
Abstract
Strategies to reduce suffering and expense for complex and costly patients have met with limited success. This may be due to both the ongoing dependence on transactional relationships and the failure to recognize anxiety spectrum disorders as a primary driver of medical complexity. The authors describe an emerging current of thought regarding a universal approach to the conceptualization of anxiety disorders and extend it for application to medical complexity. Using 4 cases, they illustrate distinct anxiety–complexity patterns and describe how a relational intervention untangled and identified treatment targets within that process, with excellent results for patients, providers, and payors. They go on to propose future directions and implications of this intervention.
Complex and costly patients—the small percentage of patients who drive the majority of health care costs—are a major focus of all payors, but elegant strategies to reduce costs and relieve suffering in this population have proven elusive. Those interventions that do show promise tend to increase care coordination, follow-up, and social services through interdisciplinary care teams. 1 However, if sustained success depends on perpetual intensive engagement with individual patients, costs remain high and intensive resources cannot be freed for further population-wide use. Therefore, successful interventions must stabilize and ensure sustainability.
The authors hypothesize that the low impact of prior efforts to address complex and costly patients is due to 2 primary and complementary omissions.
The largely transactional nature of both provider–patient and provider–provider relationships. A standardized exceptional patient experience is vital for health care improvement, but for the minority of highly complex patients, standardization does not account for their unique needs. They require individualized, relational, highly adaptive, and flexible care.
The failure to recognize and treat anxiety as a main driver of suffering and utilization. Mental health comorbidity highly increases the impactability of interventions for high complexity. 2 In working with 18 highly complex patients over the past year, anxiety became the main narrative for most patients.
This approach to complex and costly patients in a large academic Accountable Care Organization (ACO), using a medically informed psychiatrist supported by a care manager and a dietitian, has already been published (in press). The team met weekly to review patients, and the care manager and dietitian were free to engage with each patient as needed. Following are 4 case studies that illustrate emerging understanding of the central role of anxiety and the importance of a relational approach for costly and complex patients.
Pronovost et al previously described the suboptimal patient, provider, and system behaviors that prevent patients from getting and staying well.
3
In designing this intervention for complex and costly patients, the hypothesis was applied to these ideas by diagramming a comprehensive conceptualization of each patient's unique system of illness, including all their relevant medical, behavioral, and social factors. This would allow for individualized patient care plans, which was built using an outside-in strategy of recovery, simultaneously: Targeting first-order problems (the 1 or 2 primary pathologies that drive the overall system of illness), containing risky higher order problems (those that can lead to decompensation and unplanned care), and fostering relational interactions between providers and patients.
Initial patients were drawn from the hospital system's employee care plan, a population of 35,000 patients across 18 hospitals and >350 Primary Care Providers (PCPs). Potential patients were identified by filtering out all but the 5% highest risk adults who also had a recent behavioral health billing code, and those with the highest rate of unplanned care in the past year were recruited through their PCPs.
Because half of the target population met criteria for bariatric surgery, case conceptualizations were organized according to obesity as the first-order problem. Progress stalled, so obstacles were explored more deeply through care team coordination and ongoing behavioral reassessment. This led to a reconceptualization that placed anxiety spectrum disorders—a broad category encompassing depression, anxiety, and emotional dysregulation—as the common first-order problem. Once this was identified, the team educated patients and care teams not only on the nature of their anxiety, but also exactly how it drove their systems of illness. This shared understanding, along with targeted psychiatric therapy and behaviorally informed accommodation of the overall treatment plan, cleared a pathway for progress and stabilization.
Anxiety spectrum disorders are the most common and costly mental disorders in the United States, taxing the economy for $46 billion annually in the 1990s. 4 Their prevalence is at least as high as 53% in this intervention's highly complex, commercial insurance population. Even this high percentage is certainly an underestimate, as it does not capture undiagnosed anxiety spectrum disorders, functional disorders, or subthreshold maladaptive behaviors. In each of the 17 patients worked with to date, this conceptualization and approach have sparked progress. It is reasonable to suspect that the vast majority of highly complex patients can be understood and treated according to this model.
Anxiety Spectrum Disorders
To understand how anxiety can drive medical complexity, it is necessary to elucidate the common pathology underlying all anxiety spectrum disorders. Although depression, anxiety, and personality disorders are classified separately in DSM-5, an emerging line of thought looks to unify classification, which could be immensely helpful in simplifying the integration of behavioral concepts into complex medical care, as will be shown. This shift arises from 3 realizations:
Symptoms of all anxiety spectrum disorders are highly comorbid across the lifespan.
Treatments targeting one anxiety spectrum disorder are often effective for symptoms of emotional comorbidities.
Advances in neuroscience demonstrate common neural pathways shared by all anxiety spectrum disorders. 5
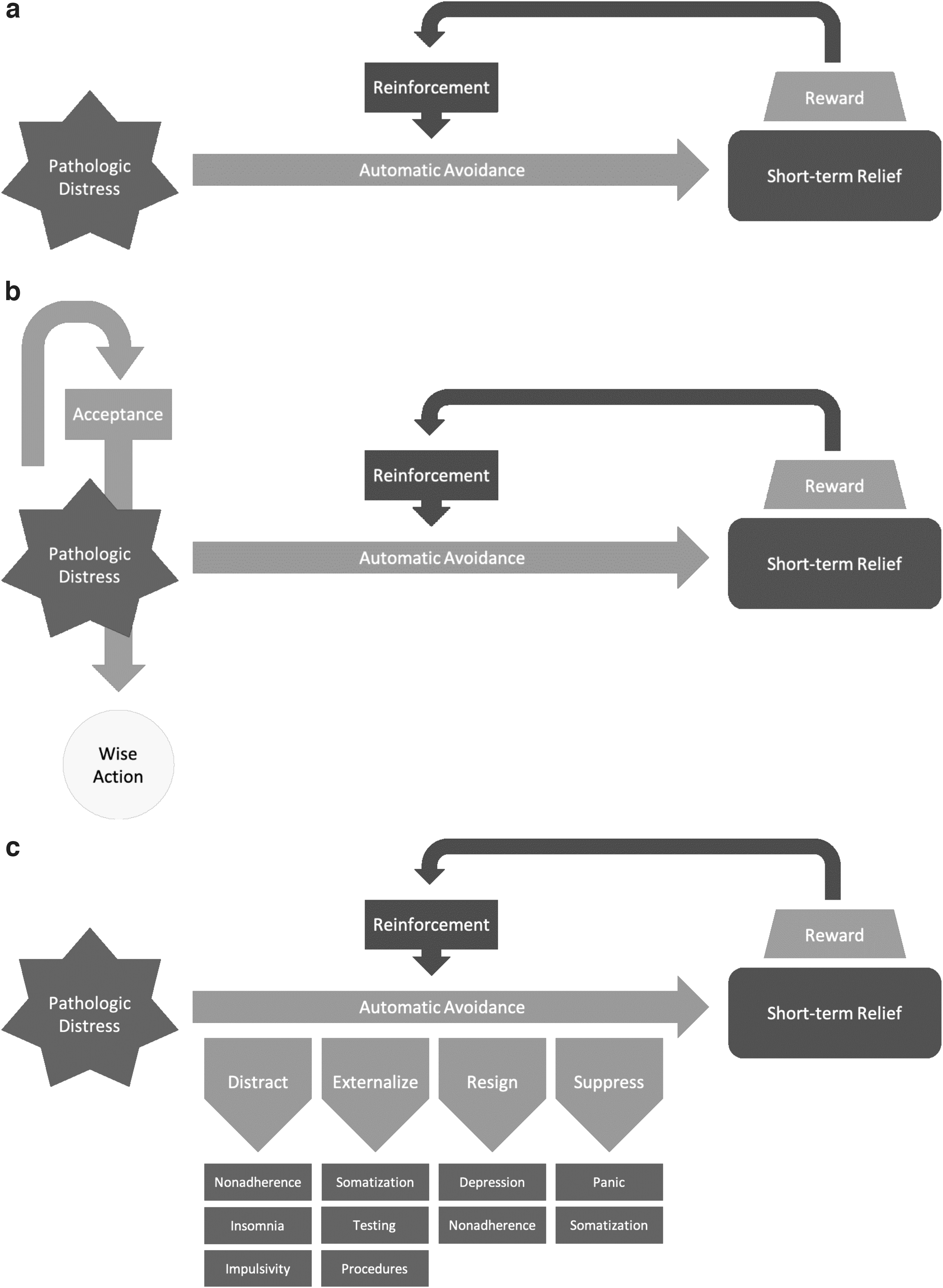
The nuances of all the separately classified anxiety spectrum disorders can be reduced to a unifying pathology to inform diagnosis and treatment as illustrated in Figure 1a and explained below.
The power supply
The anxiety process is powered by an underlying, pathological distress, which arises from the interaction of core factors:
A heightened expectation of threat or danger
Catastrophic interpretations of stimuli (internal: physical, emotional, cognitive) or events (external)
Biased expectations of negative outcomes. 6
The balance of these factors helps define various disorders, all of which are characterized by a constant fear of, and defense against, negative emotional states such as anger, sadness, and fear itself. Post-traumatic stress disorder (PTSD) is defined by fear of intolerable distress triggered by trauma reminders. In generalized anxiety disorder, in contrast, biased expectations of negative outcomes drive constant worries of inevitable, intolerable distress. In all cases, the pathological distress is magnified, reinforced, and greatly extended by maladaptive avoidance mechanisms.
The circuitry of avoidance
The mind's normal response to distress is to try and make it stop as soon as possible. When an external factor is the cause, it is adaptive for an organism to resolve it quickly. However, internal sources of distress cannot be dealt with in such a straightforward manner. Frantic attempts to avoid internal distress can lead to reward in the form of short-term relief, in which case they are reinforced and become conditioned behaviors. The manifestations of automatic avoidance can be obvious, such as numbing with intoxicants or risk-taking, distraction by constantly keeping busy, or simple physical avoidance of triggers.
However, the mechanism of reward can also be less intuitive. By engaging in worrying, the mere act of mental problem-solving triggers reward, despite being unpleasant and functionally impairing. Similarly, when distress begins to feel overwhelming, hopelessness can lead to depression, and the relief afforded by mentally “giving up” actually reinforces depression as a conditioned response. A complex circuit of interlacing, impairing avoidance behaviors is wired together over time, and another core belief—“I can't handle this distress”—becomes further reinforced and solidified. 7,8
Lasting treatment
Appropriate psychiatric medications can help decrease the intensity of the power supply—the core distress—and psychotherapy can help establish new, helpful behaviors that wire adaptive circuits to compete with the pathological, as shown in Figure 1b. The central tenet of psychotherapy for anxiety disorders is that the mind must be trained to turn toward distress, not avoid it. Accommodating distress openly helps the patient gain self-efficacy and softens the mind's impulse toward avoidance. Techniques such as exposure therapy and mindfulness-based therapies are built around this principle. These can be individualized to specific illness systems and incorporated throughout care plans, helping patients manage their distress and maintain adaptive health behaviors.
It is easy to imagine how avoidance behaviors could directly or indirectly cause and maintain medical complexity, and this is explored through 4 case studies, each of which represents a distinct pattern of complexity formed by its underlying anxiety disorder. Each pattern here revolves around obesity and obstacles that arose while working with the bariatric surgery clinic.
The first patient had already met with the bariatric surgeon, but was terrified to consider surgery. In the second case, the patient was highly motivated for surgery and seemed to be making progress with limited team engagement, but her continued high engagement with various care providers forced us to reconsider. The third case had successfully lost >100 lbs after her surgery, but was struggling terribly after eventually regaining all the weight. The fourth case had also regained weight, but was more focused on problems at home and at work.
Case 1: Health Care-Avoidant Illness Anxiety and Respiratory Dysfunction
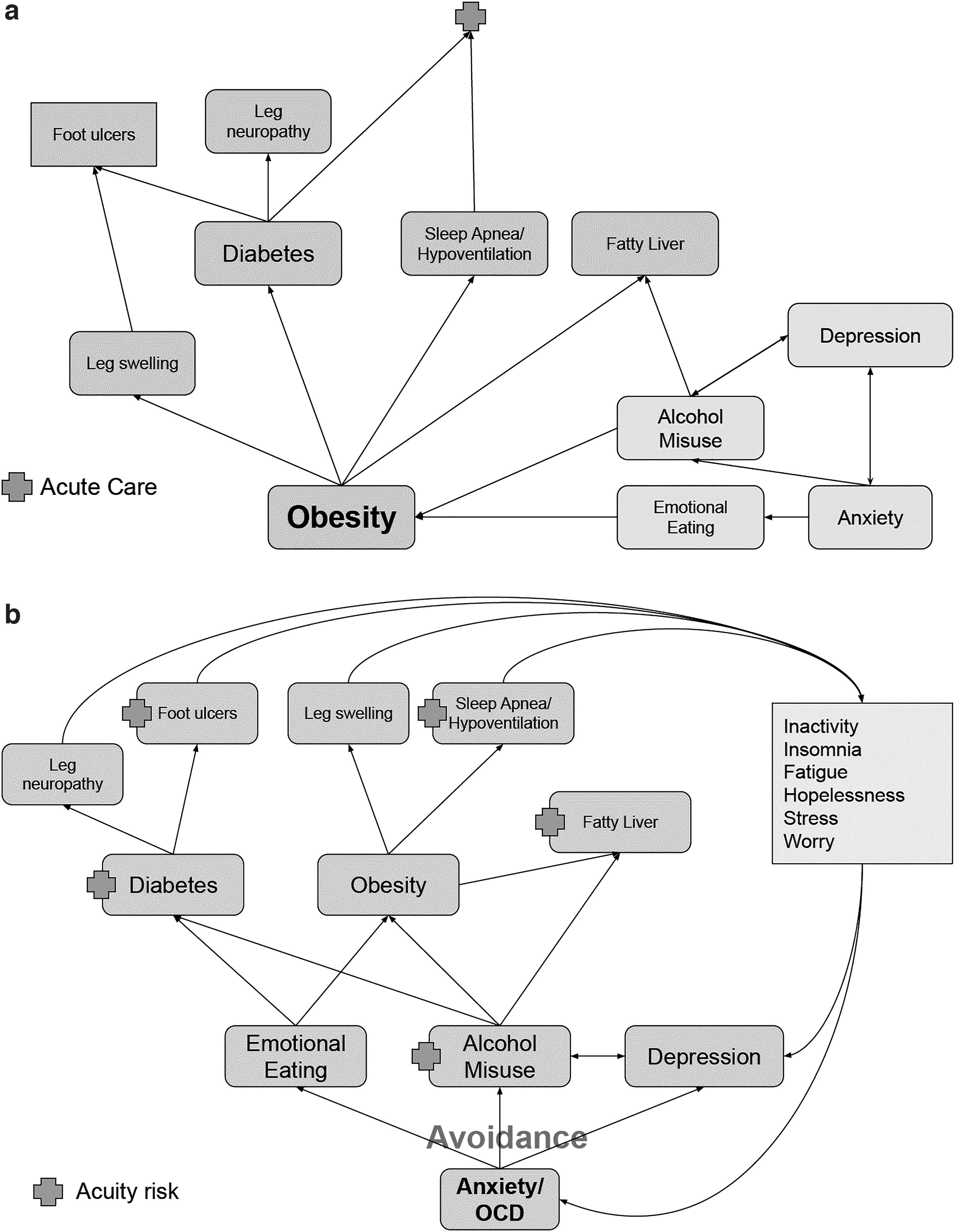
Susan was a married woman in her 40s with class 3 obesity, type 2 diabetes, obstructive sleep apnea, recurrent lower extremity swelling and ulceration, fatty liver disease, unspecified anxiety, and unspecified alcohol misuse. Just before the coronavirus pandemic, she had required intubation and ventilation during treatment of a streptococcal community-acquired pneumonia. The intervention team suspected that the severity of her infection was influenced by the combination of untreated sleep apnea, obesity hypoventilation syndrome, and poorly controlled diabetes.
They initially conceptualized her illness system as illustrated in Figure 2a and began applying motivational interviewing to encourage Continuous Positive Airway Pressure machine (CPAP) and lifestyle change adherence. Although the patient was highly motivated and engaged, various recommendations failed due to one reason or another. It eventually became apparent that her other care teams were having similar difficulties. After looking for hidden barriers to adherence, a series of key discoveries led to the understanding that her behavior was being guided by severe anxiety.
When she was a teenager, her mother died unexpectedly of medical complications, and she began having panic attacks about her own health. Desperately avoiding these thoughts, she could not intentionally engage in healthy behaviors. Stress eating eventually led to obesity and its complications. Anxiety was worst at nighttime—alone, in the dark, the reality of death was especially salient. She started drinking heavily in the evenings to prevent this nighttime distress, and when she eventually required CPAP therapy, she was too intoxicated at bedtime to use it.
By the time of intervention, she was always worried about her health and desperately wanted to improve it, but any attempt to adhere to recommendations forced her to confront her anxious distress and was abandoned. Not surprisingly, she sometimes became overwhelmed and depressed. Her illness system was reconceptualized as shown in Figure 2b.
The team then met with the patient and her family, reviewed this conceptualization, and explained how this anxiety drives avoidance behaviors. She was referred to a psychologist to start cognitive-behavioral therapy (CBT) for anxiety and incorporated her new understanding into treatment adherence. Whenever she identified a barrier to treatment, the team explored the situation more fully to see how illness anxiety was driving avoidance, then reinforced CBT skills to help follow through with her medical plan. Since then, she has stopped drinking alcohol, sleeps well, controls her diabetes, and is losing weight. Her annual health care spend has decreased from $38,000 to $6000 since enrolling in the intervention.
Susan's pattern is an excellent illustration of how avoidance by distraction can create and maintain medical complexity (Fig. 1c). Everyone experiences the tendency to distract themselves from distressing thoughts, but in an anxiety disorder, this becomes second nature. Because the underlying fear is too distressing to bear, reminders of it are frantically avoided and replaced with more superficial worries.
When those fears are triggered by medical disease, this takes the form of nonadherence, often with insignificant and inconsistent explanations for treatment intolerance. Distraction also creates disease in the first place through chronic impulsivity, such as with binge eating, substance use, or risky sexual behaviors. Patients have more difficulty distracting themselves at bedtime, when they find themselves alone with their distressing thoughts and unable to sleep. This can then lead to chronic fatigue, physical inactivity, and lower emotional reserve.
Case 2: Health Care-Dependent Illness Anxiety and Chronic Neuropathic Pain
Jeannie's case seemed relatively straightforward. Her unplanned visits focused around various neuropathic and musculoskeletal pains, as well as one episode of mild dyspnea, that appeared to be related to obesity. She also had obstructive sleep apnea with poor CPAP adherence, but readily agreed to begin using CPAP nightly, and was excited by how much better she felt. She was very interested in bariatric surgery, was referred to that clinic, and began adhering properly to dietary and lifestyle changes. She engaged minimally with the intervention team, which suspected her complexity was too low for ongoing participation, and planned to complete her program of care. However, as part of that process, they noticed that she had a pattern of seeking subspecialty care and, in some cases, receiving further workup, even after being reassured by her PCP. Because these visits were scheduled, the team had paid them less attention.
Although she initially denied any anxiety, this was reassessed with a specific focus on her feelings surrounding physical symptoms and medical testing. She noted high levels of distress with near-constant ruminations about physical sensations. Negative medical workups did not reassure her; she only worried more that something had been missed. If a specialist ordered a study that her PCP had deemed unnecessary, she lost confidence in her PCP, and was even thinking about terminating their relationship. Revisiting an earlier recommendation of as-needed abortive therapy for migraines (after an unplanned visit), it was found she was taking this medication multiple times per week for any kind of mildly unpleasant cranial sensation.
Looking back, the patient described these worries as starting just a few years back, after caring for her ailing mother in a nursing home. Staff were inattentive and the patient ended up assuming most of the care duties herself. After her mother died, her focus shifted to her own health. Similar to the first case, her worries focused on health, but rather than try to push these thoughts away, she felt compelled to solve them through diagnosis and treatment. One can imagine how this thought process might respond to bariatric surgery: hypervigilance surrounding gastrointestinal symptoms leading to multiple workups, surgical revisions, food avoidance, and malnutrition. The patient was open to a frank discussion about these concerns and agreed to seek treatment for illness anxiety before progressing with bariatric surgery preparation.
She initially required constant and assertive intervention to reinforce and remind her of these concepts and to schedule follow-up appointments with her psychologist. Eventually, she became aware of how anxiety was distorting her interpretation of physical sensations, and began reinforcing this with mindful practices. She expressed relief and reassurance that her most recent workup for a medical concern was negative. The relational nature of the intervention team's relationship has been essential for building trust, given the oppositional force of a mind that struggles against acceptance. And even though it took several months to get to this point, her annual spend during this time decreased from $17,000 to $7000.
Jeannie's underlying pathological distress was her fear of becoming ill and slowly dying while being neglected. This outcome was so distressing that her mind catastrophized any feeling of discomfort. Everyone struggles to accept the inevitability of sickness, old age, and death, but for the patient with medical illness anxiety, these stages feel both unbearably close and absolutely unacceptable. Comfort is found in the idea of external control, which is realized through constant hypervigilance of physical sensations.
Any twitch or tingling could lead to the discovery of a serious illness that can be treated and cured, finally providing reassurance that sickness and death are avoidable. Negative test results are reassuring for most people, but here, they are a disappointment: uncertainty and fear must continue. The externalization pattern of avoidance, as shown in Figure 1c, leads to constant seeking for a disease to be treated, in hopes that underlying fear can be taken away.
Case 3: Atypical Eating Disorder and Recurrent Malnutrition
Unlike Jeannie, Lisa's underlying anxiety spectrum disorder was not fully understood before bariatric surgery. She had a history of undiagnosed self-harm and restrictive eating during adolescence, but these symptoms eventually resolved, and she was maintaining a stable career and home life. However, she was still consumed by feelings of low self-worth and body image anxiety, which could sometimes lead to strong feelings of sadness or anger at herself. Some concerns were discussed at her psychological screening for bariatric surgery, but the decision was made to proceed. She did extremely well, losing >100 pounds before plateauing.
Once her weight loss slowed, her feelings of low self-worth and anxiety came back in full force, and she developed a cycle of binge eating and restriction. This, in turn, led to regaining all of the weight she had lost. She began suffering from multiple episodes of nausea and vomiting leading to malnutrition and hospital admissions for IV nourishment. Because this occurred so frequently and her vascular access was so difficult, her surgeon inserted a gastric tube, which led to further unplanned care for related complications. When the intervention team met her, she was chronically depressed.
Eating disorders may vary over time and are commonly comorbid with emotional disorders. Lisa's case was confusing because, although she endorsed food restriction and presented with malnourishment, she continued to gain weight. She also endorsed recurrent vomiting that was at times self-induced, but sometimes spontaneous. Care team alignment was blocked by the absence of communication between her bariatric surgeon, psychiatrist, and therapist, each of whom belonged to different health systems. Once her disparate care teams were aligned, a plan was made to replace or remove potentially exacerbating medications, remove the gastric tube, and offer admission to a residential eating disorder treatment facility.
Since then, Lisa has understood more fully that her distress arose from low self-worth associated with physical perfectionism, and that her mind avoided and suppressed that distress in multiple maladaptive ways, such as bingeing and purging, hyperfocusing on gastrointestinal sensations, and feeling overwhelming pressure not to disappoint her care teams. She continues to work on skillful responses to her emotions, has been eating well, and has not had another episode of unplanned care in many months. Even though her intervention involved extended residential mental health treatment, her overall cost of care decreased dramatically, from $176,000 in 2020 to $90,000 in 2021.
Eating disorders may manifest in different ways over the lifespan, especially when underlying anxiety spectrum disorders are unresolved. In this case, Lisa's eating disorder was driven by her low self-worth and chronic depression, illustrating the “resignation” pattern (Fig. 1c). When there is no end in sight, patients may resign themselves to the inevitability of distress and become depressed. This is in stark contrast to acceptance, which opens up to distress.
Resignation is a form of avoidance, where the hopelessness of the entire pathological network is embraced. The cessation of frantic attempts to escape is experienced as relief, and the pathway to depression is reinforced. Most patients with anxiety spectrum disorders become depressed at times, and many patients with depression may recover only to again feel trapped by anxiety. The effects of depression on physical health have been well described, and associated anhedonia hinders treatment adherence.
Case 4: Chronic PTSD with Panic Attacks
Linda also regained all of her weight after initial postsurgical success, and her chart told a story of chronic pain and unplanned care for dyspnea, possibly related to obesity hypoventilation syndrome. However, on engagement, she was not concerned with her weight or pain symptoms, instead asking for help with overwhelming stress at work and at home. She was struggling to master the details of a new job, feeling unsupported by her supervisors. She was in the process of selling her house and moving in with her mother, who had advancing dementia and needed more support.
Her dyspnea was due to panic attacks while at work, and so the team began by focusing on her anxiety. After meeting with her and her family together, they discovered that she had debilitating fear in many standard situations. This led to further discovery that her childhood was filled with recurrent trauma and fear.
She suffered from severe PTSD with high situational avoidance, and had managed to adapt her life around these restrictions. However, with multiple new stressors, avoidance was becoming impossible, leading to panic attacks. She acknowledged that her obesity was a protection against unwanted attention from men, and she only became concerned with weight when stress eating increased her body mass beyond the point of feeling safe. Because treatment of PTSD can itself be stressful, the team supported her closely through financial, work, and life changes, and by helping her to manage panic attacks, maladaptive thoughts about eating, and other forms of health-related avoidance.
Through this process, they built a strong relational relationship, and as she learns to accept and work with her fear, she has been able to react more skillfully to life stressors and feel comfortable losing weight. She has become much more independent, is working consistently with a therapist, and is better able to process through panic attacks on her own, rather than going to the emergency department. New and serious social stressors have emerged during this time, however, and while her annual spend remains around $10,000, it may have been much higher without the intervention.
Although Linda had certainly relied on distraction and resignation avoidance patterns, the utilization aspect of her case best illustrates suppression (Fig. 1c). Similar to distraction, this pattern actively denies and pushes away distress. The struggle is not to escape, but rather to contain. Suppression can be very difficult to work with, as denial can prevent patients from recognizing or disclosing their distress to providers. In addition, emotion suppression can lead to chronic pain or gastrointestinal distress, which can then lead to externalization. 9 When distress becomes too overwhelming to be pushed away, it may manifest as intense fear accompanied by an acute autonomic response, or a panic attack. And when complex patients also suffer from cardiac or respiratory pathologies, the uncertain nature of these attacks can be even more distressing.
Conclusion: Future Directions of Team-Based Intervention for Complex and Costly Patients
In all these cases, it is apparent how a pattern of behavior can inform diagnosis of an underlying anxiety spectrum disorder, which can then be used to help classify and target distinct patterns of medical complexity. Furthermore, almost all of the 17 patients seen thus far have begun to improve after comprehensive conceptualization with the anxiety disorder as the driving, first-order problem. With an understanding of the wide variety of avoidance behaviors that can become reinforced in response to pathological distress, it is easy to see how anxiety can be at the root of complexity, and how the unique ways in which anxiety drives complexity need to be mapped out and understood by the patient and all members of their care team.
Anxiety often goes unrecognized, but even when discovered, targeting it as a separate process may diminish its importance in the eyes of the patient. They may even think, “I need to get my medical problems under control before I put all this effort into changing my thought patterns.” Maladaptive medical behaviors may go unrecognized by mental health professionals who have not been trained to look for them, and well-intentioned medical care team members may inadvertently reinforce or exacerbate avoidance behaviors through misinformed testing, counseling, or intervention.
The connections between avoidance patterns and medical complexity exist in a space that has been largely neglected in the health care system. With a few exceptions, such as with chronic musculoskeletal pain syndromes, most exploration of functional disorders takes place with an emphasis on medical pathology. Anxiety-driven medical nonadherence behaviors are largely unexplored, but their recognition became the key to this intervention's progress. However, success in this middle space required good coordination with and support from the parties on either end.
This means that providers must have the bandwidth to collaborate in fairly unexplored terrain. With patients spread throughout the system, provider engagement and alignment required significant effort. This burden could be reduced by integrating the team into existing comprehensive care packages, such as with advanced primary care (APC) practices. One complex and costly care team could possibly embed within a small number of APC practices, forging strong care team relationships.
Team efficiency can be further increased by recognizing common patterns of complexity. The 4 distinct patterns of medical complexity already discussed were described using currently accepted psychiatric and medical diagnoses. However, the psychology of individual disorders is more nuanced, and this first attempt at a classification of avoidance patterns (into distraction, externalization, resignation, and suppression) is neither comprehensive nor optimal.
As the team increases its patient volume, it hopes to optimize this classification according to simplicity and efficacy. This will not only improve the team's efficiency, but also simplify engagement with care team partners. Medical providers need not understand every nuance of behavior, and mental health providers need not be trained in the details of a host of medical pathologies. But if they each can draw from a limited set of general patterns that drive complexity, the foundation for comprehensive treatment can be put in place easily.
These patterns, as well as the optimal design of the team, will likely vary by population. The work thus far has been with a commercial ACO in a metropolitan region, but there will be different challenges among Medicaid and Medicare populations, and in exurban or rural areas. New patterns of complexity may be discovered that are best served by a different makeup of primary skillsets. In addition, the context of the team's work will guide its needs.
When embedded within APC practices that already have case management and pharmacy support but limited mental health access, the team may work most optimally by replacing its case manager with a counselor. Collaborative care, a different model of embedding within APC practices for less complex patients with depression and anxiety, has produced savings of around $4000 per patient. 10
The impact of interventions for complex and costly patients could be increased by fostering relational patient and provider relationships and by targeting the neglected connections between anxiety spectrum disorders and physical illness. Although this intervention was guided by previous work showing high impactability of case management interventions for highly complex patients with mental health comorbidities, only 67% of those patients were determined to be impactable. The number was much lower for substance use disorders (14%), trauma (14%), unstable social support (23%), and the presence of at least 4 risk factors (15%).
Many of this intervention's patients fall into these categories, and some of their families and care teams had already given up hope of helping them recover. However, the theory and methods already described led to strong initial success. This intervention is fairly inexpensive compared with the return it could generate, and it can become even more efficient. Still in the early stages, continued expansion will hopefully lead to more detailed analysis in future reports.
Footnotes
Authors' Contributions
All authors named have contributed meaningfully to this work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this work came directly from the budget of the hospital system's accountable care organization.