
Abstract
This qualitative review of 57 published case reports aimed to analyze primary care and public health integration efforts in 45 states to summarize collaboration aims, participants, and systemic, organizational, and interactional success determinants. Chronic disease management, maternal and child health, and wellness and health promotion were the most commonly reported aims of collaboration between primary care and public health entities in the United States. Typical participants were government public health structures, health delivery systems, communities, academia, state professional medical associations, and employers and businesses. Systemic, organizational, and interactional determinants included adequate funding, multiple stakeholder engagement, leadership, data and information sharing, capitalization on collaborator resources, community engagement, steering committees, effective communication, regular meetings, shared mission, vision, and goals, previous positive relationships, collaborations, and partnerships. The present study contributes to the body of knowledge of when, where, and under what contextual circumstances collaboration and integration have been perceived as effective. Future research could extrapolate which determinants are more essential than others and focus on how systemic, organizational, and interactional factors are interrelated. To advance the practice of successful integration between primary care and public health entities, longitudinal research is needed to examine the degree of integration and sustainability.
Introduction
Few formal analyses of the efficacy of primary care and public health integration efforts exist. 1 A literature review conducted in Canada revealed that integration efforts resulted in improved health-related outcomes, improved access to health services, improved implementation of new collaborative initiatives, improved chronic disease management, and improved communicable disease control. 2 Wright, Ugwi, and Nice 3 described integration as a strategy toward improved health outcomes, reduced costs, and ultimately, reduced health disparities. Additional research is necessary to both heighten awareness of the significance of collaborative efforts between primary care and public health sectors and to reveal the complex array of determinants influencing their success in the United States and worldwide. Such analyses could inform and catalyze efforts to replicate early successes; heighten understanding of when, where, and under what contextual circumstances collaboration is effective; and inform opportunities for future synergies. 4 The purpose of this qualitative, systematic, and sampling review of published case reports of collaboration between primary care and public health entities in the United States was to investigate the following primary research questions:
Research Question 1: What are the most commonly reported aims of collaboration between primary care and public health entities in the United States?
Research Question 2: Who are the most commonly reported participants in primary care and public health integration efforts in the United States?
Research Question 3: What are the most commonly reported systemic, organizational, and interactional determinants of successful integration efforts among primary care and public health entities in the United States?
Research Question 4: Do the most commonly reported determinants of successful integration between primary care and public health entities among cases in the present study align with previous research findings?
Background
Disease in the United States has transitioned from predominately infectious to predominately chronic in etiology. 5 Most of the country's more than $3.0 trillion national health expenditures 6 can be attributed to direct medical treatment of chronic conditions. 5 Concurrently, links between chronic illnesses and social, physical, and economic influences remain apparent. 5
San Martin-Rodriguez et al 4 reinforced the importance of collaboration and interprofessionalism on the efficiency and effectiveness of health services. Although federal health agencies, nonprofit organizations, and funding opportunities emphasize the critical importance of integration among primary care and public health entities, the incongruent academic, professional, and private or public sector focus of the 2 systems hinders positive population health outcomes. 5,7 Concurrently, the philosophical frameworks inherent among respective professions can restrict health professionals' viewpoints 4 of collaboration. Lastly, integration efforts are often further confounded by time and funding constraints 8 and market response to uncontrollable health care costs. 9
The Institute of Medicine (IOM) 1 report Primary Care and Public Health: Exploring Integration to Improve Population Health emphasized the power of integration to effect population health. In response to the IOM's report, the Association of State and Territorial Health Officials (ASTHO) 10 collaborated with the IOM and the United Health Foundation to develop a strategic map. The strategic map aimed to assist with the following: strengthening and supporting public health and primary care integration, increasing integration of public health–primary care infrastructure, and identifying partnerships between the sectors to reduce health care costs and improve health care quality and outcomes. To accomplish such goals, ASTHO, a national nonprofit organization representing public health agencies in the United States, launched the Integration Forum (IF), a partnership of more than 60 organizations and 200 individual partners, to promote integration efforts. 10 The present study aimed to review IF case studies, as well as cases from other sources, to identify determinants of successful collaboration among primary care and public health entities and to summarize integration aims and participants.
Drawing on the conceptualizations of San Martin-Rodriguez et al, 4 collaboration determinants were categorized by the following 3 definitions: systemic determinants, defined as “elements outside the organization, such as components of social, cultural, educational and professional systems.”4 (p. 134) Organizational determinants “combine attributes of the organization that define the work environment of the team, such as communication and coordination mechanisms”4 (p. 138) and interactional determinants are “components of interpersonal relationships among team members, such as their willingness to collaborate and the existence of mutual trust, respect and communication.”4(p. 141) In addition, the integration framework presented by Martin-Misener et al 2 served as the conceptual model that guided identification and categorization of the most common determinants of collaboration, as presented in the IF and other case studies.
Methods
Research design
The research design for this study was a sampling and systematic retrospective review of published case reports of collaboration between primary care and public health entities in the United States. The study employed thematic analysis 11 to identify and summarize commonly reported aims of collaboration, participants in collaboration, and determinants of successful collaboration.
Data collection
Cases reported to the ASTHO IF were used as a primary source (most of which were reported in 2013). To identify cases reported on since 2013, 4 databases (PubMed, MEDLINE, CINAHL, and ABI/INFORM) were searched for dates from January 2014 to January 2017 employing the general search strategy displayed in Table 1. Additional peer-reviewed literature was gained using the related articles function. The Practical Playbook 5,12 also was consulted for updated cases. The overall intent of the present study was to contribute to the body of knowledge of when, where, and under what circumstances integration was perceived effective, to inform future endeavors.
Keywords for Electronic Database Search
Cases were included in the study if they identified a primary focus, participants explicitly identified as primary care and public health workers, and at least 2 units of meaning (one unit of meaning had to address a dynamic other than required funding). The ASTHO IF displays 84 cases of primary care and public health integration efforts in the United States. The authors decided to include at least 1 case from each state to ensure widespread geographic representation. The first case reported to the IF in each state, beginning on the west coast and moving eastward, was used for the present study if the aforementioned focus, participants, and units of meaning were apparent. If these 3 criteria were not extracted from the first case in each state, the second case in the state, if available, was used. Florida's Healthy Start Program 13 was the only second case used in place of the first.
No case reports were available for South Dakota, Wisconsin, Michigan, West Virginia, and Oregon. Alaska's Foodborne Botulism case 13 did not meet inclusion criteria. Therefore, the total number of cases included from the ASTHO IF was 44. Integration efforts displayed in the ASTHO IF began prior to 2013 and convey information related to the present study primarily under 4 headings: required resources, key elements for success, lessons learned, or infrastructure to support collaboration and sustainability.
The Practical Playbook and associated website feature 13 public health success stories reported on in 2016 and 2017. In such cases, units of meaning were depicted primarily as lessons learned. Cases were included in the present study if they exhibited the case inclusion criteria previously described and did not duplicate a collaboration aim already addressed by the ASTHO IF map in the same state. This resulted in the inclusion of 7 additional cases.
The search strategy for peer-reviewed journal articles on primary care and public health integration was intended to capture cases reported on in the United States since the ASTHO IF map. A total of 1354 abstracts were reviewed and 6 cases were ultimately included, including a case from Michigan. Peer-reviewed case articles followed no specific reporting format for unit of meaning extraction; rather, units of meaning were discussed broadly, often in results and conclusions sections.
Data analysis
The unit of analysis for this study was units of meaning within each case study brief retrieved from the ASTHO IF map, journal articles, and Practical Playbook. Units of meaning were defined as statements specifically addressing the aim of integration, collaboration participants and determinants, elements, factors, or resources identified (by case authors) as integral to collaboration success, or sustainability as related to Research Questions 1, 2, and 3. Statements presented in cases as lessons learned also were included.
The 14 primary activities of focus of primary care and public health entities conceptualized by the American Academy of Family Physicians (AAFP) 14 was used to guide categorization of collaboration emphases found in articles and reported to the IF and Practical Playbook. To address Research Question 1, simple binary variables (1, 0) were assigned to indicate the presence or absence of each of the 14 activities in each case. Collaboration focus frequencies were calculated and reported for all 57 cases included in the study (see Table 2). To keep analysis concise, a single primary focus was identified for each case. For example, the Ohio case identified an aim of increasing hypertension and cholesterol screening among African American males in a particular age range. 13 Although the targeted population in this case could subject it to multiple categories, only the first category (preventive care screenings) was considered.
Collaboration Aims
Other indicates cases coded outside the original categories in the conceptual model.
Concerning Research Question 2, collaboration participant frequencies were calculated and reported for all 57 cases included in the study (Table 3). The IOM's 1 depiction of the intersectoral public health system (communities, health delivery systems, employers and businesses, media, academia, and government public health structure) informed the categorization of collaboration participants. Simple binary variables (1, 0) were employed to indicate the presence or absence of each of the 6 variables in each case. Subsequently, each case could be defined by inclusion of none of the model participants, all 6 of the model participants, or any number in between.
Collaboration Participants
Indicates cases coded outside the original categories in the conceptual model.
To answer Research Question 3, common determinants of successful integration were analyzed using each of the 13 updated cases included (from the Practical Playbook and journal articles) and the first case reported to the IF in each state, beginning on the west coast and moving eastward until at least 1 case from every state was included. As discussed previously, the final list did not include South Dakota, Wisconsin, Michigan, West Virginia, Oregon, and Alaska. Twenty additional ASTHO cases were coded and evaluated using a second and then third case from each state, where available, to ensure saturation of data among the 57 sample cases. No additional themes emerged from these supplementary 20 cases; therefore, they were not included in the results.
Statements extracted from case studies were identified as units of meaning and inserted into a data extraction form for ease of review and coding. The authors made every attempt to extract success determinants explicit to the integration process rather than the specific integration aim, as integration aim was not a constant variable. The Alabama colorectal cancer screening case served as a clear example of the distinction between integration process and aim. To achieve increased screening rates, the author stressed the importance of mass screening initiatives that improve existing corporate wellness systems. 13 As a disease outcome-specific element, this dynamic was not extracted as a unit of meaning related to integration process among partners.
A codebook (see Supplementary Data), based on the conceptualizations of Martin-Misener et al 2 and refined by researcher interpretation of the data, was developed. Individual units of meaning were coded in 3 distinct phases beginning with the systemic, interactional, or organizational designation. The second phase of coding included categorization of units of meaning into subgroups that comprise the first phase systemic, organizational, and interactional categories. The third and final phase of coding categorized the units of meaning into the various categories that exemplify codes of the second phase. If units of meaning were not detailed enough to be described via 3 phases of coding, coding concluded at the appropriate level. Units of meaning that did not fit explicit codebook definitions were noted, reported, and used to enhance final codebook definitions and to inform study findings and discussion.
Concerning success determinants, one author and a second coder independently reviewed and coded a small number of case studies and collaborated to establish consensus, coder reliability, and codebook exclusivity and exhaustivity. The author trained the second coder in codebook development and function. Interrater coder reliability was recorded and reported. The author continued to code case study reports until no new information was added to the existing research. 15 Code frequencies were calculated, reported, and discussed (Table 4). The researcher synthesized phase 1 coding frequencies to inform and summarize the most commonly reported determinants of successful collaboration, as described by the systemic, organizational, interactional model. Phase 2 and 3 code frequencies were synthesized to provide a more in-depth depiction of the specific determinants inherent among these 3 primary categories. Research Question 4 compared results of the present study's identified success determinants with similar research inquiries, empirical studies, and literature reviews.
Frequencies of Success Determinants
Results
In relation to Research Question 1, collaboration focus, frequency calculations for the 57 cases included in the present study are displayed in Table 2. Chronic disease management emerged as the most commonly reported focus, as identified in 14 of the 57 cases. Explicit conditions addressed included asthma, cardiovascular diseases, HIV, and diabetes (Table 2). 5,12,13,16 The final collaboration addressed multiple chronic diseases. 13
Maternal and child health issues emerged as the primary focus in 10 of the 57 cases. Recurring efforts in this category included reducing infant mortality and improving birthing outcomes (Table 2). 13 Wellness and health promotion emerged as the third most common collaboration focus. Recurring efforts included programs addressing healthy weight or obesity, prescription drug overdose (2 cases), and tobacco cessation. 5,12,13,17 The 6 cases classified as care coordination exhibited no explicit themes. They included aims such as establishment of an integrated health location, 13 creation of neighborhood health stations, 12 and focus on organized trauma care. 13
Five cases in the present study were categorized outside the 14 primary activities proposed by the AAFP. Such aims included increasing or improving access to care for specific populations, an environmental lead exposure issue, and creation of an immunization portal to improve access to valid records (Table 2). 12,13,18 Categories exhibiting less than 5 coded cases included preventive care screenings, immunizations, behavioral health care, community involvement, and outbreak and disaster preparedness (Table 2). 13,19
Table 3 displays results for Research Question 2. Government public health structure emerged as the most frequently reported collaboration partner, as coded in 53 of the 57 sample cases. Specifically, state health department, Department of Health, or Department of Health and Human Services involvement was apparent in 67% of cases, while local health departments were coded as collaborators in 35% of cases. 5,12,13,19 State and local health departments were coded concurrently in 11 cases. Nine cases reported State Medicaid involvement.
Health delivery systems emerged as the second most frequently reported collaboration participant (Table 3). 5,12,13,16 –18,20 Within such delivery systems, the following participants were reported (each delivery system could include more than 1 of the following participant categories): practices or providers, hospitals and health systems, nurses (often in addition to practices and health systems), Federally Qualified Health Centers, community health centers, and rural health clinics (Table 3). Communities comprised the third most frequently coded category of participants. 5,12,13,16,17 More precisely, these collaborations incorporated community organizations or coalitions, including faith-based organizations and local Young Men's Christian Associations. 13
The academia category included universities and local schools or school districts (Table 3). 5,12,13,16,20 University and local school involvement emerged concurrently in 4 cases. 13 No specific themes arose from the employers and businesses category, as not all cases explicitly named the employers and businesses involved. Specific employers noted in single cases included Walmart, Microsoft, Regions Bank, and a local power company. 13
Lastly, although not specifically mentioned in the IOM's depiction, state professional associations were coded in 13 cases. 5,12,13,20 Chapters of the American Academy of Pediatrics led the list. Other professional chapters included the American Lung Association, the American Heart Association, the AAFP, and the American College of Obstetricians and Gynecologists. 13
Every extracted unit of meaning related to success determinants was coded at least to the first level: systemic, organizational, or interactional. Initial reliability between 2 independent coders for all coding levels was 84%. After reconciling coding discrepancies through discussion, the 2 coders reached complete consensus. Intercoder reliability and intercoder agreement in the present study were differentiated by the following definitions: Intercoder reliability “requires that two or more equally capable coders operating in isolation from each other select the same code for the same unit of text.”21(p. 297) Intercoder agreement
“requires that two or more coders are able to reconcile through discussion whatever coding discrepancies they may have for the same unit of text – discrepancies that may arise, for instance, if some coders are more knowledgeable than others about the interview subject matter.”21(p. 297)
Results for Research Question 3 are listed in Table 4. Adequate funding was coded in 54 of the 57 included cases, most commonly reported as a required resource. 5,12,13,16,17,20 In 2 of the extraneous cases, the funding source was unclear to the authors. The Living Well Hawaii Project, aimed at improving health outcomes for adults with serious mental illness, explicitly highlighted the lack of additional funding required to initiate the project. 13
Federal funding or grants were identifiable in 35 cases, with the CDC being the most common source (14 cases). The breakdown of cases showing State funding or grants, concurrent Federal and state funding or grants, and Miscellaneous are shown in Table 4. Miscellaneous funding sources included foundation (5 cases) and private (4 cases). Advocacy was the only noted recurring systemic determinant coded in fewer than 5 cases. 13
Multiple stakeholder engagement arose as the most commonly coded organizational determinant, 5,12,13 followed by leadership (Table 4). 5,12,13,16 Specific statements about leadership were broad and, therefore coding concluded at the second level. Units of meaning coded in this category included a strong leadership team, ongoing leadership, strong network leadership, high-level engagement from leadership, and identification of a single lead organization. 5,12,13
Data and information sharing units of meaning appeared in 10 cases. 5,12,13 This was followed by capitalizing on various collaborator resources, community engagement, and the positive role of steering committees (Table 4). 5,12,13 Steering committee involvement represented an explicit subcategory of leadership that could be coded to a third level and therefore was reported separately. 13,17 Recurring organizational determinants coded in fewer than 5 cases included joint planning and collaboration evaluation mechanisms. 13
Emerging interactional themes included effective communication; regular meetings between members; shared mission, vision, or goals among collaborators; and previous positive relationships among collaborators (Table 4). 5,12,13,17 –19 Collaboration and partnerships were presented nonspecifically as facilitators of success or lessons learned. 5,12,13 Recurring interactional determinants coded in fewer than 5 cases included quality professional relationships and cultural competency among collaborators. 13
In relation to Research Question 4, integration success determinant results depicted in the present study reinforced components of multiple historical conceptual models. Examples included the importance of shared goals, as described by Lasker 9 and Scutchfield et al, 22 and the synergistic effects of diverse resources and skills. 9 The importance of diversified funding, 22,23 leadership, 23 and aligned data collection 24 also were supported. Perhaps most importantly, the results in the current study explicitly reinforced 4 of the 5 principles of integration set forth by the IOM 1 : shared goals, community engagement, leadership, and collaborative use of data and analysis. The fifth principle, sustainability, 1 did not emerge as a theme in the present study.
The systemic, organizational, interactional framework conceptualized by San Martin-Rodriguez et al 4 and Martin-Misener et al 2 proved inclusive, as every extracted unit of meaning in the present study was coded to at least the systemic, organizational, or interactional level. Adequate funding was the sole systemic determinant coded to 3 levels in multiple cases. The authors' decision to focus on self-reported success determinants may have led to underrepresentation of systemic determinants in the present study; this will be discussed further in Conclusions.
Organizational determinants defined by 3 levels of detail included multiple stakeholder engagement, various collaborators bringing resources to the table, steering committees, and community engagement. Interactional determinants defined by 3 levels of detail included shared mission, vision, and goals; previous positive relationships among collaborators; regular meetings among collaborators; and general mention of partnerships and collaborations.
The results of Research Question 3 also underscored explicit literature-derived determinants not exemplified among cases included in the current study. For example, no extracted units of meaning typified the following second-level systemic categories: government involvement, policy and fit with local needs, power and control issues, and education and training. Likewise, geographic proximity of partners remained a second-level organizational category with no emerging themes.
Discussion
The present study's summary of primary care and public health integration efforts aligned fundamentally with previous frameworks, including Lasker, 9 the IF, 10 and Martin-Misener and Valaitis. 25 Lasker's 9 conceptualizations of the importance of coordination of services and community involvement were reinforced, as were ASTHO's 10 broad categories of leveraged initiatives and expanded collaborations. Also highlighted were Martin-Misener and Valaitis's 25 focus areas of chronic disease, immunizations, access, and smoking cessation. The AAFP's conceptualization of 14 primary activities proved inclusive and useful for this study. All but 5 cases were coded within this model.
The authors' decision to identify a single integration aim for each case in the present study likely contributed to the lack of thematic representation of the following categories: advocacy, patient registries, transitions of care, palliative care, and social determinants identification. For example, the Idaho Maternal and Child Health Program was coded in the maternal and child health category in the present study, but the case highlighted a concurrent effort to address health disparities. 13 The Kansas case aimed at improving infant mortality also was categorized in the maternal and child health category, despite its concurrent focus on low-income women. 13 These results suggested secondary aims could be evaluated in future work to further inform concurrent collaboration aims.
Chronic disease management, maternal and child health, wellness and health promotion, care coordination, preventive care screenings, immunizations, behavioral health care, community involvement, and outbreak and disaster preparedness, as consistent with the AAFP's 14 primary activities conceptualization, were confirmed as collaboration themes in the present study. These themes, as well as those that were absent as primary aims in the current study, provide a solid reference for informing current collaboration efforts and highlighting where opportunities may exist for future endeavors.
The present study's summary of primary care and public health collaboration participants also aligned fundamentally with previous models, including the IOM's 1 depiction of the intersectoral public health system. Media involvement represented the most obvious variance between the present study's findings and the IOM's 1 intersectoral conceptualization, as it did not emerge as a commonality in the present study. Other participants explicitly mentioned in previous literature that did not arise as commonalities in the present study included nutritionists, therapists, pharmacists, housing organizations, and health advocacy lawyers. 1,5,9 Conversely, the present study revealed professional health care associations as a common collaboration participant. Future collaborative efforts could benefit from knowledge of potential participants who have been historically underutilized, as well as summaries of those incorporated most frequently.
Research Question 3 in the present study addressed success determinants. At the systemic level, results revealed adequate funding as an essential component of collaboration initiatives. Organizationally, multiple stakeholder engagement, leadership, data and information sharing, pooling resources, community engagement, and steering committees emerged as common themes. At the interactional level, effective communication; regular meetings; shared mission, vision, and goals; previous positive relationships; and collaborations and partnerships were typified. These results largely reinforced previous conceptualizations, such as Lasker's 9 focus on shared goals and diverse resources and skills. Collaboration and vision, mission, and goals, as presented by Jones and Leighton 26 and Scutchfield et al 22 also were exemplified. Lastly, the systemic, organizational, interactional framework conceptualized by San Martin-Rodriguez et al 4 and Martin-Misener et al 2 proved inclusive, as every extracted unit of meaning in the present study was coded to at least 1 level (systemic, organizational, or interactional).
The authors' decision to focus on self-reported success determinants may have led to underrepresentation of systemic determinants in the present study. The IF itself represents a collaboration of diverse federal, state, and local health agencies seeking to inform, align, and support integration efforts. 10 As such, codebook elements, such as government involvement, common goals (at the systemic level), and collaboration between levels of government, were apparent. Because these elements were not explicitly identified by case authors as determinants, elements, factors, or resources as integral to collaboration success or sustainability, they were not extracted as units of meaning for inclusion in the present study. Similarly, the IOM 1 suggested that Million Hearts initiatives inherently portray a shared goal of population health improvement. Nevertheless, the shared goal of population health improvement was not extracted as a unit of meaning in the current study's Million Hearts cases because it was not explicitly apparent. Examples included cases from Iowa, Ohio, New York, and Maryland. 13
The results of the present study also underscored explicit literature-derived determinants not exemplified among cases included in the current study. For example, no units of meaning were coded in the second-level systemic categories of government involvement, policy and fit with local needs, power and control issues, and education and training. According to Martin-Misener et al, 2 historic examples of such systemic determinants included health reform and government mandates for development of teams and partnerships. Other examples included enhancing evidence-informed practice and improving emergency planning and response. 2 Interdisciplinary education and educational programs promoting integrative practice and diverse team facilitation also were important. 2
Geographic proximity of partners remained a second-level organizational category with no emerging themes. Martin-Misener et al 2 described co-location of primary care and public health organizations and team members as a collaboration facilitator. Geographic proximity of team members facilitated communication, information exchange, a sense of common purpose, and high levels of trust among collaborators. 2 Much like collaboration aims and participants, future integrative efforts could benefit from knowledge of the presence or absence of such factors within previous efforts.
The final purpose of the present study was to compare the most commonly reported systemic, organizational, and interactional determinants of successful integration between primary care and public health entities in the present study with previous research findings. As discussed previously, determinants reported in the present study partially aligned with multiple historical conceptual models. Further, the codebook used in the present study proved useful for categorizing units of meaning as systemic, organizational, or interactional. Additional case study detail could facilitate more precise second- and third-level coding.
Limitations
Explicit limitations characterized the current study, thus limiting the generalizability of its findings. 11 It is important to note the ASTHO integration cases examined in this study were self-reported and, therefore, could carry a bias toward those strategies that proved successful, represent organizations that qualify as members of ASTHO, or represent organizations with the leadership interest, resources, transparency, and capacity to generate such reports. This study did not attempt to identify cases exhibiting higher degrees of integration or demonstrating prolonged sustainability, nor did it attempt to distinguish large-scale from small-scale integrations or urban from rural integrations. In addition, cases displayed in the ASTHO IF map followed at least 2 distinct reporting formats and exhibited varying degrees of detail; both of these dynamics complicated the data extraction process. Lastly, extracted units of meaning were derived from one author's interpretation of the case reports and therefore were subject to misinterpretation.
The authors' decision to identify a single integration aim for each case in the present study likely contributed to the lack of thematic representation of the following categories: advocacy, patient registries, transitions of care, palliative care, and social determinants identification. For example, the Idaho Maternal and Child Health Program was coded in the maternal and child health category in the present study, but the case highlighted a concurrent effort to address health disparities. 13 Secondary aims could be evaluated in future work to further inform primary and secondary collaboration aims.
More broadly, although qualitative research analyses are valued for their richness and potential to inform new relationships, 11 the present study did not provide an understanding of how the systemic, organizational, and interactional determinants influence collaborative or integrative practice among sectors. A lack of empirical evidence addressing this pattern persists. 4 In addition, and consistent with previous literature, 1,2,27,28 semantic discrepancies exist between the term integration and similar terms such as collaboration, cooperation, and coordination. Lastly, the present study did not identify optimal degree of integration because it can vary with integration dynamics such as differentiation of services. 29
Conclusion
Future research could further extrapolate which determinants are more essential than other determinants and focus on how systemic, organizational, and interactional factors are interrelated. Repositories such as the ASTHO's IF may prove critical to future research, as they provide comparative information in a relatively standardized reporting format. Additional primary research and theoretical constructs are necessary to advance the science and practice of successful integration between primary care and public health entities in the United States as well as to analyze whether integration was actually achieved (and to what degree).
Future case authors should deliberately consider reporting format. If case authors make success determinants explicitly apparent to readers under such headings as Key Elements for Success, 13 unit of meaning extraction becomes clearer and more meaningful. To ensure unit of meaning detail consistent with codebook detail, case authors should consider reporting as much detail as possible about explicit perceived success determinants. For example, it was difficult to distinguish between common goals at the systemic and interactional levels in the present study without sufficient background information. The authors would like to propose the Washington Prescription Drug Overdose case, which plainly highlighted collaboration aim and participants, as an optimal reporting model of relaying information relevant to integration success. Further, success determinants related to integration process (common understanding of the problem among parties and all parties work cohesively) were clearly distinguishable from successes related to collaboration aim (reduction in the number of opioid poisonings and fatalities in the last 2 years). The 2 categories were separated and designated key elements of success and results, respectively. 13
In the present study, the authors concluded use of the IOM's 1 definition of primary care and public health integration depicted cases in the present study: “The linkage of programs and activities to promote overall efficiency and effectiveness and achieve gains in population health” (p. 3). In its report, Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes, the IOM 30 utilized the following definition of collaboration: “an active and ongoing partnership, often involving people from diverse backgrounds who work together to solve problems, provide services, and enhance outcomes” (p. xi). This definition also accurately described cases in the current study, although use of the word partnership can be further confounding. If one accepts the IOM's 1 conceptualization of collaboration as a degree along the integration continuum, a collaboration–integration dual categorization of cases in the present study would be logical. A majority of the cases in the present study demonstrated the ability to enhance outcomes and achieve gains in population health. Some ASTHO IF case authors identified explicit integration degree. Although ASTHO cases were included in the present study irrespective of integration degree, consideration of perceived degree was useful when attempting to summarize integrative efforts. Figure 1 displays a summary of integration degree reported in 15 ASTHO cases. 13
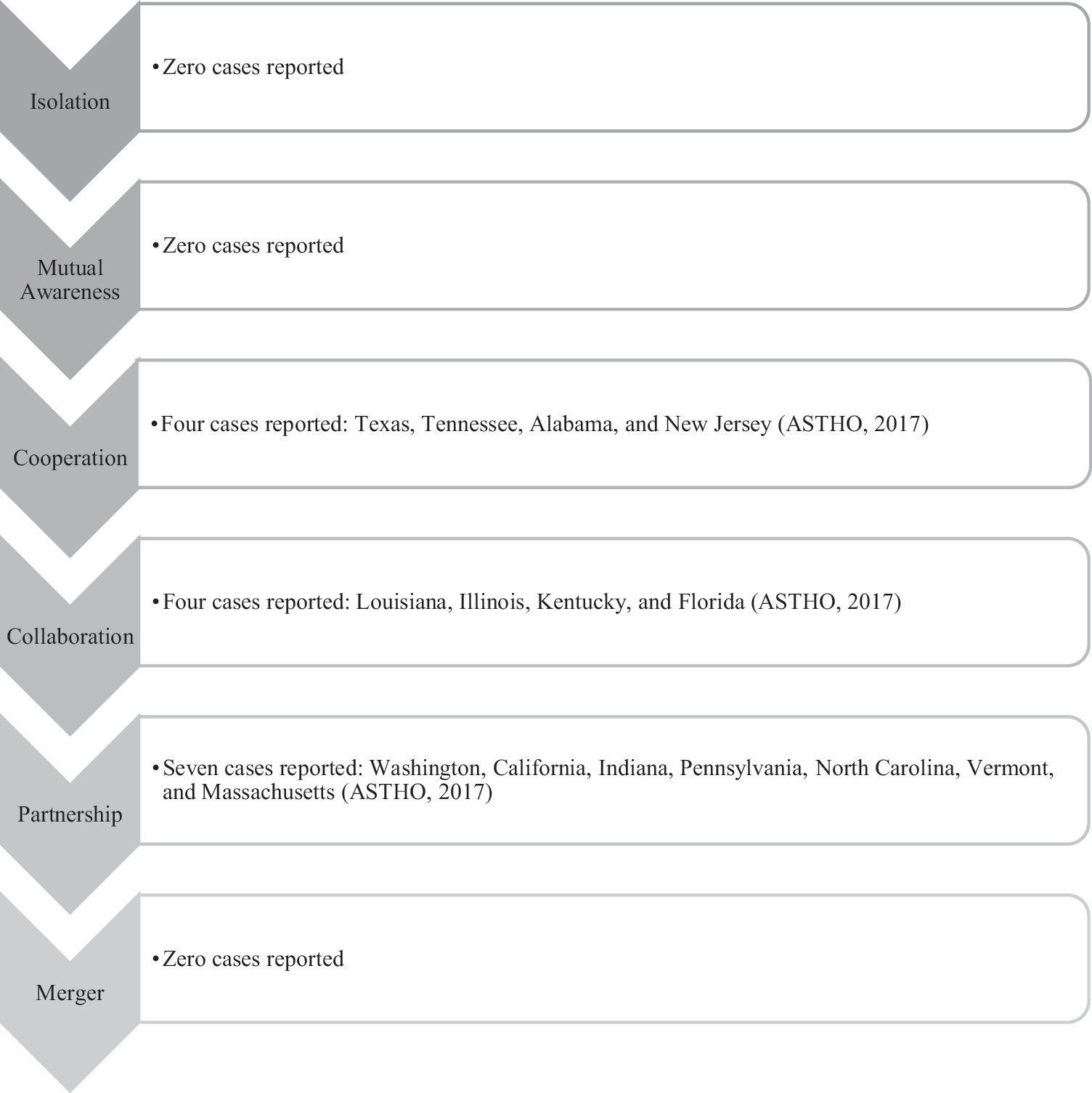
Integration degree. Adapted from: Institute of Medicine. 1
The IOM 1 posits federal policy and funding are the greatest levers influencing primary care and public health integration. Concurrently, they recognize grant funding as a potential limiting factor of integration sustainability. 1 Additional research is necessary to enhance understanding of the impact of systemic, organizational, and interactional determinants on project sustainability relative to monetary factors. Although most of the cases in the present study lack detail about sustainability, review of cases such as The Living Well Hawaii Project 1 may prove worthwhile. This case highlighted an effort that recognized a certain level of success despite the absence of funding.
Self-reported case summaries such as those in the present study (Table 5), are characterized by inherent confounds. Self-reported cases can provide essential information for research examining success determinants but also can be deemed a weak evaluative strategy. 31 Self-reports can be biased by the general impression of professionals' perceptions of the phenomena of integration. 29 Perceptions also can vary between individual stakeholders and groups of stakeholders involved in collaborative efforts. 29 To eliminate such biases and to facilitate comparative data, the authors suggest independent or quantitative assessment of future integrative efforts may prove beneficial. Independent assessors should practice diligence in developing evaluation language that is relevant to all stakeholders. Raney, Lasky, and Scott 28 posit evaluation models may need to highlight process and outcome measures such as patient and provider satisfaction, improved population health, value-based savings, and sustainability. Further development of carefully articulated interprofessional collaboration milestones also may be warranted. 32
Cases Included in the Present Study
ASTHO, Association of State and Territorial Health Officials.
Based on the evidence in the present study, funders of future collaborative efforts could demand emphasis on the following elements: social determinants as clear primary aims, sustainability as a foundational guiding principle, 1 and funding dedicated to supplemental external evaluations. In addition, research relating integration degree and level of results achieved could prove useful. Specific levels of integration may be more or less appropriate depending on integration aim. Lastly, perhaps future collaborators should solicit interest from underutilized groups highlighted in the present study (the media, therapists, housing organizations, and health advocacy lawyers) as well as investigate the systemic determinants that portrayed little representation (policy and fit with local needs, power and control issues, and education and training).
The ASTHO strategic map aimed to strengthen and support public health and primary care integration. The authors contend this goal is progressed through the data summarized in the present study. This review portrays the vast array of health professionals, models of care, social, and interpersonal contexts that influence collaborations. Primary care and public health entities have critical, complimentary roles. The present study contributed to the body of knowledge intended to inform and catalyze efforts to replicate early successes; heighten understanding of when, where, and under what contextual circumstances collaboration is effective; and inform opportunities for future synergies.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest. The authors received no financial support for this article.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.