
Abstract
People with disabilities can face substantial barriers to living stably in community settings. Evidence shows that permanent supportive housing (PSH), which combines subsidized housing with individualized support services, can improve housing stability among subpopulations of people with disabilities, including those with behavioral health conditions. PSH has also been shown to improve some health outcomes among people with severe mental illness or substance use disorder, but effects varied by participants' program tenure. This study assessed retention in a PSH program serving a broad population of adults with disabilities and identified factors associated with program tenure. Administrative data from 2093 individuals who began participating in a North Carolina PSH program between 2015 and 2018 were analyzed. Participants' unadjusted probability of remaining in a PSH placement at specific time points was estimated, with censoring due to death or the end of the study period (July 2020). Using Cox regression, program tenure was modeled as a function of participant and PSH placement location characteristics. Participants had a 71% probability of remaining in PSH after 2 years. Older age, female gender, and non-Hispanic Black race/ethnicity were associated with lower hazard of PSH departure. Having a severe mental illness diagnosis was associated with greater departure hazard. Level of socioeconomic deprivation and rurality of the PSH placement ZIP code were not associated with departure hazard. PSH programs may be able to successfully retain a heterogeneous population of adults with disabilities, although tenure may vary by participant demographic and clinical characteristics.
Background
Housing stability is a well-established determinant of health outcomes. 1 People with physical or mental disabilities can face substantial barriers to maintaining stable housing, representing nearly one-quarter (24%) of adults in the United States experiencing homelessness. 2 When housed, those with disabilities may reside in restrictive settings, such as nursing homes and adult living facilities, in part because the services they need are not available in the community. 3 Compounding the challenge of poor community-based service availability, the dire lack of affordable rental housing across the United States 4 places a particular burden upon people with disabilities, who often have limited income.
As of 2019, 25.9% of nonelderly noninstitutionalized adults with disabilities had an income level below the United States Census Bureau poverty threshold, compared with 11.4% of those without disabilities. 5 For people with disabilities who rely upon public benefits such as Supplemental Security Income (SSI), rental costs may exceed their ability to pay; as of 2016, the national average rent for a studio apartment was equivalent to 99% of the average SSI payment. 6
Permanent supportive housing (PSH) programs combine subsidized housing with individualized community-based support services 7 to help individuals with disabilities maintain stable affordable housing in the community. PSH programs have been shown to improve housing stability among people with serious mental illnesses, substance use disorders, or HIV who are unhoused or at risk of becoming unhoused. 8 PSH may also have downstream health benefits, 9 and it has been found to reduce acute health care use among some subpopulations, including unhoused individuals with behavioral health conditions. 10
A key feature of the PSH model is provision of housing on a long-term basis. 10 Studies of chronically unhoused individuals with behavioral health conditions have found that over half of participants remained housed 2 years after entering PSH. 11 –14 Among participants with behavioral health conditions, program tenure varies by participant age, substance use pattern, housing unit features, and neighborhood social distress, 12,13,15 and tenure is associated with improvements in some health-related outcomes. 16,17
Less is known about program tenure among individuals with disabilities other than behavioral health conditions 8 and individuals who move into PSH from institutional settings. 18 Understanding the experiences of formerly institutionalized populations is especially important as a number of states are implementing supportive housing programs to transition people with disabilities from institutional to community settings. 19
This study assesses retention in a scattered-site PSH program serving North Carolina residents who have a disability and a low income level. Using PSH program administrative data merged to Medicaid claims data, the authors estimate the association between PSH program tenure and participant characteristics and PSH placement area characteristics. By evaluating a PSH program that serves people with a wide range of disability types who enter the program from a variety of settings, this study builds upon similar evaluations of PSH programs that served only chronically unhoused individuals with severe mental illness or substance use disorder.
Methods
PSH program description
The PSH program under study is administered by the North Carolina Department of Health and Human Services and the North Carolina Housing Finance Agency. As part of the program, 10%–20% of units in North Carolina rental properties financed by the Low-Income Housing Tax Credit, a tax credit for property developers intended to incentivize the creation of housing for low-income households, are set aside for individuals with disabilities and their families. 20
These rental units are made affordable to low-income individuals with disabilities through rental subsidies of an amount that ensures they spend no more than 30% of their household income on rent and utilities. 21 Participants are also entitled to receive flexible individualized services intended to enhance their ability to maintain tenancy, such as rehabilitation counseling, peer support services, or case management services.
To be eligible for the program, an individual must be at least 18 years old, have a disability (identified through receipt of federal disability income), and have an income level that is <50% of the area median income but a minimum gross monthly income of at least $300. Participants can enter the program after being chronically unhoused or after living in an institution or living in the community, and the population served by the program includes individuals with severe mental illness, substance use disorder, physical disabilities, intellectual/developmental disabilities, and/or other severe chronic health conditions.
Data
Primary data sources for this study included administrative data on individuals who participated in the PSH program between 2014 and 2018 and 2014–2018 North Carolina Medicaid enrollment, professional claims, and institutional claims data obtained through the Carolina Cost and Quality Initiative. 22 The PSH program data contained PSH participants' housing placement move-in dates and move-out dates for any program departures that occurred before July 3, 2020. These data also contained limited information about participants' reasons for housing placement exit, as reported by property managers.
The Medicaid data contained information on PSH program participants' demographic characteristics, area of residence at the ZIP code level, type of living arrangement, and clinical diagnosis codes. The North Carolina Division of Health Benefits, the state's Medicaid agency, merged the PSH program data and Medicaid claims data using individual first and last name, date of birth, and ZIP code. They obtained a match rate of 74%; many PSH participants were not enrolled in Medicaid and thus would not be expected to match to a Medicaid identifier.
This study was determined to be exempt from review by the Institutional Review Board at the University of North Carolina at Chapel Hill.
Sample
The sample was restricted to PSH program participants who were enrolled in Medicaid sometime during the 2014–2018 time period for which Medicaid data were available (n = 3337). The sample was further restricted to individuals who began participating in the PSH program from 2015 to 2018 (n = 2342) so that a 12-month wash-out period with no prior participation in the PSH program could be implemented. Continuous enrollment in full Medicaid coverage in the 3 months before the PSH move-in date (n = 2093) was also required so that information about participants' ZIP code of residence, living arrangement, and diagnosis codes before program participation could be observed in the Medicaid claims.
Measures
The dependent variable in the study was a continuous measure of the number of days in the PSH program until censoring due to death (identified using the death date as reported in Medicaid claims data) or the end of the study period, where the last date observable in the PSH program data was July 3, 2020. The explanatory variables included participant demographic and clinical characteristics, as well as characteristics of the ZIP code where their PSH placement was located. A continuous measure of age and categorical measures of gender (male or female) and race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, and other/multiple races reported) were constructed using demographic information reported by participants in the Medicaid enrollment data.
Although information about the disabling condition(s) that qualified an individual for participation in the PSH program was not available, indicators of potentially disabling chronic condition types were constructed and classified using the program's qualifying disability categories (severe mental illness, substance use disorder, physical conditions, intellectual/developmental disorders (IDDs), and other severe chronic conditions). Relevant ICD-9 or ICD-10 diagnosis codes using chronic condition definitions were identified based on the Healthcare Cost and Utilization Project (HCUP) Clinical Classifications Software (CCS) for ICD-9 and ICD-10, 23,24 and an individual was classified as having a given condition if they had 2 claims on distinct dates with diagnosis codes for the condition (see Appendix Table A1 for additional information).
To capture potential differences in PSH experiences by living arrangement before program participation, the analysis included an indicator of whether an individual was institutionalized for at least half of any month in the 3 months before entering PSH. Institutionalization was defined using a combination of living arrangement codes in the Medicaid enrollment file; room and board revenue codes in the institutional claims for nursing facility stays, intermediate care facility stays, or inpatient stays; and professional claims charges for personal care services delivered in an adult living facility. The analysis also included an indicator of whether an individual was ever dually enrolled in Medicare in the 3 months before entering PSH to adjust for potential differences in baseline health service access resulting from the additional source of health insurance coverage.
As a measure of service availability in the community, indicators of the rurality of the PSH placement were generated using the 2010 Rural-Urban Commuting Area (RUCA) code associated with the placement ZIP code, with metropolitan, micropolitan, small town, and isolated area categories. 25 As an additional measure of community resources, the level of socioeconomic deprivation of the PSH placement ZIP code was classified using the 2015 Social Deprivation Index (SDI). The SDI is a composite measure constructed using multiple area socioeconomic variables from the American Community Survey. 26 Since the SDI measure is only available at the ZIP Code Tabulation Area (ZCTA) level, the 2017 UDS Mapper ZIP Code to ZCTA Crosswalk was used to identify the ZIP code associated with each ZCTA.
Using the continuous SDI measure, a set of indicators were developed based on the percentile of the ZIP code SDI score relative to all North Carolina ZIP codes with a valid SDI score (<25th percentile, 25th to <50th percentile, 50th to <75th percentile, 75th percentile or above). Greater percentile values indicate greater social deprivation. In addition to measures pertaining to the PSH placement, measures of the rurality and SDI percentile of the ZIP code of the pre-PSH residence were also included, to control for baseline service and resource access.
Area-level characteristics were examined based on both PSH placement ZIP codes and pre-PSH residence ZIP codes, using Medicaid enrollment data. To account for potential delays in updates to address information in the enrollment data, the ZIP code from the second month after the PSH move-in date was used if available or if not available, any nonmissing ZIP code from the 3 months after the move-in date or the move-in month itself was used. For the pre-PSH residence ZIP code, the modal ZIP code from the 3 months before the move-in date was used.
Missing values
In 16.2% of the sample, RUCA and/or SDI information was missing due to missing or invalid ZIP code information or because a ZIP code did not have a corresponding RUCA or SDI value. To account for missingness in these variables, multiple imputation by chained equations with 30 imputations was performed using Stata 17. Missing values of the categorical RUCA and SDI variables were imputed as functions of all other study covariates, the number of months enrolled in Medicaid during the 3 months before PSH entry, an indicator for departure from PSH during the study period, and the Nelson–Aalen estimate of the cumulative hazard function for program tenure. 27
Analytic methods
Survival analysis of the time until PSH program exit was performed, with death and the end of the study period as censoring events. A Kaplan–Meier survival function was estimated for all participants to assess their overall probability of remaining in the PSH placement at specific time points. Using the imputed data sets, Cox proportional hazards models were fit to estimate the association between study covariates and program tenure. To test the assumption of proportional hazards, a Cox model was fit with interactions between tenure and all covariates. In a Wald test of the time-varying coefficients, the null hypothesis that all interaction term coefficients were equal to 0 was not rejected, that is, evidence of a violation of the proportional hazards assumption was not found. Hazard ratios (HRs) and 95% confidence intervals (CIs) for all covariates are presented.
In the primary analysis, all exits from PSH were treated as failure events, including exits that may have occurred for both positive reasons (eg, moving to be closer to family) and negative reasons (eg, eviction). The authors examined the feasibility of performing a sensitivity analysis in which only exits for negative reasons would be classified as failure events, using property managers' reports of participant exit reasons to distinguish between positive and negative exits. However, this analysis was determined to be infeasible due to a high degree of missingness and ambiguous information (eg, exit due to “personal reasons”) in the exit reason variable.
Results
In total, 2,093 PSH participants who met study inclusion criteria were identified. Participants had a mean age of 48.1 years (standard deviation [SD] = 13.5) upon moving into PSH, and 57.9% were female (Table 1). A majority of participants identified as non-Hispanic Black (52.6%). A total of 20.7% resided in an institutional setting during at least half of 1 of the 3 months preceding PSH move-in.
Characteristics of Adults with Disabilities in a North Carolina Permanent Supportive Housing Program, 2014–2020
Resided in institutional setting during at least half of 1 of 3 months before PSH move-in.
Ever dually enrolled during the 3 months before PSH move-in.
Participants could have multiple potentially disabling condition types so category percentages do not sum to 100.
PSH, permanent supportive housing; SD, standard deviation; SDI, Social Deprivation Index.
Nearly two thirds of participants had diagnosis codes for a severe mental illness, and the next most common potentially disabling condition types were other severe chronic conditions (59.4%), such as diabetes, cardiovascular disease, or HIV, and physical disorders (58.9%). Participants were concentrated in metropolitan and micropolitan zip codes with an SDI score at or above the median for North Carolina ZIP codes (indicating greater social deprivation), both before and during their PSH placement.
Participants spent a mean of 929.7 days (SD = 482.0) spent in PSH during the study period. A total of 40.3% of participants exited PSH during the study period for reasons other than death, and 6.5% died during the study period (Table 1). Information on departure reasons was missing for 36% of participants who exited PSH during the study period, but eviction was the modal departure reason (48%) among those with available departure information. Figure 1 shows the unadjusted Kaplan–Meier survival curve of estimated PSH tenure for all participants. Based on the unadjusted Kaplan–Meier survival function, 98.5% (95% CI = 97.8%, 98.9%) of participants were estimated to remain in their PSH placement for at least 90 days, 85.8% (95% CI = 84.2–87.2) for at least 365 days, and 70.7% for at least 2 years (95% CI = 68.7–72.7).
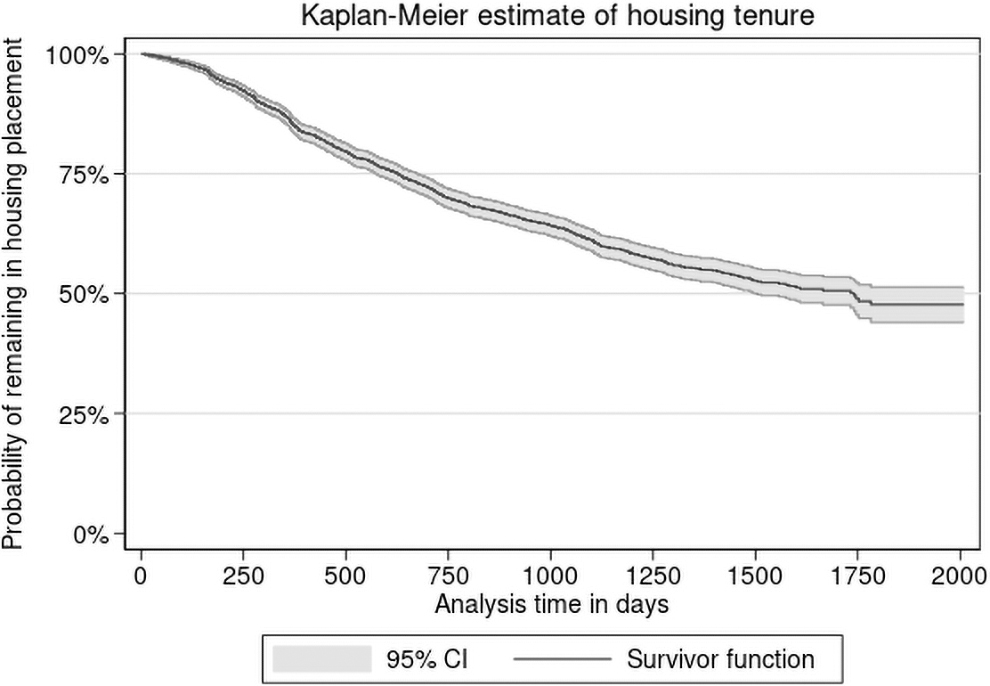
Unadjusted Kaplan–Meier survival estimate of program tenure among PSH participants with disabilities, N = 2093. Program tenure was calculated as the number of days between the housing placement start date and departure date, with death and the end of the study period treated as censoring events. Participants entered the program between 2015 and 2018, and housing placement departure dates were observable until July 3, 2020. Information on program tenure was retrieved from administrative data on the PSH program obtained from the North Carolina Department of Health and Human Services and the North Carolina Housing Finance Agency. PSH, permanent supportive housing.
Adjusted analyses using Cox proportional hazards models provide evidence of variation in program tenure by demographic characteristics (Table 2). Controlling for other demographic, clinical, and area characteristics, an increase of 1 year in age was associated with 1.9% lower (HR = 0.981; 95% CI = 0.976–0.987) hazard of PSH program departure. Female participants had a hazard of program departure that was 19% lower than male participants (HR = 0.810; 95% CI = 0.704–0.931), and non-Hispanic Black participants had a hazard of program departure that was 20% lower than non-Hispanic White participants (HR = 0.798; 95% CI = 0.686–0.927).
Association Between Individual and Area Characteristics and Permanent Supportive Housing Program Departure Among Adults with Disabilities (N = 2093), 2014–2020
HRs and 95% CIs were retrieved from Cox proportional hazards models with multiple imputation of missing values. HR values >1 indicate factors are associated with shorter duration of PSH program tenure.
Resided in institutional setting during at least half of 1 of 3 months before PSH move-in.
Ever dually enrolled during the 3 months before PSH move-in.
Participants could have multiple potentially disabling condition types.
SDI percentiles calculated using all North Carolina zip codes with a valid SDI score.
p < 0.05.
CI, confidence interval; HR, hazard ratio; PSH, permanent supportive housing; SDI, Social Deprivation Index.
With respect to clinical characteristics, having diagnosis codes for a severe mental illness was associated with 22% greater (HR = 1.218; 95% CI = 1.027–1.444) hazard of program departure. Being dually enrolled in Medicare before PSH move-in was associated with 16% greater (HR = 1.163; 95% CI = 1.011–1.338) hazard of program departure. No significant differences in PSH program tenure were detected between those with and without other types of potentially disabling conditions or between those who were institutionalized before PSH and those who were not. Characteristics of the area where participants lived before and during their PSH placement were not found to be associated with PSH program tenure.
Discussion
In this study of a statewide PSH program in North Carolina serving low-income adults with disabilities, participants had a 71% probability of remaining in PSH after 2 years. However, for participants diagnosed with a serious mental illness, shorter program tenure was observed relative to those without SMI diagnosis codes, adjusting for other individual and housing placement area factors. Unlike prior research, no significant differences in program tenure between those with and without substance use disorders were detected. 13,15
Populations under-represented in the PSH literature (ie, those with physical conditions, IDD, or other severe conditions and those transitioning from institutional settings) did not face an elevated risk of PSH program departure in this study. Participants in the housing program studied could qualify on the basis of multiple disability types, in contrast to most prior PSH research that has focused on individuals with severe mental illnesses and/or substance use disorders. The PSH program in this study was also novel in its inclusion of individuals transitioning to PSH from institutional settings and other community-based settings, as well as those who were chronically unhoused.
This study also provides evidence of heterogeneity in PSH program tenure by individual demographic characteristics. Older age was associated with greater program tenure in these analyses, consistent with findings from an evaluation of a supportive housing program serving unhoused individuals with SMI. 13 Black participants and female participants in the study also had longer program tenure, adjusting for other individual and area characteristics. Given that low-income Black individuals and women face a greater risk of housing instability in US society broadly, this finding is surprising. 28,29 Future research should seek to identify the mechanisms underlying these associations by examining any differences in program experiences reported by participant subgroups.
This study also assessed the role of PSH placement area characteristics as predictors of program tenure. No evidence of an association between the level of socioeconomic deprivation of the ZIP code in which the PSH placement was located and participant program tenure was found. This finding is surprising in light of the extensive body of literature showing that community integration among individuals with SMI in PSH is related to area characteristics such as neighborhood safety and resource availability. 30
Prior studies of PSH retention have largely focused on programs in a single city or county. 11,12,15 Because this study evaluated a statewide program, it captured greater diversity of placement locations allowing for comparison of placements across a range of rurality levels. The analyses did not show any evidence of an association between the rurality of either the pre-PSH placement ZIP code or the ZIP code of the PSH placement itself, despite likely differences in the resources available to individuals in rural versus urban placements.
Limitations
A limitation of this study is that available data did not allow the authors to distinguish between voluntary and involuntary exits from PSH. Some participants may voluntarily leave PSH programs to enter housing arrangements that they perceive as granting greater independence, 31 whereas others may involuntarily leave, potentially reflecting unmet health needs or inadequate independent living skills. 32 Although robust information on PSH departure reasons from the perspective of participants was not available, a high prevalence of eviction was observed among those with recorded departure information, suggesting that involuntary departures were common in the sample.
The analyses were also subject to several other limitations. The PSH program data did not contain information on characteristics of participants' housing placements. Although PSH placement area characteristics were included in the model, information was not available about features of the housing itself (such as the quality of the housing environment), which may also influence program retention. 13 Data regarding sources of informal support that PSH participants may have had available to them (such as family caregiving and other social support) were also not available, although such supports are likely an important determinant of program outcomes. 33
Estimates of the association between area characteristics and program tenure may have been biased by the use of measures at the ZIP code level. ZIP codes represent postal service delivery areas and do not necessarily reflect areas with coherent geographic boundaries and homogeneous socioeconomic conditions. 34 Measures at a more granular geographic level, such as the census tract, may better capture meaningful differences in area characteristics with the potential to influence PSH program outcomes.
Conclusions
Findings from this study suggest that PSH programs have the potential to provide long-term housing for people with disabilities. In particular, these programs may be able to successfully retain subpopulations of people with disabilities who have not traditionally been served by PSH, including those with disability types other than behavioral health conditions and those who transition into PSH from institutions. Participants in the study with a severe mental illness diagnosis in fact had higher risk of leaving the program, which may indicate that they require greater service intensity to stay housed through PSH than participants with other condition types.
The study also provides evidence of variation in program tenure by individual demographic characteristics, including gender and race/ethnicity. These findings point to the need for future quantitative and qualitative research to uncover reasons for PSH program exit within specific subpopulations of people with disabilities. Maximizing tenure in PSH among people with disabilities may in turn increase the magnitude of the potential health benefits associated with these programs.
Footnotes
Acknowledgments
The database infrastructure used for this project was supported by the Cecil G. Sheps Center for Health Services Research and the CER Strategic Initiative of UNC's Clinical and Translational Science Award (UL1TR002489). The North Carolina Division of Health Benefits and the North Carolina Housing Finance Agency provided the data used in this study. The North Carolina Division of Health Benefits and the North Carolina Housing Finance Agency do not take responsibility for the scientific validity or accuracy of methodology, results, statistical analyses, or conclusions presented.
Authors' Contributions
Dr. Grove conceived the study, performed statistical analyses, and led article writing. Dr. Domino provided study oversight. Dr. Berkowitz, Dr. Cuddeback, Dr. Pink, Dr. Stearns, and Dr. Domino guided study design and interpretation of findings and provided critical revisions of the article for important intellectual content.
Author Disclosure Statement
Dr. Domino has received funding on unrelated projects from the North Carolina Department of Health and Human Services.
Funding Information
This research was partially supported by a National Research Service Award Pre-Doctoral Traineeship from the Agency for Healthcare Research and Quality sponsored by The Cecil G. Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill, Grant No. T32-HS000032.
Potentially Disabling Condition Definitions
| Potentially disabling condition type | Conditions included |
|---|---|
| Intellectual/developmental disorder (IDD) | Developmental disabilities Pervasive developmental disorders Intellectual disabilities |
| Severe mental illness (SMI) | Bipolar disorders Depressive disorders Schizophrenia and other psychotic disorders |
| Substance use disorder (SUD) | Alcohol-related disorders Substance-related disorders |
| Physical condition 35 | Rheumatoid arthritis and related disease Osteoarthritis Spondylosis, intervertebral disk disorders, other back problems Other connective tissue diseases Other bone disease and musculoskeletal deformities Nervous system congenital anomalies Musculoskeletal congenital anomalies Joint disorders and dislocations, trauma related Spinal cord injury Skull and face fractures Fracture of vertebral column without mention of spinal cord injury Fracture of pelvis Crushing injury Hereditary and degenerative nervous system conditions Paralysis Disorders of the peripheral nervous system |
| Other severe chronic condition | Diabetes mellitus with/without complication Acute myocardial infarction Coronary atherosclerosis and other heart disease Congestive heart failure, nonhypertensive Cerebrovascular disease HIV infection Chronic kidney disease Chronic obstructive pulmonary disease Chronic obstructive pulmonary disease and bronchiectasis |