
Abstract
Having access to adequate and appropriate food is a major population health issue. This study investigated food insecurity in patients with high rates of inpatient hospitalization (“super-utilizers”). Forty adults with ≥3 hospital inpatient admissions within a 12-month period were interviewed in an urban hospital in Philadelphia, Pennsylvania, between March 2015 and May 2015. Inpatient admission history was obtained from hospital billing data. The majority had ≥5 hospitalizations in the past 12 months and ≥6 chronic conditions. Using the USDA definition of food insecurity, 30% (95% CI, 17% to 47%) were food insecure and 25% (95% CI, 13% to 41%) were marginally food secure. Forty percent responded that, in the past 30 days, they worried that their food would run out; 35% that their food would not last; 17.5% that they did not eat for a full day; and 10% that they were hungry but did not eat some or all of the time. Additionally, 75% were unable to shop for food on their own and 58% were unable to prepare their own food. More than half reported using food pantries or other community food resources. The impact of unmet food needs on hospital super-utilization warrants further investigation. Interventions that educate and connect patients with unmet food needs to community resources can help engage patients in their own health and well-being. Communication with patients about whether they have enough nutritionally appropriate food for their health conditions is an important starting point.
Background
T
Super-utilizers have become increasingly important for population health management. Super-utilizers are costly to the health system and to payers. Although it is recognized that super-utilizers have multiple and complex health and social needs, the nature and extent of their “nonmedical” issues are not well understood. This study investigates those needs related to food insecurity.
Access to nutritionally adequate food is a major population health issue and a relevant concern in patients with frequent hospital admissions. 8 In 2014, an estimated 15.4% of American households reported that the food intake of 1 or more household members was reduced and eating patterns were disrupted some time during the year because the household lacked money or other resources for food. 9 The health consequences associated with limited access to healthful foods has received substantial attention. For example, health conditions such as diabetes, hypertension, cardiovascular disease, and obesity have been associated with diet. 10 –12
In order to improve our knowledge and understanding about the ways in which food access and food insecurity may be present in hospital super-utilizers, the research team designed a qualitative, exploratory study. The team used the United States Department of Agriculture (USDA) definition and quantitative assessment of food insecurity. The team also examined food access and specific ways in which patients living with multiple health problems depended on others to obtain and prepare food, potentially rendering them vulnerable to food insecurity. Hospital super-utilizers were defined as patients with ≥3 inpatient admissions during a 12-month period. 13
The study was approved by the Institutional Review Board of the Einstein Healthcare Network in Philadelphia. Written informed consent was obtained from all study participants (hereafter referred to as patients).
Methods
Setting
The study site is a 770-bed tertiary care teaching hospital located in North Philadelphia, serving a primarily low-income, minority patient population. Almost one half of the population in the surrounding zip codes live at or below 200% of the Federal Poverty Level (FPL); 40% of those households have an annual income of $25,000 or less. 14
Identification of study patients
A qualitative approach with a purposive sampling frame was used in order to examine the range and expression of food insecurity in patients who were super-utilizers. 15,16 Daily inpatient admission reports that identified currently hospitalized adult patients who had ≥3 admissions to the hospital within a 12-month period were prepared for the study. The research team excluded patients admitted to critical care units, psychiatry, or labor and delivery. Other than those exclusions, the team did not select based on reason for admission. The reports provided room location, reason for current admission, number of previous admissions within 12 months, and the physician of record. The team contacted care providers of potentially approachable patients to ascertain whether the patient would be capable of participating in a brief interview. After confirming capability, a member of the research team went to the patient's room. Those requiring full medical contact precautions (posted outside the room) were not approached. Patients who were in the room and awake were told of the study and, if interested, engaged in an informed consent discussion. Those who were not in the room (presumably for testing or a procedure) or otherwise unavailable (eg, asleep, with visitors) were reapproached later in the day. After 3 unsuccessful contact attempts, the patient was dropped from the recruitment list. In all, 40 patients were enrolled and interviewed (Fig. 1).
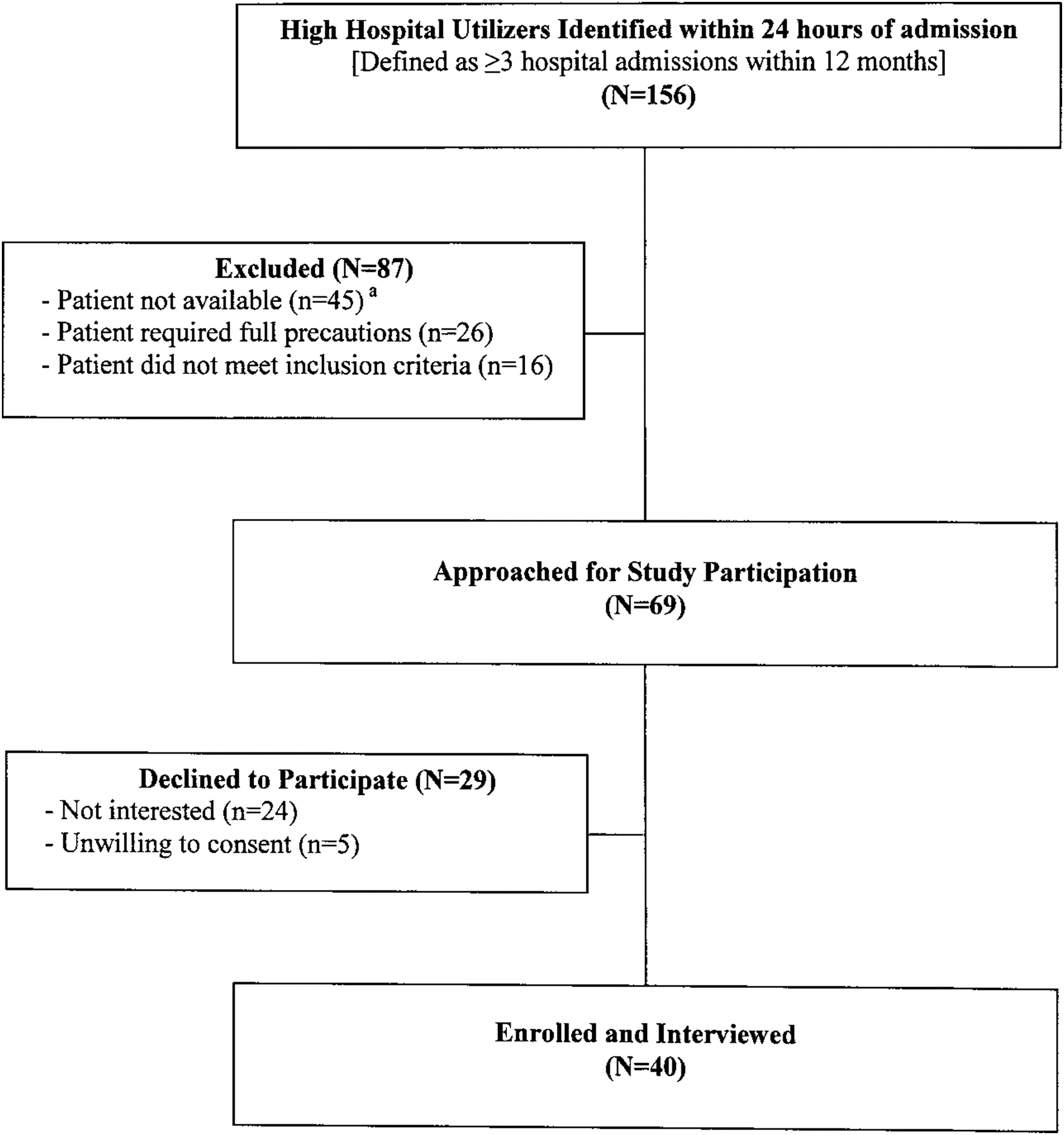
Flow of study participation.
Medical history
The research team obtained patient hospitalization history at the study institution from consenting patients including all associated International Classification of Diseases (ICD)-9 and ICD-10 diagnostic codes. These were obtained from hospital billing data for the past 12 months for all patients interviewed. To determine the number of chronic conditions and comorbidities for each patient, the team used the Healthcare Cost and Utilization Project Chronic Condition Indicators software, which categorizes all 5-digit ICD-9 diagnosis codes into chronic and not chronic. 17 Results were reviewed by a physician (HDH), consolidated to avoid redundancy (eg, diabetes mellitus type 2 with complications, diabetes circulation disorder, type 2) and retabulated.
Survey instrument
The research team developed a brief 27-item survey (average completion time 20 minutes) in order to minimize the burden on the hospitalized study patient. Questions addressed sociodemographics, self-reported health, food insecurity, ability to purchase and prepare food, and use of food banks and other food programs. To assess food insecurity, the team used 7 of 10 questions from the United States Adult Food Security Survey Module
18
with a 30-day “look-back” period. Participants were asked to respond to the following statements, indicating whether, during the past 30 days, the statement was true for them and/or the frequency with which the statement was true: • “The food that [I/we] bought just didn't last, and [I/we] didn't have money to get more.” • “[I/we] couldn't afford to eat balanced meals.” • Did [you/you or other adults in your household] ever cut the size of your meals or skip meals because there wasn't enough money for food? • Did you ever eat less than you felt you should because there wasn't enough money for food? • Were you ever hungry but didn't eat because there wasn't enough money for food? • Did you [you/or other adults in your family] ever not eat for a whole day because there wasn't enough money for food? • How true is this statement to you: “[I/We] worried whether [my/our] food would run out before [I/we] got money to buy more.”
The research team eliminated 3 questions. One question related to weight loss, which the team felt might not be a relevant indicator of food insecurity given that these patients were currently hospitalized for failing health and may not have been eating normally. The 2 others were follow-up questions that used a 1-year time frame, which was beyond the scope of interest.
Following the USDA cutoff point, patients were defined as food insecure if they answered some of the time or all of the time to 3 of the 7 questions. Those who answered 1 or 2 questions affirmatively were considered to be marginally food secure.
19,20
Selected probes in the form of an open-ended question such as, “Can you tell me more about that?” encouraged patients to elaborate on their responses and provided additional qualitative data. Interviews were conducted in patient rooms, digitally recorded, and transcribed verbatim. Questions used are provided in online Appendix A (available at
Statistical analysis
Descriptive statistics included group frequencies and percentages. Bivariate analyses examined associations between assessed characteristics and household food insecurity. Fisher's exact test compared percentages. Strength of association for rank variables was assessed using Spearman's rank correlation. Mean ages of food secure and food insecure patients were compared using independent sample t tests. Ninety-five percent exact binomial confidence intervals (95% CI) were computed. P values ≤0.05 were considered statistically significant. All statistical tests were 2-sided. Statistical analyses were performed using Stata 13 (StataCorp LP, College Station, TX).
Qualitative analysis
Qualitative methods and procedures were used to analyze narrative responses to open-ended questions and probes. 15,21,22 Two members of the study team (SBS, CAC) separately read and open-coded (labeled) the first 10 interviews by highlighting words and sections of related sequences. The preliminary labels were discussed with the Principal Investigator and a coding scheme with definitions was prepared. Both investigators recoded the same 10 interviews with the new coding scheme and reviewed results. Interrater reliability was established using Kappa. Disagreements on codes were discussed and resolved. Using the final coding scheme, all transcripts were independently (re)coded.
Results
Patients
The majority of the super-utilizers were African American and female. The average age was 60.5 years (SD 16.5). Almost half of the study group resided in zip codes where more than 30% of the population lived below the FPL (Table 1). 14
SD, standard deviation of the mean.
Does not equal 40 (100%) because 2 patients refused to answer.
Does not equal 40 (100%) because 1 patient was homeless.
Source: US Census Bureau, American Community Survey, 2009–2013, five-year estimate.
Medicaid application was completed during hospital admission.
About 43% had ≥5 inpatient admissions to the study hospital in the previous 12 months. The majority had ≥6 chronic conditions. The following chronic conditions were present in at least one third of the patients: diabetes mellitus (present in 62.5% of the 40 super-utilizers), hypertension (47.5%), hyperlipidemia (45%), chronic kidney disease (40%), gastro-esophageal reflux disease (40%), and coronary artery disease (32.5%). (Data not shown.) The majority (88%) rated their health as either fair or poor at the time of interview. Multiple health problems and dependency on others to care for them were the most common reasons for a fair or poor rating. Five patients rated their health as very good or good. Their reasons generally included a more positive self-assessment (eg, still being able to perform physical functions, overall sense of being mostly healthy). Examples of patient explanations for their self-rating in their own words are provided in online Appendix B (available at
Food insecurity
Based on the USDA criteria, 30% (95% CI, 17% to 47%) of study patients were food insecure and 25% (95% CI, 13% to 41%) were marginally food secure. On average, those who were food insecure were younger compared to those who were food secure (50.3 yrs. vs. 64.9 yrs. respectively, P = 0.008), though similar on other sociodemographic characteristics (all P > 0.33). Sixteen patients (40%) “worried that their food would run out” and 14 (35%) that their “food would not last,” some of the time or all of the time in the past 30 days. Seven (17.5%) “did not eat for a full day,” and 4 (10%) responded that they were “hungry but did not eat,” in the past 30 days. (Data not shown.)
Quantitative measures alone are insufficient to understand food insecurity. The understanding of food insecurity was expanded and deepened by qualitative data derived from the experiences of individuals. In the following exchange, a 66-year-old white female was asked to expand on her answers to 3 of the food insecurity questions. (Interviewer is indicated with I and Patient with a P.)
I: In the last 30 days, did you ever eat less than you felt you should because there wasn't enough money for food?
P: Yes and no.
I: Can you tell me a little bit about that?
P: At the end of the month I don't have money really. I'm by myself and that is my only income. By the time you buy personal, household…you've got to have coffee, you've got to pay your co-pays for doctors…I go to doctors a lot, transportation, gas.
I: …there's not a lot left over after that?
P: If any …30 days is a long time.
I: It sounds like a tough predicament to be in…
P: [interrupts] when you don't have any other income.
I: In the last 30 days were you ever hungry but you didn't eat because there wasn't enough money for food?
P: No, I'll go to my daughter or whatever.
I: Did you ever not eat for a whole day because there wasn't enough money for food?
P: That's a rough question. Yes.
I: Is that something you can tell me about?
P: Not really. It just wasn't there.
I: How true is this statement for you: I've worried whether my food would run out before I got money to buy more? Often true for you? Sometimes true? [Never True?]
P: Sometimes. …I go the first of the month and buy what I can buy and when it goes, it goes.
Shopping for and preparing food
The inability to shop for and prepare food puts many individuals at risk for not having adequate or appropriate food in the home. This is of increasing importance for individuals who have multiple chronic conditions such as this study group of super-utilizers. Seventy-five percent (95% CI, 59% to 87%) were unable to shop for food without assistance from others. All of those who were unable to shop on their own identified at least 1 other person—a family member, friend, or neighbor—who helped them with shopping. Those who needed help shopping were older (64.6 yrs. vs. 48.3 yrs., P = 0.005) but did not differ by race, sex, education, or by whether they lived alone (all P > 0.21). In the following exchange, a 68-year-old biracial female described the help she got from her cousin.
Interviewer (I): Do you have any trouble doing the food shopping?
Patient (P): Not really. When I go food shopping, my cousin always goes with me because I am in a wheelchair and I can't walk the aisles.
I: Does your cousin unpack the food for you…?
P: Yeah, he gets it off the shelf… He packs it and he brings it home to me.
Sometimes dependency on others involved a loss of control over what food was purchased and, in some cases, their own access to it. One patient lamented that, while family and neighbors brought her food, others in her house ate it first: “And my guests going to come in there and tear ‘em up, eat ‘em up and I don't have nothing to eat.” [61-year-old black female]
Another noted how she was dependent on what her granddaughters purchased for her:
“Well, a lot of times…they [her granddaughters] prepare the meals and when they go shopping, they'll buy something that they like.” [87-year-old black female]
One male who lived alone talked about his difficulties obtaining and preparing food for himself: “… there is nobody around to buy me [food]. And I got to either get in touch with somebody to get it or I got to go get it and that makes it sort of hard…” [82-year-old black male]
Even those who were able to shop for food without assistance reported having problems with food shopping. The main reasons cited were not being physically able to carry enough groceries on public transportation or not having a reliable mode of transportation to get to the store. Some patients mentioned problems with mobility while inside the store or becoming fatigued quickly and needing someone there to help them shop.
More than 57% (95% CI, 41% to 73%) reported needing help preparing meals. One patient, who was wheelchair bound, reported that although she could prepare her own food, she was physically unable to see above the stove level: “I could [prepare food] … but see the stove is like eye level. I can't see in the pot.” [66-year-old black female]
All patients who needed help with food preparation identified someone who prepared food for them or helped them with food preparation. Despite having help, one patient expressed his fear of not being able to prepare or feed himself: “…that's the greatest challenge, and that's what I worry about most. Um, being found where I can't prepare my own food, or I can't—there is nothing, it might be there but I can't—I'm in a condition where I can't fix it or eat it.” [60-year-old biracial male]
Use of community food programs
In addition to government-supported supplemental nutritional assistance programs, food banks, pantries, and church programs were important resources for emergency food for individuals and families. Home-delivered meal programs provided nutritional assistance (and often social support) to those coping with chronic or terminal disease and/or unable to leave their home.
Twenty-four patients (60%) obtained food from community programs at some time. Thirteen (32.5%) had obtained food from food pantries, 17 (42.5%) from food give-away programs at churches, and 6 (15%) patients reported receiving (free) home-delivered meals. Those who had obtained food regularly from food pantries or church programs were knowledgeable about the locations and/or times of distribution. Others who used these resources irregularly were, understandably, less certain about location or times of distribution. Sixty percent of food secure patients and 58% of food insecure patients reported using food pantries, church programs, or home-delivered meals to obtain food at some time (P > 0.9).
Discussion
This study found that 30% of hospital super-utilizers were food insecure and another 25% marginally food secure by the USDA definition. Although comparisons with other studies should be made cautiously, the research team notes that the 2014 national average of household food insecurity reported by the USDA was 15.4%. 8 Reports of food insecurity in other groups of low-income patients have ranged from 18% to 46%. 23 –25
Of equal concern are the findings that the majority of super-utilizers were unable to obtain food on their own and unable to prepare it. Access to nutritionally appropriate and adequate food is an important health concern for low-income populations in general, and particularly so for those with chronic conditions, which are often diet sensitive. 26 –28 In the study group, all of the more commonly reported diagnoses were diet sensitive and have specific nutritional guidelines associated with each condition. This heightens the importance of assessing both food insecurity as well as understanding about dietary needs and restrictions, particularly in patients with high hospital utilization.
Patients reported that family, friends, and neighbors provided critical assistance in bringing food into the home. These “nutritional gatekeepers” 29 often determined what foods would be available in the home and how they were prepared. Dean and Sharkey highlight the critical role family and friends play in ameliorating food insecurity. 30
More than half of the study group had obtained food from food pantries, church programs, or received home-delivered meals. It appeared to the research team that patients were minimally aware of what food resources in their community were available to them. In fact, more than half of the patients interviewed were interested in having a list of food banks or pantries where they could go to obtain [no cost] food.
To the research team's knowledge, food insecurity in super-utilizers has not been reported previously. The team has identified practical problems in food insecurity and food access faced by a sample of mainly African American super-utilizers. The team investigated the prevalence of food insecurity and also used qualitative investigation. This combined approach provided a context and face to the experience of food inadequacy, as so eloquently noted by Chilton. 31 The study results are limited by focusing on a selected group of super-utilizers at 1 institution at 1 point in time. The research team was able to report utilization within the study hospital system although it is possible that patients in the study group were admitted to other hospitals. Although the team took time to establish rapport, they expect that food insecurity in the study group was underreported.
Future investigation in larger studies is needed to better understand barriers to adequate and nutritionally appropriate food in patients with high hospital resource utilization. In the course of the interviews, the research team observed that many patients seemed uninformed about the dietary regimen appropriate for their health conditions. Only a few volunteered examples of how they needed to restrict their food choices or use of salt or sugar. Although this is understandable in the context of poverty, it is an important population health management concern. Institutional engagement in community partnerships, as Nash notes, is a critical component of practicing population health. 32,33 Interventions that educate and connect patients with unmet food needs to community resources such as food banks and home delivery programs can help to engage patients in their own health and well-being. Communication with patients about whether they have enough and appropriate food for their health conditions is an important starting point.
Footnotes
Author Disclosure Statement
Drs. Phipps, Hares, and Braitman, and Ms. Singletary, and Ms. Cooblall declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received the following financial support: This study was funded by Albert Einstein Society (Phipps, PI) grant #8545.
Acknowledgments
We thank Jared Vanderzell, BBA for his assistance in preparing the hospital data for analysis and Kathleen Mahan, RN for her review of the payor data. We also thank Steveanna Wynn and Gail Johnson of the Self-Help and Resource Exchange (SHARE) Food Program for providing us with an on-site orientation to community food programs and for sharing information with us about food assistance programs in Philadelphia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.