Mood Disorder Questionnaire; PHQ-9: Patient Health Questionnaire.
The average number of outpatient visits in the 6 months after enrollment was lower for the remission group; this also was noted in the 12-month data. Outpatient visit outlier status was defined at >8 visits at 6 months and >12 visits at 12 months. Patients in remission were noted to be statistically less likely to be an outlier for outpatient utilization at 6 and 12 months.
With a multiple logistic regression model for outpatient visit outlier status as the dependent variable, the number of outpatient visits by patients in the 6 months prior to enrollment was highly correlated to this outcome (6-month follow-up odds ratio [OR] 1.19, confidence interval [CI] 1.13–1.26, P<0.001, 12-month OR 1.77, CI 1.61–1.95, P<0.001) (Figs. 1 and 2). This is consistent with results seen in the authors' earlier studies in primary care and retail clinic settings. 21 –26 Remission status at 6 (OR 0.52, CI 0.35–0.77, P=0.001) and 12 months (OR 0.57, CI 0.35–0.93, P=0.023) was associated with the subsequent outpatient visit outlier status. With this inverse relationship between remission and outlier status, those patients who were not in remission had an OR of 1.93 (1.30–2.87, P=0.001) for outpatient visit outlier status at 6 months after enrollment and an OR of 1.75 (1.08–2.82, P=0.023) at 12 months. The patient's initial GAD-7 score was the only intake variable that was associated with subsequent outpatient utilization outlier status at 6 months (OR 1.05, CI 1.00–1.09, P=0.034). Other variables including age, sex, race, marital status, clinical diagnosis, initial depression severity, or other screening scores did not significantly impact outpatient utilization outlier status at 6 or 12 months. The multiple logistic regression for model for 6 months had a full model −2 log likelihood of 688.577 (P<0.001), while the 12-month regression had a full model −2 log likelihood of 497.752 (P<0.001).

Odds ratio for outpatient visit outlier status (>8 visits) 6 months after enrollment into collaborative care management for depression (N=773). Controlling for age, sex, race, marital status, clinical diagnosis, initial depression severity, Mood Disorder Questionnaire score, Alcohol Use Disorders Identification Test score, and site location to minimize site-to-site variability in clinical outcomes and patient enrollment characteristics. Abbreviation: GAD-7, Generalized Anxiety Disorder-7 screen.
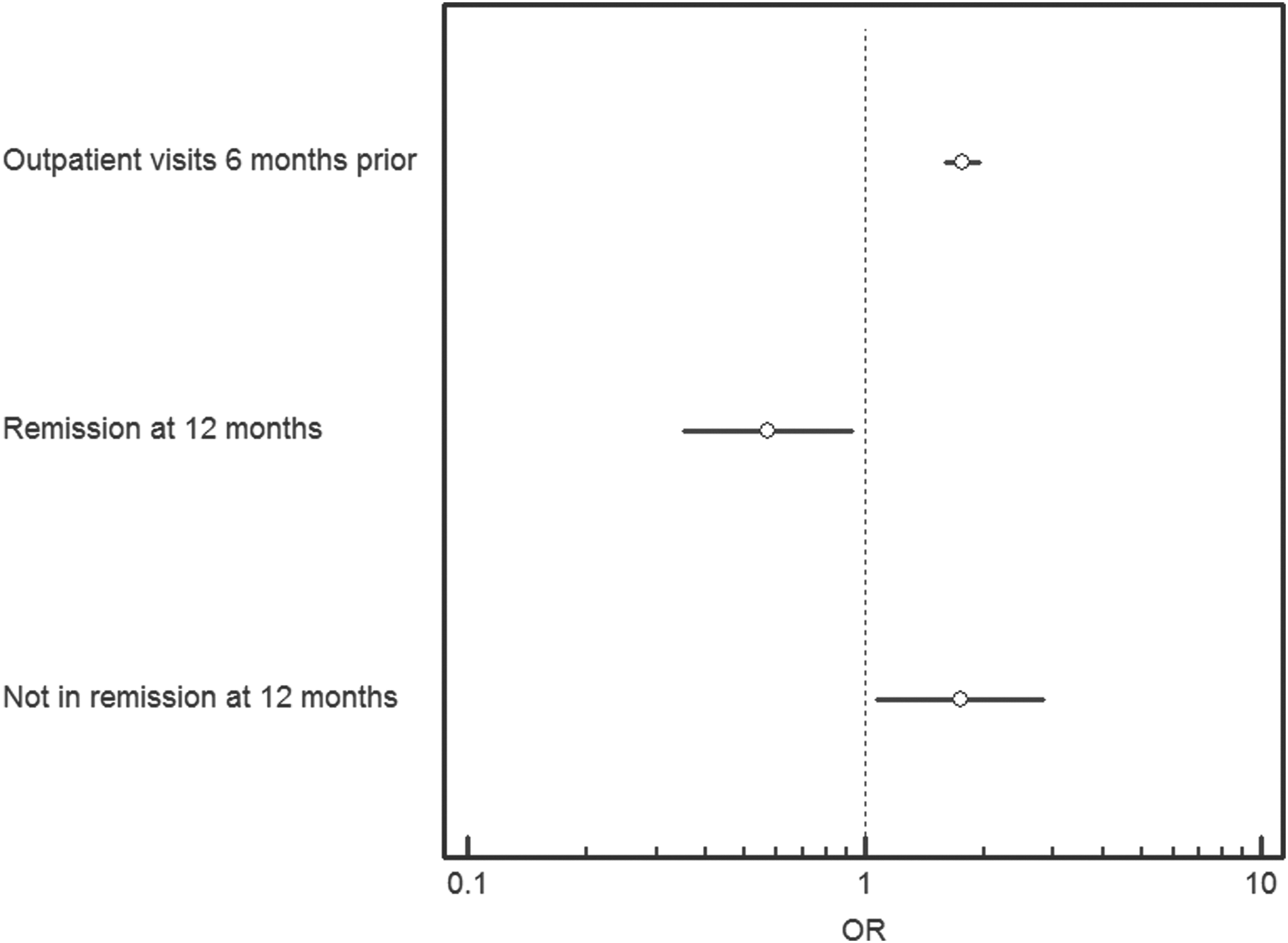
Odds ratio for outpatient visit outlier status (>12 visits) 12 months after enrollment into collaborative care management for depression (N=773). Controlling for age, sex, race, marital status, clinical diagnosis, initial depression severity, Mood Disorder Questionnaire score, Alcohol Use Disorders Identification Test score, Generalized Anxiety Disorder-7 screen score, and site location to minimize site-to-site variability in clinical outcomes and patient enrollment characteristics.
Discussion
In depressed patients in CCM, outpatient utilization after enrollment was significantly associated with improving the clinical status to remission, even when controlling for the individual patient's prior utilization patterns. Except for anxiety severity and prior outpatient visits, all other baseline variables had no significant effect on utilization. In the authors' patient population, it has been demonstrated previously that patients with severe depressive and anxiety symptoms, along with an abnormal MDQ and a clinical diagnosis of recurrent depression, have a 42.1% risk of persistent depressive symptoms (PDS) at 6 months, versus 6.6% for a patient with a moderate first episode of depression without anxiety or mood disorder issues. 27 In a goal to further enhance patient outcomes and now utilization reduction, active management of patients at higher risk for PDS would be encouraged. This active management would be consistent with the Triple Aim initiative. 14
These results are validated by their consistency with previous studies that also showed increased health care utilization by patients diagnosed with anxiety. 28,29 One study of 500 primary care patients in Connecticut showed that patients with anxiety or depression were likely to be consistently high utilizers of primary care services, with anxiety having a higher correlation than depression. 28 Similarly, a study of 3300 patients in Germany found that, although a depression or anxiety diagnosis resulted in higher health care utilization and health care costs, coexisting depression and anxiety were associated with higher utilization and costs than either diagnosis alone. 29 Although the present study was limited to CCM for patients with depression, future studies could examine the effects of CCM for patients with anxiety as the authors' institution develops a program for anxiety CCM.
In this study, as in their previous work, 21 –25 the authors adjusted for patterns of use for medical care by including the number of outpatient visits in the previous 6 months as a covariate. This variable reflects both the biomedical need for services and any psychological tendencies for the patient to seek care. By adjusting for prior use of service, the authors were able to separate out how much depression remission changes use of service above and beyond the normal pattern.
This analysis, however, did not differentiate impact on the number of visits variable between the need for medical service as reflected by medical comorbidity versus psychological factors. Disentanglement of medical comorbidity and psychological factors such as self-efficacy 30 would produce thinner slices of depressed patient types and their influence on health care utilization and costs. The attenuated depression subtypes would in turn inform CCM intervention.
The number of medical visits used in the previous year offers certain advantages as a case mix adjuster in studies of primary care patients. Visits can be counted easily, with fewer coding difficulties. Visit counts reflect both the clinical need for medical care and the psychological factors that may cause a patient to habitually seek care. And in studies in which visit counts have been used as a covariate, visits have been shown to have significant predictive validity both for return visits and for costs. 21 –25
Future studies that examine total health care costs (per member per month) in individuals within the CCM program would be interesting. Currently, the authors are evaluating the outpatient utilization patterns of patients in CCM versus those treated with usual care at their institution. Limitations of this study include the lack of racial and economic (such as health insurance coverage) diversity in the population. Because this study encompassed 1 large midwestern US medical practice, the results may not be able to be generalized to other clinical sites. As this study was evaluating clinical outcomes and not individual therapies, variations in outcomes by therapeutic choice (though not expected) could impact results.
Conclusion
Prior studies have demonstrated the effectiveness of CCM for the treatment of depression in primary care. In this study, it was demonstrated that those patients who improved clinically to remission while in CCM had decreased odds of outlier status for outpatient utilization at 6 and 12 months, when controlling for baseline severity of depression, clinical diagnosis, anxiety symptoms, and prior utilization patterns. Improvement in health care outcomes by CCM could translate into decreased outpatient utilization for depressed patients.
Footnotes
Acknowledgments
Isaac Johnson, MBA, and Julie Maxson, BA, assisted with abstraction and collection of the data.
Disclosure Statement
Drs. Oberhelman, Rohrer, Meunier, Rasmussen, and Chappell declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr. Angstman has a consulting agreement with Tamber Health. Tamber Health was not involved in study design, data analysis, or manuscript preparation. Departmental funds were used for this research; no outside funding was received.