
Abstract
In California, 1 in 3 hospital beds are occupied by adults with diabetes. The aim of this study was to examine whether diabetes impacts length of stay (LOS) following common elective orthopedic procedures compared to nondiabetic individuals, and also the performance of hospitals across California for these procedures. Using the Public Use California Patient Discharge Data Files for 2010–2012, the authors examined LOS for elective discharges for hip, spine, or knee surgery (n = 318,861) from the total population of all discharges (n = 11,476,073) for 309 hospitals across California. In all, 16% of discharges had a codiagnosis of diabetes. Unadjusted average LOS was 3.11 days without and 3.40 days with diabetes (mean difference 0.29 [95% confidence interval (0.27, 0.31) days, P < 0.01]). After adjusting for covariates, diabetes no longer resulted in a significant difference in LOS. However, the presence of common comorbidities did significantly impact LOS. Average LOS for patients with diabetes also varied widely by hospital, ranging between −50% and +100% of the mean LOS for all hospitals. Diabetes does not prolong LOS after orthopedic procedures unless comorbidities are present. Nevertheless, across California there is significant variation in LOS between individual hospitals, which may inform the decision-making process for prospective patients and payers.
Background
I
Unfortunately, rates of all types of diabetes are continuing to rise in the United States, with an excess burden especially affecting older people, a group with a substantial burden of other comorbidities. 6 As a corollary, the number of elective orthopedic procedures in older people also continues to increase, reflecting changes in population demographics. 7,8 For patients who require an elective surgical procedure in California, geographical location appears to be important and the likelihood of being referred is often determined by the referring physician's preference rather than the patient's. 9
With a move toward more personalized medicine, it would seem prudent to examine the outcomes for elective procedures to allow for a more informed choice by people with diabetes. Therefore, the aim of this study was to examine the impact of a diagnosis of diabetes on LOS for common orthopedic procedures across California and also to compare individual hospitals' LOS for these discharges with and without a diagnosis of diabetes.
Methods
The research team used the Public Use California Patient Discharge Data Files 2010–2012 from the California Office of Statewide Health Planning and Development (OSHPD,
Surgical procedures were identified by Medicare Severity Diagnosis-Related Group (MS-DRG).
10
Spinal surgeries were identified by MS-DRG 460 and 473 (spinal fusion except cervical without major complications or comorbidities [MCC] and cervical spinal fusion without MCC). MS-DRG 470 (major joint replacement or reattachment of lower extremity without MCC) consists of both hip and knee surgeries. These patients were further divided into hip and knee surgeries according to their diagnosis code, including severity (International Classification of Diseases, Ninth Revision [ICD-9]. See online Appendices, available at
Extensive diagnostic data are available in the OSHPD files, making it necessary to group diagnoses by condition categories. Diagnoses were grouped into diagnostic categories using the Chronic Disability Payment System (CDPS) grouper model version 6.
11
This model maps ICD-9 codes to 67 disease categories for risk-adjustment purposes. Disease categories were used to identify and stratify type 1 and type 2 diabetes patients as well as to identify comorbid independent variables for a generalized linear model analysis (to be detailed in the following section). ICD-9 mapping to CDPS categories is available at
Model
A generalized linear model was used to model the link between the expected LOS and the explanatory variables (and some of their interactions) in the data set. More specifically, a quasi-Poisson model was used to allow for overdispersion and to adjust for inference. The dispersion parameter was found to be significantly smaller than 1 (ie, the value used for the Poisson model), suggesting that the latter would not have been appropriate. Because of the large size of the data, it was not computationally feasible to include a random effect to account for the dependence created by the variable “hospital.” Therefore, this variable was added with each hospital as a fixed effect. The final model was obtained using the quasi-maximum likelihood estimator and significant parameters were selected using a backward model selection procedure. Indeed, some of the parameters of the initial (full) model were found to be nonsignificant (at the 95% confidence levels) and the “least significant” parameter was removed and the model re-estimated until all variables kept in the model were associated to at least 1 significant parameter. The final model contains 724 parameters and explains approximately 35% of the observed deviation.
Application of the model
Let
where
The following example illustrates the application of the model parameters. Assume that the variable “Poverty” changes by δ%. Then the effect on LOS, Δ (change in LOS as a percentage) is calculated as
And therefore if δ = 5,
Results
The total number for all discharges in California for the study period was 11,476,073 for all procedures. The number of patients having the orthopedic procedures was 318,861. The number of these patents with an additional diabetes diagnosis was 52,895 (16.6% of the total).
Unadjusted LOS
Raw (unadjusted) LOS for patients with and without diabetes is shown in Table 1 for each procedure. Overall, the unadjusted average LOS for all patients was 3.11 days (without diabetes) and 3.40 days (with diabetes). The difference (0.29 days or 9.3%) related to diabetes was significant (mean difference 0.29 [95% confidence interval (0.27, 0.31) days, P < 0.01)]. For specific procedures, Table 1 shows that in all cases (with the exception of the very few observations for knee replacements for type 1 diabetes high-risk individuals) patients with diabetes experienced a longer unadjusted LOS.
LOS = length of stay; SD = standard deviation.
Adjusted LOS
After adjusting for the covariates available for the study, diabetes alone no longer resulted in a significant difference in LOS (Table 2). However, this comparison is likely to be unrealistic because of the presence of comorbidities in the case of most patients with diabetes. 15 Table 3 shows the percentage increase in LOS for patients with diabetes and selected comorbidities.
Standard deviation in parentheses. Results were obtained using the function glm in R. The P values for the test H0 : β = 0 against HA : β ≠ 0 intervals are represented by asterisks using the following convention: *** if p∈ (0.0, 0.001); ** if p∈ (0.001, 0.01),and * if p∈ (0.001, 0.05). Note that †denotes an increase of 104 “units” and ‡denotes an increase of 5 “units.”
The Chronic Disability Payment System model defines 2 severity levels for type 1 diabetes (High and Medium) and 2 levels for type 2 diabetes (Medium and Low). For cardiac and kidney comorbidities, there are 4 levels of severity. For cardiac: Very High (VH), Medium (M), Low (L), and Extra Low (Cardiac); for kidney: Extremely High (EH), VH, M, and L. Specific diagnosis codes that map to these severity levels may be found in online Appendix 1 (available at
LOS by hospital
The average LOS for patients with diabetes varies widely by hospital, after adjusting for the covariates in the model. The range of reported LOS varies between −50% of the mean and +100% of the mean LOS. These differences are illustrated graphically in Figure 1.
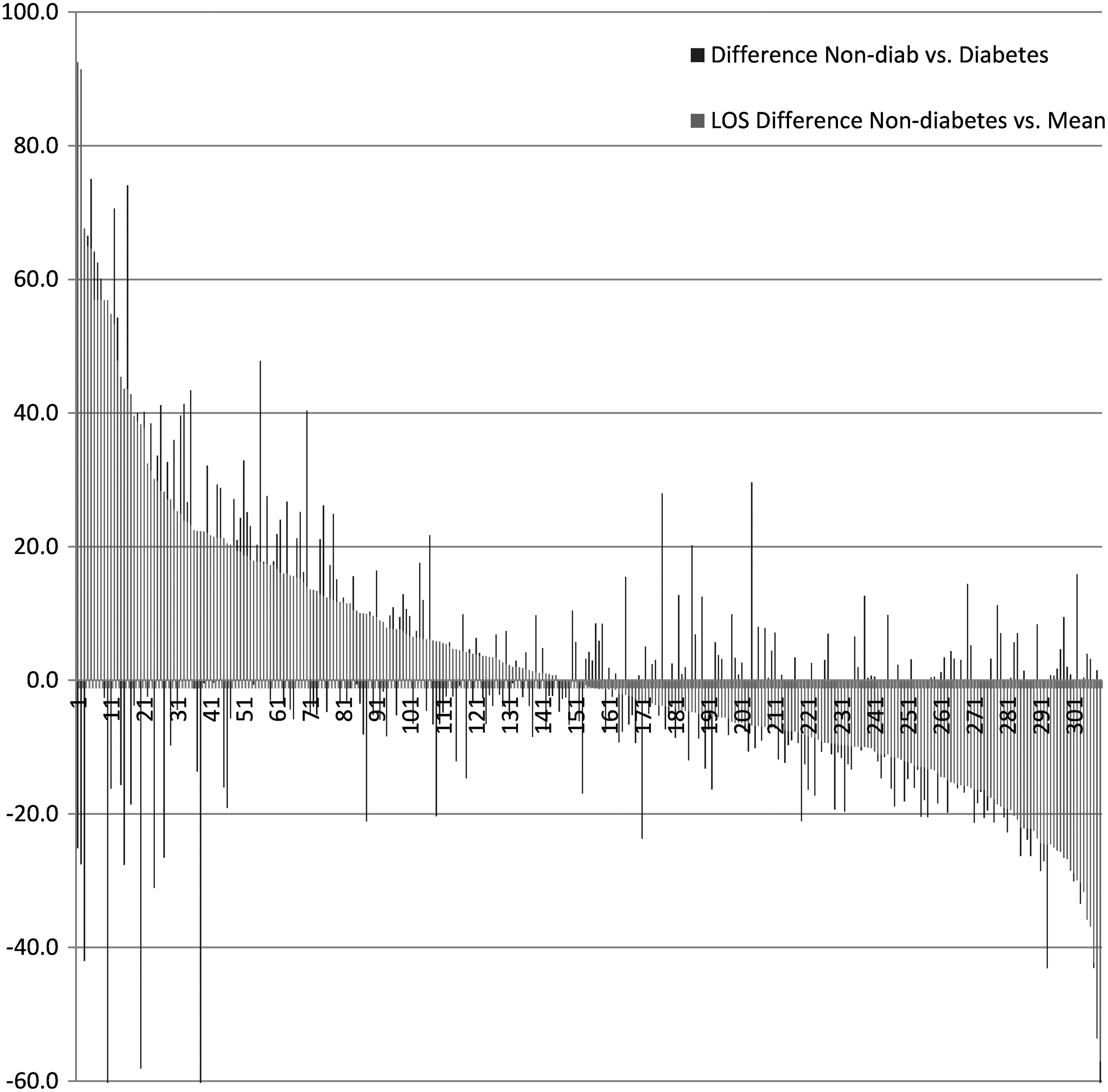
Difference in non-diabetes and diabetes patients' length of stay (LOS) relative to the mean LOS for non-diabetes patients, by hospital.
In Figure 1, all hospitals are ranked by their LOS relative to the mean for non-diabetes LOS. Thus, hospitals with a relative non-diabetes LOS higher than the mean for all hospitals are to the left of the graph, and those with a LOS lower than the mean are to the right. The bars superimposed on the graph are the relative LOS for each hospital for patients with diabetes. A bar that lies above the non-diabetes graph implies a longer LOS for patients with diabetes than nondiabetic patients; a bar that lies below the non-diabetes graph implies a shorter LOS for patients with diabetes. Data on individual hospital performance is available on request.
Discussion
In the United States, hip and knee replacements are some of the most common surgeries that Medicare beneficiaries receive. In 2013, there were more than 400,000 of these procedures costing more than $7 billion for hospitalization alone. Although some incentives exist for hospitals to avoid postsurgery complications that can result in readmissions to the hospital, or protracted rehabilitative care, the quality and cost of care for these hip and knee replacement surgeries still vary greatly among providers (
This study examined hospital admissions for elective procedures in California hospitals and specifically the impact of a diagnosis of diabetes using a large, publicly-available database. This study found that, on an adjusted basis, diabetes does not add significantly to LOS. However, the presence of common diabetes comorbidities (heart and kidney disease) does have a significant impact on LOS. This study also compared LOS by hospital, which allowed for the modeling of individual hospital performance for this measure, both for the general population and the population with diabetes. Study results indicated wide variations in performance for California hospitals for patients with and without diabetes who were admitted for common elective orthopedic procedures, even after adjusting for covariates such as race, poverty, and comorbidities.
Over recent years the number of elective orthopedic procedures in older people has risen, reflecting changes in population demographics. 7,8 For spinal orthopedic procedures, the duration of hospital stay appears to be prolonged in the presence of diabetes and advancing age, 16 although this is not a consistent finding for knee or hip surgery. 17 –19 A number of studies have examined the effect of a diabetes diagnosis (as well as other chronic conditions) on hospital LOS in patients with high-frequency elective procedures (knee replacement, hip replacement, and spinal fusion). The results have been inconclusive, some suggesting that a diabetes diagnosis was associated with longer LOS after knee 20 or hip surgery, 21 while other studies have reported little or no difference relative to patients without diabetes. 22 Elsewhere, others have reported that patients with multiple comorbidities do have a longer LOS after knee surgery, and that diabetes was the second most common condition, increasing LOS by 20%. 20 Norris and Parker also have shown an increased risk of extended LOS for patients undergoing hip surgery. 23 However, a later report suggested that a diagnosis of diabetes was uncorrelated with increased risk of postoperative complications after hip fracture surgery among geriatric patients. 22 In terms of the effect of hospital characteristics, greater hospital volume of orthopedic procedures does appear to result in shorter average LOS for certain orthopedic procedures. 21
As mentioned earlier, the presence of diabetes-related comorbidities does appear to prolong LOS for common orthopedic procedures. The US Centers for Disease Control and Prevention has reported that more than 70% of adults with diabetes have hypertension, 65% have hyperlipidemia, 30% have microvascular disease in the eye, and rates of heart disease and stroke are 1.5 to 1.8 times the frequency seen in the background nondiabetic population. 24 Estimates of the prevalence of chronic kidney disease related to diabetes range from 10% to 40% for both type 1 and type 2 diabetes, depending on the definition of the disease used. 25 –27 Moreover, diabetic kidney disease is known to carry with it substantial morbidity and mortality. Persons with diabetes are already at high risk for cardiovascular disease, and the additional development of kidney disease markedly amplifies their risk for cardiovascular disease and death. 28 The costs of dealing with diabetes as a comorbidity already add a significant financial burden overall; diabetes is expensive for any health care system, with estimates suggesting that the average cost per individual is more than $2,200 greater compared to nondiabetic individuals admitted for identical reasons. 3 The additional variation in LOS seen in the present study will further add to health care costs depending on individual hospital providers.
Overall, in California, length of hospital stay for patients with diabetes increases as the income level decreases, and readmission rates to hospital in California average 26% within 3 months of discharge, almost 90% of which are unscheduled and at least one fifth of which preventable. Patients with unscheduled readmissions are also likely to have a higher comorbidity burden, be members of minority groups, and live in lower income neighborhoods. 3 As mentioned earlier, the reasons for an increased LOS associated with diabetes are likely to be multifactorial, including more complex disease, presence of diabetes-related complications, lack of access to a structured program to optimize glycemic control prior to admission, and delays related to problems with glucose management, although access to an in-hospital specialist diabetes team can ameliorate some of the latter difficulties for elective and nonelective admissions. 29,30 Nevertheless, patients likely will want to know facility- as well as procedure-based risks and benefits, and this type of information has the potential to aid the decision-making process for elective surgical procedures where provider choice is available.
Most health care systems have adopted strategies aimed at reducing hospital LOS for orthopedic procedures. 31 When comparing LOS between hospitals, a longer duration does not always reflect lower standards of care. Recently the relationship between inpatient LOS after hip fracture and risk of death after hospital discharge was investigated using a large national population database in Sweden. 32 In that study, a shorter length of hospital stay was associated with an increased risk of death within 30 days of hospital discharge. For orthopedic procedures, too early a discharge, especially if into community care that lacks appropriate resources and rehabilitation facilities, could put patients at risk of adverse outcomes. The California Hospital Discharge Files data set used in the present study did not allow the research team to provide mortality of readmission rates. Additional information may be obtained by special request to the OSHPD.
Given the prevalence of diabetes and the significant variance between hospitals in terms of LOS for patients undergoing elective procedures, more research is needed at the hospital level to determine the factors that lead to longer or shorter LOS and also to provide data on mortality and readmission rates, both of which would be of significant interest to patients and payers. Payers also may wish to take these results into account when constructing preferred networks and contracting with hospitals. 33 Most importantly, patients undergoing elective orthopedic procedures may wish to know outcomes that matter directly to them such as expected LOS, especially if they have diabetes, to allow them to make an informed decision.
Footnotes
Author Disclosure Statement
Drs. Kerr and Guerrier, and Ms. Yadollahi, Mr. Bautista, Mr. Chen, Ms. Dong, Mr. Laan, and Mr. Duncan declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.