
Abstract
Despite increasing resources dedicated to identifying and addressing social risks in health care settings, many patients screening positive for social risks either decline assistance or do not follow up with offered resources. This study assessed predictors of engagement with offered social care assistance through guided self-navigation or in-person assistance. Data came from a cross-sectional analysis of 6-month follow-up survey data from an ongoing trial of participants with poorly controlled diabetes and a positive social risk screen randomized to guided online self-navigation or in-person social care assistance. Multivariable logistic regression models estimated participant characteristics associated with engagement with offered assistance. Mean age was 55 years (standard deviation = 12). Of 407 participants, 41% (n = 165) engaged with offered assistance: 76% (n = 137) of those in the guided self-navigation arm and 13% (n = 28) of those in the in-person assistance arm. A sizable proportion of participants endorsed already using assistance for medications (30%), food (26%), and employment (22%). Female gender [OR 1.57, 95% CI (1.03–2.40), P < 0.05] and being out of the workforce [OR 1.71, 95% CI (1.07–2.73), P < 0.05] predicted engagement with social care assistance. Those already using assistance for medications [OR 4.71, 95% CI (1.69–13.15), P < 0.05] and blood glucose supplies [OR 6.25, 95% CI (1.45–26.78) P < 0.05] were also more likely to engage with offered assistance. Fewer than half of individuals engaged with offered social assistance through either guided online self-navigation or in-person assistance; limited demographic and clinical factors predicted uptake. More investments are needed to understand how best to support uptake of offered assistance.
Introduction
Increased recognition of impact of the social and behavioral determinants on health outcomes has led to a growing national interest and investment in health care-based social risk screening and resource connection. Yet despite a rapidly expanding number of initiatives dedicated to identifying and addressing social risks in care settings, studies have shown that often 50% or more of patients screening positive for social risks either decline assistance or do not follow up with offered resources. 1 –12
Few studies have examined patient characteristics associated with interest in assistance. In a national multisite study of adult patients and adult caregivers of pediatric patients screening positive for 1 or more social risk factors, De Marchis et al found that participants were more likely to express interest in receiving assistance as the number of social risks increased. 4 Those with lower household income levels and who self-identified as having non-Hispanic Black ancestry were also more likely to accept offered assistance. De Marchis et al further found that the screening approach mattered, as given an otherwise identical self-administered paper screener, participants were more likely to accept assistance if questions assessing interest in receiving assistance were asked before rather than after questions about social risks. 4
Consistent with prior studies, 5,13 De Marchis et al found that a substantial proportion of participants were interested in assistance even if they screened negative for all social risks, with higher likelihood of interest if participants reported lower household income levels, previous exposure to health care-based social risk screening, higher perceived appropriateness of social risk screening, or worse health status. 4 In a health system sample, Gruß et al found that more than half of patients who reported a risk were risk/help concordant (ie, they both screened positive for a risk and also wanted help with that risk), and lower socioeconomic status was often associated with higher rates of asking for help when reporting a social risk. 13
Gaps remain in understanding what patient characteristics and factors are associated with both interest in and engagement with offered resources, and how social care interventions can be tailored to better reach those who may otherwise not engage with offered resources. The purpose of this study was to assess prevalence and predictors of engagement with offered social care assistance through either guided online self-navigation or in-person assistance in a population with poorly controlled diabetes. The authors specifically examined participant demographic, clinical, and psychosocial characteristics; unmet social needs and self-identified risks; interest in and current use of resources by social risk domain; and perceived importance of and preferences for receiving social care information.
Methods
Data sources
This study is a secondary data analysis of 6-month follow-up assessments of a subset of participants in an ongoing randomized controlled trial (RCT) evaluating approaches to addressing unmet social risks among people with uncontrolled diabetes. 14 All study procedures were approved by the University of Michigan Institutional Review Board.
Study sample
Eligibility criteria and recruitment have been described previously. 14 For the RCT, a total of 6055 potential participants were contacted between June 30, 2019, and March, 2022, of whom 997 were confirmed to be eligible. Of those, 666 (66%) consented to participate and 600 were randomized to 1 of 2 study arms: (1) guided online self-navigation—participants in this arm were provided with a unique User ID and password to log into CareAvenue, an interactive website that builds participants' capacity to address financial strain and other social risks while managing diabetes. 14
The website provides additional self-screening for a broad range of social risk factors and includes a series of short animated videos and step-by-step guidance on navigating a set of low-cost resources that map directly to identified social needs; (2) in-person assistance—participants in this arm (active control) were provided contact information for the Guest Assistance Program (GAP) at the University of Michigan Health System. GAP social workers provide assistance with medical and nonmedical needs and resources to patients receiving medical care within the health system.
Of the 600 participants randomized, 407 participants completed 6-month follow-up surveys at the time of this writing, and were included in this study. Ninety-three participants were lost to follow-up (reasons included: not reachable (n = 24), passed away (n = 5), and withdrew from study (n = 64).
Data collection and measures
Baseline and 6-month follow-up telephone surveys were administered by trained data collectors. Baseline self-reported measures included the following.
Sociodemographic, clinical, and psychosocial characteristics
Standard demographic data as well as health insurance coverage and household income were collected. Clinical variables included presence and count of chronic conditions, polypharmacy, and extent of uncontrolled disease through HbA1c and blood pressure measures taken through home monitoring devices. 15 –17 For psychosocial factors, the authors examined depressive symptoms (PHQ-4) 18 and diabetes-related distress, 19,20 health literacy (high vs. low), 21 and social support (high vs. low) (ENRICHD Social Support Inventory) 22 collected through validated survey measures.
Social risks and needs related to diabetes
Participants were asked to self-report endorsement of social risks related to diabetes management and other social determinants, 23,24 interest in assistance, or whether they were already using assistance for each risk. Drawing on prior literature, 4–5,13 for select diabetes-related social risks and clinical needs (blood glucose supplies, medications, food and meals, income support, loan/debt management, employment, housing and utilities, and medical bills), participants were categorized as “already using assistance,” being “risk/assistance concordant” (endorsed a risk and were interested in assistance), “risk/assistance discordant” (endorsed a risk and were not interested in assistance), and “no risk but wants assistance.”
Acceptability, values, and preferences (hereafter “attitudinal factors”)
Participants were asked whether they found the information they received on assistance interesting (5-point Likert scale, strongly disagree–strongly agree); importance of knowing about low-cost options for managing diabetes (5-point Likert scale, not important–very important); and preference for having health professionals provide resources as opposed to seeking information out on their own (5-point Likert scale, strongly disagree–strongly agree). Responses were dichotomized for analysis.
Engagement with offered assistance
Participants were asked at 6-month follow-up whether they had logged onto CareAvenue or followed up with GAP services (Y/N), as relevant based on study arm.
Statistical analysis
Descriptive statistics were calculated for all variables. Bivariate analyses (chi-square tests and t-tests) were used to assess differences in baseline characteristics and social risk/help concordance between those who engaged and those who did not engage with offered assistance, both for the full sample and stratified by study arm.
A multivariable logistic regression model was used to examine the association between sociodemographic, clinical, and psychosocial characteristics that were significant in univariate analyses (gender, race/ethnicity, education, employment, health insurance status, health literacy, depressive symptoms, and social support) and engagement with offered assistance.
The model was adjusted for age. Additional multiple variable logistic regression models were used to estimate the associations between (1) each individual diabetes-related social risk/need and attitudinal factors significant in univariate analyses (information offered was interesting, importance of knowing about low-cost options for managing diabetes) and (2) select individual social risk/assistance concordance domains (medications, food/meals, blood glucose supplies, income support, and employment) and engagement with offered assistance. These models were adjusted for age, gender, and years living with diabetes.
All analyses were completed using SAS statistical package. P-values <0.05 were considered significant.
Results
Sample characteristics
A total of 407 participants were included in the analytic sample (181 in self-navigation and 226 in in-person assistance, Table 1). On average, participants were 55 years of age (standard deviation [SD] = 12), 58% (n = 235) were female, 34% (n = 139) reported non-White race and non-Hispanic ethnicity, and 43% (n = 173) reported a college education or above. Thirteen percent (n = 50) were <100% of the federal poverty level, 13% (n = 53) were 100%–200% of the poverty level, and 73% (n = 298) were 201% or more above the poverty level.
Demographic, Psychosocial, and Clinical Characteristics, and Social Risks of the Sample Associated with Engagement with Offered Assistance (N = 407)
Boldface indicates statistical significance (P < 0.05).
Difference computed between private versus public insurance.
SD, standard deviation.
Ninety-seven percent (n = 397) reported having health insurance. Mean years living with diabetes was 18 (SD = 11), mean A1c was 7.9 (SD = 1.4), and mean systolic blood pressure was 133 (SD = 19). Seventy-six percent (n = 309) reported high health literacy. Mean number of baseline unmet social needs was 5 (SD = 4.6).
Engagement and nonengagement with offered assistance
Forty-one percent (n = 165) of the total sample engaged with offered assistance: 76% (n = 137) of those in the guided self-navigation arm and 13% (n = 28) of those in the in-person assistance arm (Table 1).
Participants' sociodemographic characteristics varied in the full sample between those who engaged and those who did not engage with offered assistance by gender and provision of health insurance, with those who engaged more likely to be female (P < 0.05) and insured (P < 0.05) (Table 1).
For guided self-navigation, those who engaged were more likely to be younger (P < 0.05), non-Hispanic White (P < 0.05), more educated (P < 0.05), employed full time (P < 0.05), and have fewer depressive symptoms (P < 0.05), higher health literacy (P < 0.05), greater social support (P < 0.05), and place lower preference on having a health care provider provide options for low-cost resources (P < 0.05). For in-person assistance, those who engaged were more likely to be female (P < 0.05), non-White race (P < 0.05), and found the information provided interesting (P < 0.05).
Figure 1 shows associations between social risk/assistance concordance and engagement, stratified by guided self-navigation and in-person assistance. Social risks where a sizable proportion of participants were already using assistance were evident for medications (30%), food and meals (26%), and employment (22%). In the full sample, for social risks related to medications, blood glucose supplies, and food and meals, already using assistance, and being risk/help concordant were associated with engagement with offered assistance (P < 0.05).
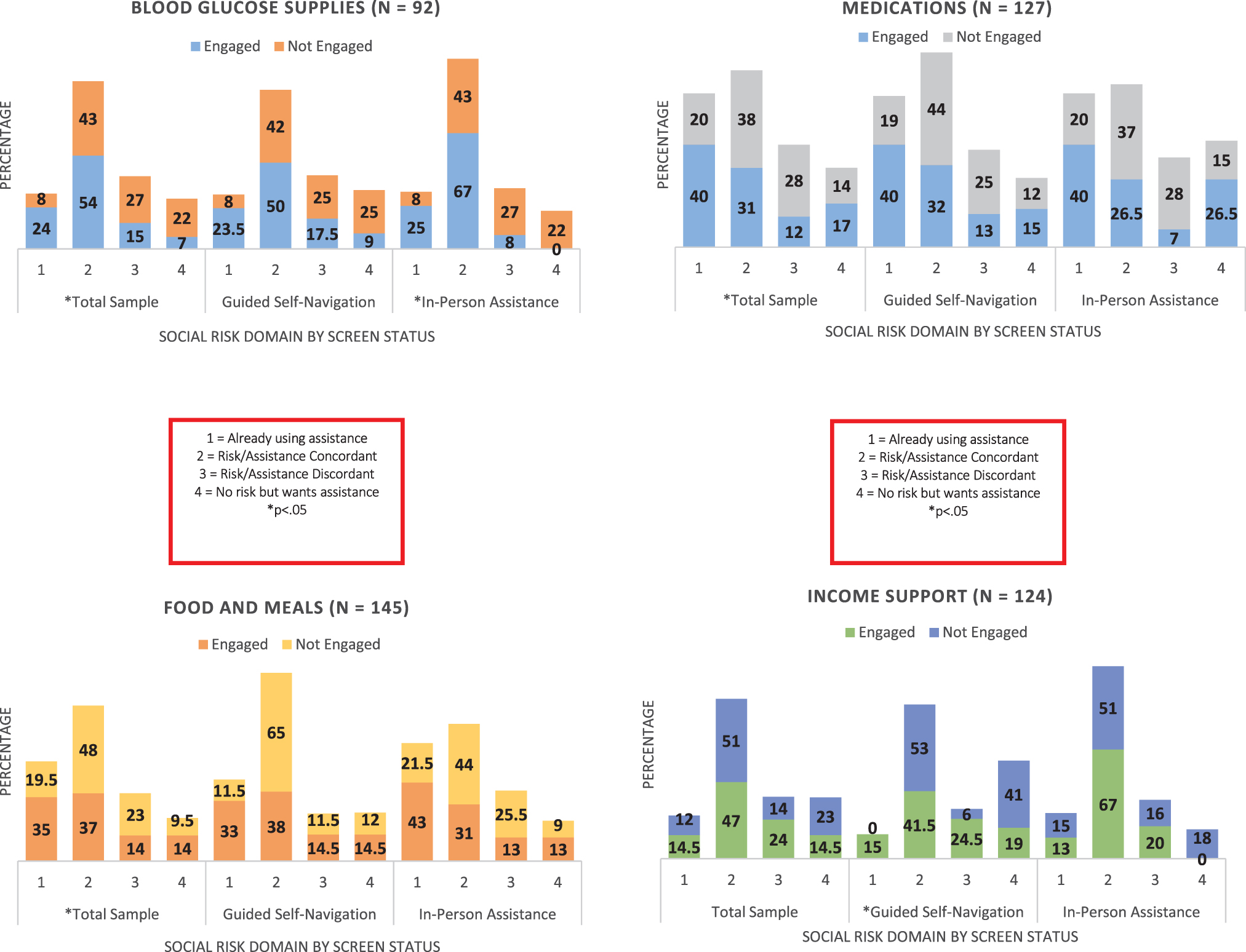
Associations between social risk/help concordance and engagement by guided self-navigation and in-person assistance.

For guided self-navigation, social risks related to income support and employment showed that those already using assistance and being risk/help concordant were associated with engagement with offered assistance (P < 0.05). For in-person assistance, social risks related to blood glucose supplies were associated with engagement with offered assistance (P < 0.05).
Multiple variable logistic regression model of sociodemographic, clinical, psychosocial, and attitudinal predictors of engagement with social care assistance
In a multiple variable logistic regression model adjusted for age, female gender [OR 1.57, 95% CI (1.03–2.40), P < 0.05], and being out of the workforce [OR 1.71, 95% CI (1.07–2.73), P < 0.05] predicted engagement with social care assistance (Table 2). In separate models for each social risk, adjusted for age, gender, and years living with diabetes, the authors found that those already using assistance for medications [OR 4.71, 95% CI (1.69–13.15), P < 0.05] and blood glucose supplies [OR 6.25, 95% CI (1.45–26.78), P < 0.05] were more likely to engage with offered assistance. For food and meals, those who did not screen positive for a risk but reported wanting assistance were also more likely to engage with offered resources [OR 3.40, 95% CI (1.02–11.37), P < 0.05] (Table 3).
Multiple Variable Logistic Regression Model of Predictors of Engagement with Social Care Assistance
Model adjusted for age.
P < 0.05.
REF, reference category.
Multiple Variable Logistic Regression Models of Social Risk Concordance Predicting Engagement with Social Care Assistance
Models adjusted for age, gender, years living with diabetes.
P < 0.05.
REF, reference category.
Discussion
In this sample of adults with poorly controlled diabetes who screened positive for social risk factors, the authors found that less than half of individuals engaged with offered resources through either guided online self-navigation or in-person assistance. Among those who engaged and followed up with resources, differences between self-navigation and in-person assistance were observed. Females and those not in the workforce were more likely to engage with offered assistance. For select social risks, those already using assistance or who endorsed wanting assistance were more likely to engage with offered resources.
This study is, to the authors' knowledge, the first to specifically compare interest in assistance and predictors of engagement across 2 distinct modalities (in-person vs. guided online assistance). Expanding a prior study by Gruß et al examining concordance between endorsing social risks and interest in assistance, 13 we additionally assessed whether participants screening positive for social risks were already receiving assistance, and the association of each of these conditions with subsequent engagement. The authors found that although, as in prior study, less than half of participants engaged with offered social care, 1 –12,25 more participants randomized to guided self-navigation followed up with assistance compared with those given information for in-person assistance.
A few reasons may explain this differential uptake beyond participant-level differences. First, this study came from a larger RCT that randomized participants to self-navigation and in-person assistance study arms. Although participants in both arms received treatment information in similar ways, study protocols may have prompted differential uptake. 26 Second, logging into a website for self-navigation may have been perceived as easier or more approachable compared with in-person assistance, where interaction with a live person may require more buy-in before individuals are willing to follow up.
Others have noted that patient interest in assistance is likely shaped by experiences with health care and social services, including experiences of trust, discrimination, and receiving help. 25,26 Although only a small percentage of individuals engaged with in-person social care assistance, more of that group followed up with recommended resources compared with those who engaged in guided self-navigation. It may have been that trust was built up in these interactions enough and/or recommendations felt personally tailored enough to then prompt individuals to seek out recommended resources.
The authors found demographic and clinical differences in the likelihood of engaging with offered assistance. Specifically, females and those not in the workforce were more likely to engage with offered assistance, which may be due to a number of reasons including degree of financial need. Women of nearly all races and ethnicities face higher rates of poverty than their male counterparts, a gap that widens for women of ages 18–44 and 75+ years. Many factors explain this disparity, including the gender–wage and wealth gap, occupational segregation between low- and high-paying jobs, and lack of supportive work–family policies. 27
Prior study has also shown that competing priorities and lack of time are often barriers to engagement with offered assistance, 1 and those out of the work force—due to retirement, disability status, or unemployment—may have had more flexibility to follow up with offered resources. Although future study is needed, this finding that those already using assistance for medications and blood glucose supplies were more likely to engage with offered resources suggests that participants found assistance programs they were already using helpful but that they were insufficient to fully meet their needs in these areas.
Consistent with prior study, 4–5,13 the authors found that a substantial proportion of participants screening negative for various social risks still were interested in assistance for those domains, supporting earlier inferences that some patients have unmet needs not reliably identified with social risk screening. The finding that those who did not screen positive for food insecurity but wanted assistance with food and meals were more likely to engage with offered resources supports both that participants had unmet food needs despite screening negative for food-related social risks and that expressing interest in food and meal assistance was associated with being able to overcome potential barriers to engagement. Collectively, these findings have implications for whether individuals in clinical settings should be universally offered social care resources regardless of whether they endorse specific social risks.
There are limitations to this study that should be noted. The sample came from an ongoing RCT, and social care assistance was offered as part of interventions being tested in that study. As a result, the estimates of social care engagement may be overestimated. However, the estimates do align with other studies. 25 Data were self-report and may reflect social desirability bias. This study is based on surveys of patients with diabetes originally identified from a health system in 1 state (Michigan), therefore, findings may not generalize to other states or settings.
Despite these limitations, the results have important implications for practice and research. Some demographic and clinical characteristics such as gender and employment, and general interest in assistance, may provide indication of subsequent engagement with offered assistance. However, patient characteristics alone likely will not provide sufficient information to inform how best to tailor interventions serving diverse patient populations given the nuanced factors impacting uptake of social care assistance. More research and practice investments are needed to understand what factors beyond patient characteristics can be leveraged to support uptake of offered assistance to address unmet social needs.
Conclusion
Gaps are evident in understanding what demographic, clinical, and psychosocial factors are associated with interest in and engagement with offered social care assistance. Although few demographic and clinical factors predicted uptake, interest in assistance both among patients already using assistance for certain needs and among those screening negative for corresponding social risks underscores the complexity of identifying and addressing social risks and needs. More research and practice investments are needed to understand what factors beyond patient characteristics can be leveraged to support uptake of offered assistance to address unmet social needs.
Footnotes
Acknowledgments
The authors are grateful to study staff and participants who made this study possible.
Authors' Contributions
Dr. Patel contributed to conceptualization (equal), writing—original draft (equal), formal analysis (lead), and writing—review and editing (equal). Ms. Smith was engaged in formal analysis (equal) and writing—review and editing (equal). Ms. Torby carried out writing—review and editing (equal). Ms. Isaacson was involved in writing—review and editing (equal). Dr. Cohen took care of conceptualization (equal), writing—original draft (equal), and writing—review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Robert Wood Johnson Foundation through the Social Interventions Evaluation Research Network grantee program, National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health (R01 DK116715-01A1) (P30DK092926) (Michigan Center for Diabetes and Translational Research), and the Department of Veterans Affairs, Health Services Research and Development (CDA 20-037).