
Abstract
In the United States, many individuals with diabetes mellitus (DM) do not achieve treatment goals despite the availability of effective interventions. Provider clinical inertia is one cause of these unfavorable outcomes. Targeted automatic eConsults (TACos) are an emerging technology-based intervention with potential to address clinical inertia in primary care (PC). TACos prospectively identify at-risk patients and use unsolicited specialist recommendations to prompt treatment intensification. Through a payer–provider collaboration, a TACos intervention was piloted for adults with uncontrolled DM (HbA1c >8%) to understand impact on DM clinical inertia and outcomes. Clinical inertia was assessed by measuring whether a PC provider implemented recommended therapeutic changes. Six-month changes in HbA1c and health care costs per member per month were evaluated using an observational matched design and intention-to-treat (ITT) analysis. The analysis included 196 individuals who received a TACos between February 2021 and August 2021 (ITT group) matched to 392 controls based on clinical and demographic criteria. TACos recommendations were implemented 65% of the time. Median percent change in HbA1c was significantly greater for the ITT group versus controls (−10.9% vs. −10.2%; P = 0.0359). Median total costs were 7.9% lower in the ITT group (P = 0.0900). A per protocol analysis was done to examine effects between ITT group individuals with an implemented TACos recommendation (n = 126) and controls. Median percent change in HbA1c was significantly greater (−19.5% vs. −10.2%; P < 0.0001), but there was no difference in total costs (−7.9%; P = 0.1753). TACos may feasibly address clinical inertia in PC and improve HbA1c for uncontrolled DM.
Introduction
Improving outcomes for diabetes mellitus (DM) is a priority for health care systems and payers given its high prevalence and cost. More than 11% of the US population is living with DM and an estimated 25% of health care spending is directed toward its treatment and management. 1,2 A high proportion of these costs are likely attributable to individuals with uncontrolled DM, 3 –5 who use more health care services and experience greater rates of associated complications and comorbidities than those with glycemic control. 6 –8
A multitude of recommended evidence-based practices are available to support achievement of glycemic control, such as team-based care, promotion of self-management behaviors, and timely treatment intensification with glucose-lowering therapies. 9 These practices can also lower health care costs and prevent or delay DM complications and comorbidities. 10 –12 However, prior research has shown that <75% of individuals with diagnosed DM achieve recommended glycemic levels and that <25% achieve control for blood glucose, blood pressure, and lipid levels. 13 Clinical inertia (ie, provider failure to use available evidence-based interventions or intensify therapy when warranted) is 1 contributing factor to suboptimal DM outcomes 14 and a prevalent and persistent cause of poor outcomes in primary care settings, 15,16 where most outpatient DM care is focused. 17,18
Electronic consultations (eConsults) are an asynchronous efficient provider-to-provider telehealth modality that may mitigate clinical inertia by providing specialist decision support within primary care settings and enhancing patient–provider shared decision making. 19,20 eConsults may be particularly beneficial for geographic areas where disparities in specialist care access are prevalent 21,22 or where primary care providers (PCPs) are overburdened. 23 Targeted automatic eConsults (TACos) are an emerging data-driven eConsult variant that prospectively identify affected patients using electronic health record (EHR) data. 24,25 Data visualization tools (eg, data dashboards) and medical records provide pertinent clinical information to specialists who then communicate unsolicited treatment recommendations to PCPs through an EHR.
At present, TACos interventions have not been thoroughly investigated: to the authors' knowledge, only 1 study has examined their impact on DM outcomes. 26 Oseran et al found that a TACos intervention increased prescribing of glucose-lowering medications by PCPs, but there was no significant reduction in 6-, 12-, or 18-month HbA1c for individuals with uncontrolled type 2 DM (T2DM) relative to a control group. 26
Although further research is necessary to understand the effectiveness of TACos interventions, such tools are likely to be of continued interest to health care organizations—especially as, pursuant to the COVID-19 pandemic, many have significantly expanded capacity to support telehealth models 27 and refocused efforts to advance key health care aims such as value-based care and health equity. 28,29 In this study, the authors report on the 6-month clinical and cost impacts of an endocrine TACos program for individuals with uncontrolled DM piloted as part of a payer–provider collaboration within a large integrated delivery and finance system (IDFS).
Materials and Methods
Setting and population
The endocrine TACos program was designed and implemented at UPMC, a large IDFS headquartered in Pittsburgh, Pennsylvania (PA). UPMC's provider system includes 40 hospitals and >800 primary care and specialty clinic sites that provide health care services to residents of PA and nearby regions. UPMC Health Plan (HPLAN) provides health care benefits for 4.5 million individuals through Medicare Advantage, Special Needs Plans, Medicaid, and private individual and employer-sponsored plans (commercial plans). The TACos program is available to UPMC-owned primary care practices located principally in rural and urban areas of Western PA. The population for this evaluation included HPLAN beneficiaries with uncontrolled (HbA1c >8%) type 1 DM (T1DM) and T2DM who had no endocrinologist visits within the past year.
Intervention
The TACos program is managed by a single endocrinologist based out of an urban academic endocrinology clinic operated by UPMC. The endocrinologist contributes a small portion of their clinical time to the TACos program, which is supported by HPLAN. Care management and administrative support is provided by a HPLAN-employed nurse practitioner (NP) who is also a certified diabetes care and education specialist. The UPMC endocrinologist and NP are not physically colocated and coordinate member care through telecommunication (eg, video conferencing, secure electronic messaging). Before implementing the TACos program, the UPMC Division of Endocrinology and HPLAN obtained approval from PCP leaders to offer the program within UPMC. The TACos program was then introduced to PCP practices at clinical faculty meetings and townhalls. PCP feedback was obtained and their questions or concerns were addressed. PCPs were also alerted by e-mail immediately before the TACos program went live at their practice.
The underlying patient identification algorithm for the endocrine TACos program was developed using a machine learning approach by the UPMC Division of Endocrinology and the UPMC Clinical Analytics department; the latter provides evaluation and analytics support to UPMC's Health Services Division. The algorithm is run each day and uses clinical data sourced from UPMC's EHR to identify adult HPLAN members who have an HbA1c >8% and whose glycemic control is predicted to worsen over time. Predictor variables used in the selection algorithm broadly include sociodemographic characteristics, prior health care utilization, anthropometric and laboratory values, and medical comorbidities.
Once identified, appointment scheduling data are used to select those HPLAN members who have an upcoming appointment with a participating PCP within the next 5 days. The prioritized list of members is then made available to the endocrinologist and NP through a data dashboard. The NP conducts a preliminary review of the member list to confirm HPLAN enrollment, identify those who are not currently under the care of an endocrinologist, and assess treatment needs. The NP then provides the endocrinologist with a final member list through UPMC's EHR. The endocrinologist reviews NP input and member medical records and then prepares the TACos, which are sent to a member's PCP 1 day before their scheduled appointment. PCPs receive an alert within the EHR to review the TACos and discuss treatment recommendations with their patients.
Evaluation Design and Measures
Medical records within the UPMC EHR were reviewed to assess whether a TACos recommendation was implemented by a PCP, the type and frequency of treatment recommendations made by the consulting endocrinologist, and reasons why recommendations were not implemented by the PCP. An observational matched design was used to compare clinical and cost outcomes between HPLAN members who received a TACos between February 2021 and August 2021 and a control group of HPLAN members with uncontrolled DM. HPLAN members were considered for matching if they had a non-UPMC PCP visit between February 2021 and August 2021 and no endocrinologist visits in the year before the PCP visit.
Intent-to-treat (ITT) methodology was used to examine outcomes for all members with a TACos (ITT group) versus the control group. A per protocol analysis was done to examine effects for those HPLAN members in the ITT group who had a TACos recommendation implemented by the PCP (per protocol group) versus the control group. In other words, the per protocol analysis excluded HPLAN members who did not have a TACos recommendation implemented by the PCP. For both the ITT analysis and per protocol analysis, outcomes assessed over 6 months included repeat HbA1c values ≥60 days after baseline HbA1c, percent change in HbA1c ([repeat HbA1c − baseline HbA1c]/baseline HbA1c × 100), total cost of care per member per month (PMPM), medical cost PMPM, and pharmacy cost PMPM.
Member characteristics for descriptive analyses included DM type, age, sex, race, insurance type, baseline HbA1c, number of days between baseline and repeat HbA1c tests, baseline insulin status, socioeconomic status based on Area Deprivation Index (ADI) score, 30 comorbidity load/mortality risk based on Charlson Comorbidity Index (CCI) score, 31 diagnosis of coronary artery disease (CAD), diagnosis of congestive heart failure (CHF), emergency department (ED) utilization per 1000 six months before the index visit, and medical cost 6 months before an index visit. Member characteristics, HbA1c, and cost data were sourced from the HPLAN Insurance Data Warehouse, which captures all administrative data and claims submissions for HPLAN members.
Statistical analysis
The intervention and control groups were matched using 2:1 greedy nearest neighbor propensity score matching 32,33 on the following criteria: HbA1c category (7.8 ≤ HbA1c ≤ 9, 9.1 ≤ HbA1c ≤ 11, 11.1 ≤ HbA1c ≤ 13, HbA1c > 13); primary care visit date; number of days between baseline and repeat HbA1c tests; age (<60 years, ≥60 years); sex (female, male); race (White, non-White); insurance plan type (commercial, Medicare Advantage/Special Needs Plan, Medicaid); socioeconomic status (ADI score <100, ≥110); comorbidity level/mortality risk (CCI score <3, ≥3); CAD (yes/no); CHF (yes/no); ED utilization per 1000 in previous 6 months; and medical cost in previous 6 months.
HbA1c category was weighted with a value of 3 and all other variables were weighted with a value of 1. Statistical comparisons of member characteristics and HbA1c and cost outcomes for ITT group versus the control group and per protocol group versus the control group included 2-sided Wilcoxon signed-rank tests for non-normally distributed data and chi-square tests of proportions. For proprietary reasons, 6-month cost outcomes are presented as percent difference in median cost. Analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
Ethics approval
This study was reviewed by UPMC Quality Improvement Review Committee (Project ID: 3459) and was determined to be an organizational quality improvement initiative and not human subject research; thus, oversight by an institutional review board was not required.
Results
The analytic sample included 588 members in total: 196 members with DM in the intervention ITT group were matched to 392 individuals in the control group (Figs. 1 and 2). Of an initial 275 members with a TACos, 28 were excluded for the following reasons: no HPLAN insurance (n = 8), HPLAN was not the primary insurer for medical and pharmacy expenses (n = 6), had <6 months of post-TACos follow-up time (n = 2), or lacked a recorded baseline HbA1c measure (n = 12). Of the remaining 247 members, 51 were unable to be matched to controls for a final ITT group analytic sample of 196 members. Of 91,822 individuals with DM who had at least 1 primary care visit with non-UPMC owned primary care practices, 6308 were eligible for matching.
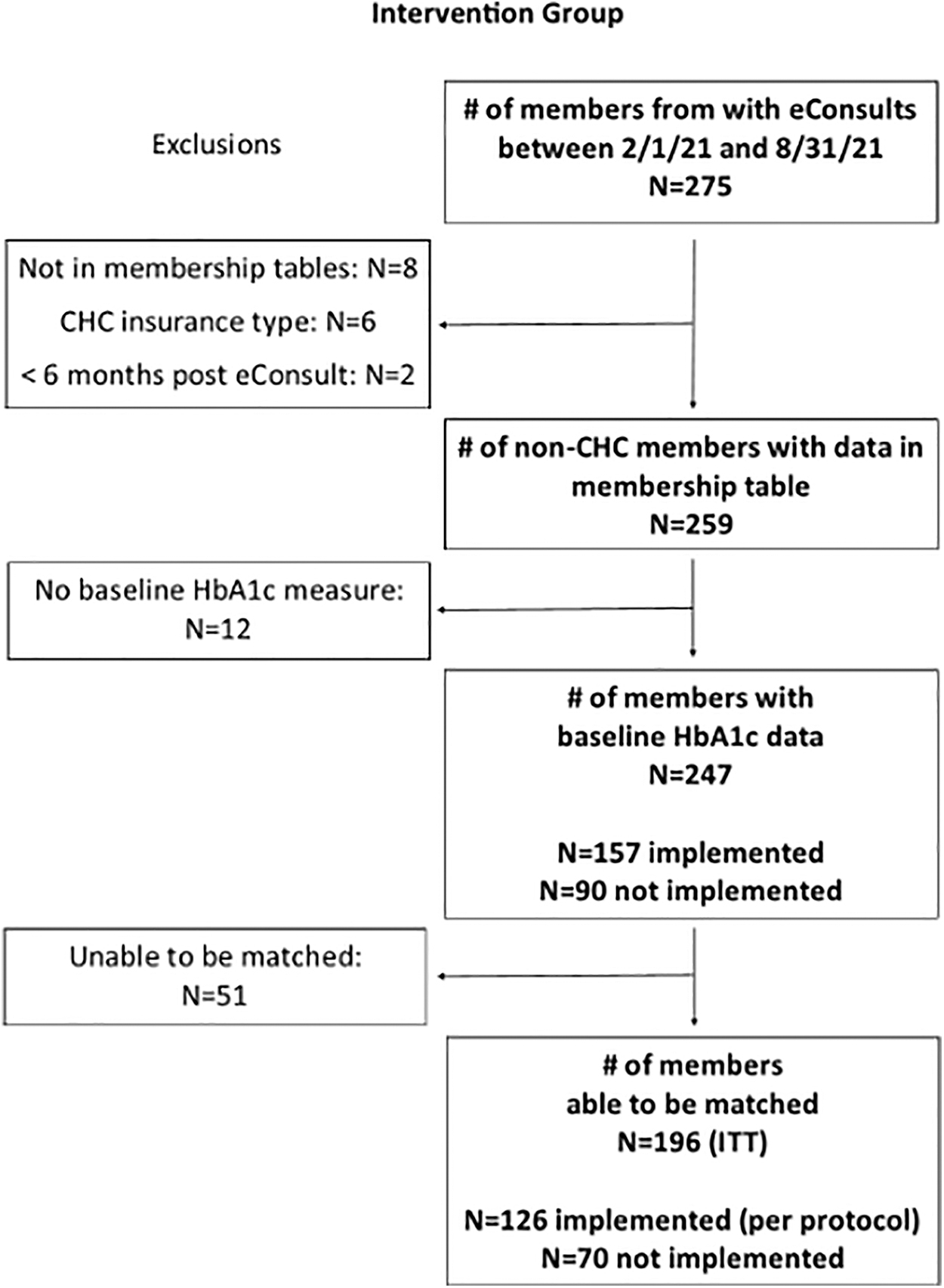
CONSORT for intervention groups. CHC, Community Health Choices; ITT, intention-to-treat.
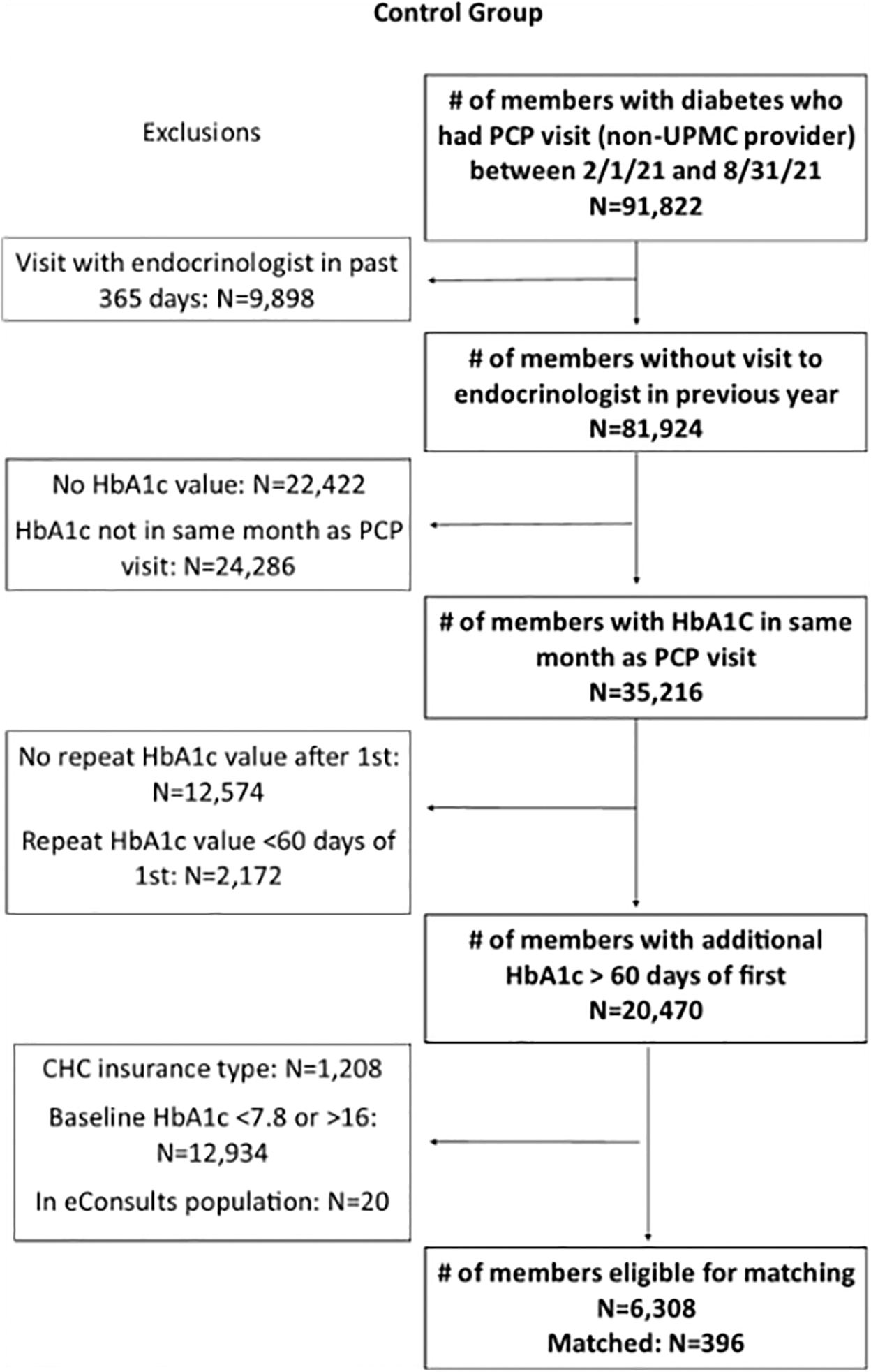
CONSORT for control group. PCPs, primary care providers.
A total of 85,514 were excluded from the matching pool for the following reasons: had an endocrinologist visit within 365 days from their index primary care visit (n = 9898), no recorded baseline HbA1c (n = 22,422), baseline HbA1c outside of the month of their primary care visit (n = 24,286), no recorded follow-up HbA1c measure (n = 12,574), or follow-up HbA1c measure taken within 60 days of the baseline measure (n = 2172), HPLAN was not the primary insurer for medical and pharmacy expenses (n = 1208), had a baseline HbA1c that was <7.8% or >16% (n = 12,934), or were already included in the intervention group (ie, likely changed PCPs during the evaluation period) (n = 20).
After matching, some differences in member characteristics between intervention groups and the control group remained (Table 1). Compared with control group members (N = 392), intervention ITT members (N = 196) and intervention per protocol members (N = 126) had higher baseline HbA1C, were more likely to be taking insulin at baseline, and were less likely to live in disadvantaged neighborhoods (ADI score ≥110) (all P < 0.10). Intervention ITT members were more likely to be in a HPLAN commercial insurance plan compared with members in the control group.
Baseline Characteristics of the Treatment and Control Groups
ADI, Area Deprivation Index; CCI, Charlson Comorbidity Index; ED, emergency department; IQR, interquartile range; ITT, intention-to-treat; SD, standard deviation.
Overall, 65% of TACos therapeutic recommendations were implemented by PCPs. The most common therapeutic recommendations made by the endocrinologist were intensification with glucagon-like peptide 1 (GLP-1) agonist (36%), intensification with a sodium/glucose cotransporter-2 inhibitor (SGLT2i) (18%), intensification with insulin (10%), insulin regimen adjustment (16%), and use of a continuous glucose monitor (16%). All TACos included a referral to a certified diabetes care and education specialist and lifestyle and chronic condition management health coaching services provided by HPLAN. Where a TACos therapeutic recommendation was not implemented (35% of TACos), reasons included the HPLAN member declining the treatment change (55%), member nonattendance to a scheduled primary care appointment (30%), the PCP not discussing the TACos recommendation with their patient (10%), and a change in member circumstances that rendered the TACos recommendation irrelevant (5%).
HbA1c at baseline was significantly higher for both intervention ITT group (9.7%) and intervention per protocol group (9.8%) versus control (9.0%) (both P < 0.0001) (Fig. 3). Median HbA1c 6 months after TACos was significantly higher in intervention ITT group versus control (8.4% vs. 8.0%; P = 0.0258) but significantly lower in intervention per protocol group versus control (7.8% vs. 8.0%; P = 0.0409) (Fig. 3). Median percent change in HbA1c was slightly greater for intervention ITT group versus control (−10.9% vs. −10.2%; P = 0.0359), and greater for the intervention per protocol group versus control (−19.5% vs. −10.2%; P < 0.0001) (Fig. 4).
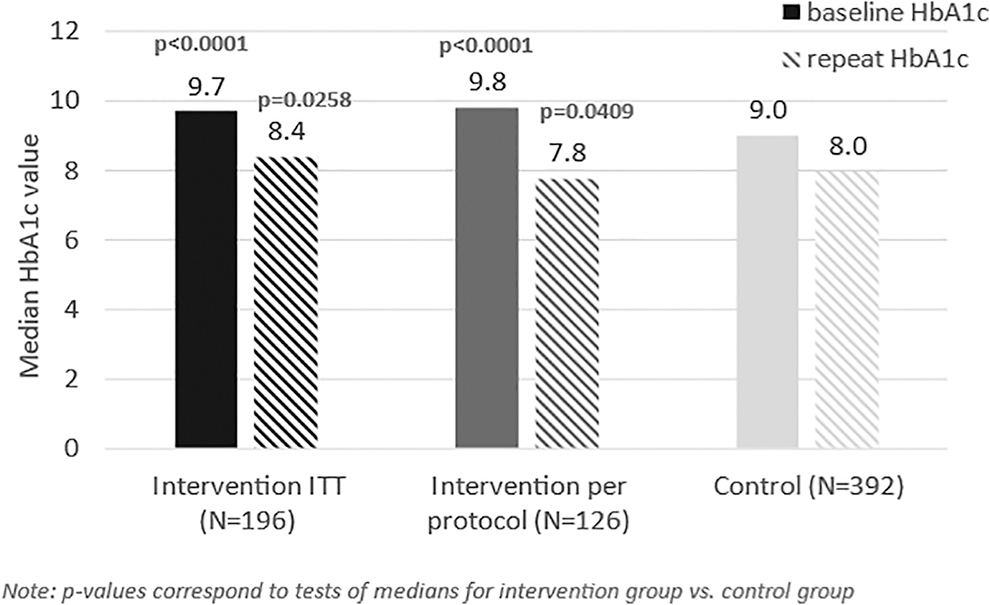
Median baseline and repeat HbA1c values for intervention groups versus control group.
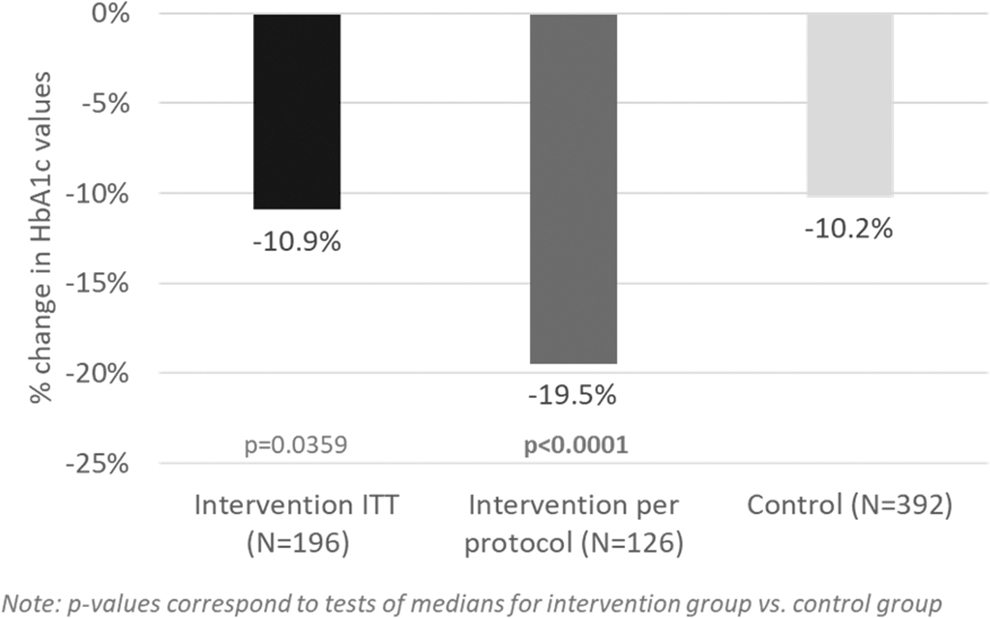
Median percent change between repeat and baseline HbA1c for intervention groups versus control group.
Median total, medical, and pharmacy costs in the 6 months after TACos were compared between intervention groups (ITT group and per protocol group) and the control group, with results presented as a percent difference relative to the control group (Fig. 5). Compared with control group members, intervention ITT members had 7.9% lower median total cost PMPM in the 6 months after TACos; this difference was marginally significant (P = 0.0900). The difference in total costs was driven by a lower median medical cost PMPM (−22.8%; P = 0.0242). Median pharmacy cost PMPM was 15.3% higher in the ITT group, but this difference was not statistically significant (P = 0.3130).
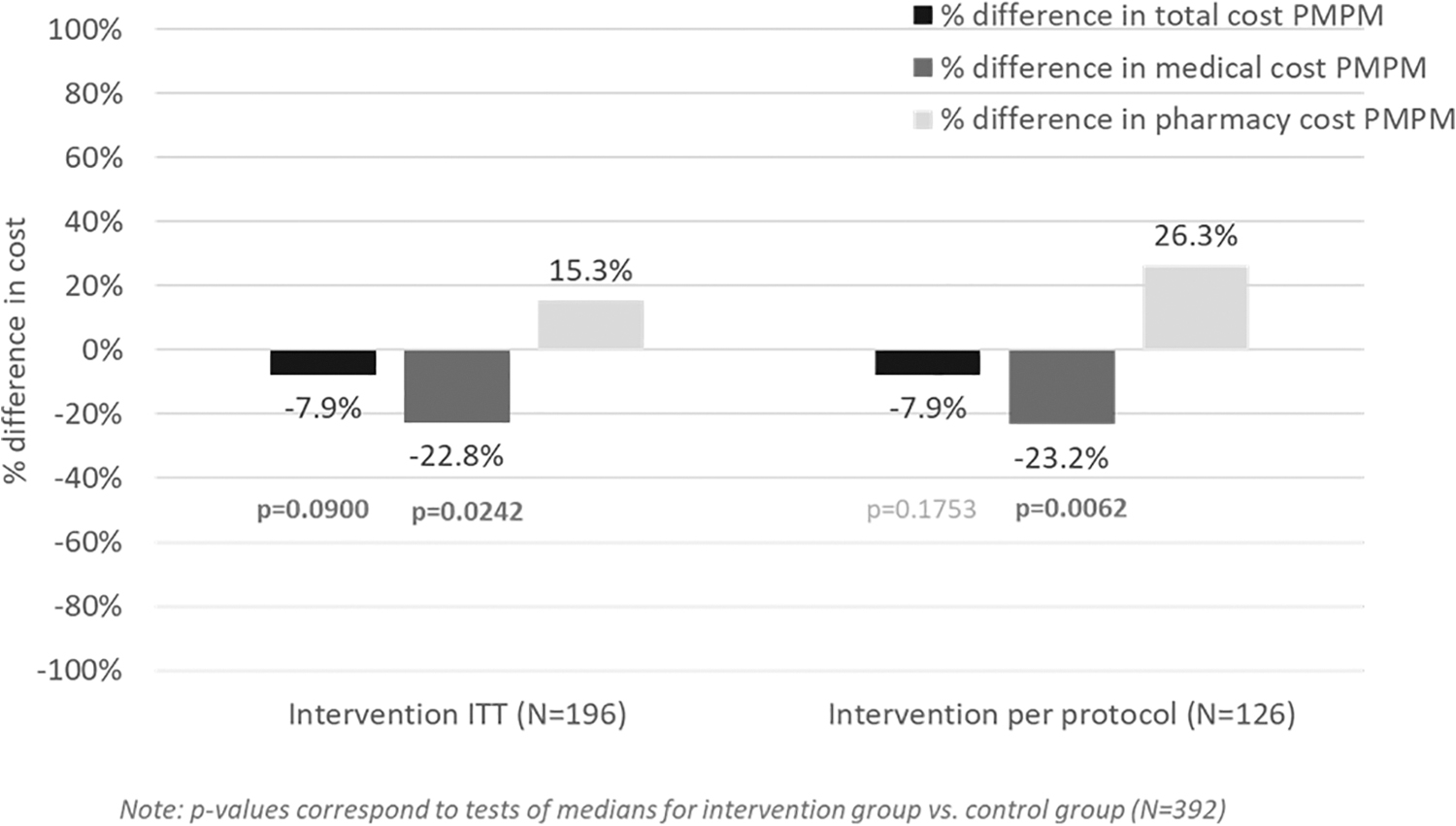
Percent difference in 6-month cost outcomes for intervention groups versus control group.
For the per protocol analysis, median total cost PMPM in the 6 months after TACos was lower for the intervention per protocol group compared with the control group, but this difference was not statistically significant (−7.9%; P = 0.1753). The total cost PMPM difference was driven by lower medical cost PMPM (−23.2%; P = 0.0062). PMPM pharmacy costs were significantly higher in the per protocol group relative to the control group (26.3%; P = 0.0104).
Discussion
Findings from this evaluation demonstrate that an endocrine TACos program can be a feasible mechanism for communicating specialist treatment recommendations to PCPs and a viable tactic for overcoming clinical inertia in a primary care setting. In addition, results indicate that a TACos intervention has potential for improving glycemic control in populations with uncontrolled DM.
PCPs implemented 65% of unsolicited specialist therapeutic recommendations, which is comparable with rates reported for solicited endocrinology eConsults. 34 Although a comparison of prescribing patterns between intervention and control groups and member medication adherence was outside of the scope of this pilot evaluation, ITT and per protocol analyses showed that 6-month pharmacy spending was higher in both intervention groups (ITT group and per protocol group) relative to the control group. Higher pharmacy spending was expected if the consulting endocrinologist recommended therapy adjustments with more expensive glucose-lowering medications, 35 which was observed in this evaluation.
A clinically meaningful HbA1c reduction was observed in both intervention groups and control groups; however, the relative change in HbA1c was greater for both the ITT group and per protocol group. In addition, the magnitude of HbA1c reduction in the per protocol group (ie, the group where PCPs implemented TACos recommendations) was nearly 2-fold that of the intervention ITT group and control group. Taken together, these findings suggest that TACos facilitated more intensive therapeutic management.
In a prior study, Oseran et al reported a nonsignificant difference in follow-up HbA1c for a similar TACos model. 26 The authors posited that this null finding was due to low adoption of endocrinologist treatment recommendations by providers (38% of recommendations were adopted). 26 Lack of familiarity, technical challenges, and workload concerns are known barriers to PCP adoption of eConsult services. 36 The timing of TACos may be 1 reason a higher adoption rate was observed in this evaluation.
Specialist recommendations were sent 1 day before a PCP met with a patient during an already scheduled appointment, which negated the need for additional patient outreach and minimized PCP burden. The efforts of the consulting endocrinologist to familiarize PCPs with the TACos intervention before implementation may be another contributing factor. Also, PCPs within UPMC health care system are incentivized through value-based care arrangements with HPLAN to achieve quality and cost performance targets for their DM populations. Although this arrangement does not provide direct incentives for using the TACos program, it may have indirectly influenced program acceptance.
Refusal of treatment change by HPLAN members was the leading cause of nonadoption of TACos recommendations in this evaluation (55%), followed by missed primary care appointments (30%). Factors contributing to patient reluctance to start or intensify DM therapy have been well documented, 14,37 and primary care nonattendance has been associated with poor glycemic control, disruptions to care continuity, and economic/psychosocial factors. 38 Coupling TACos to interventions that address patient-level treatment concerns or barriers may be 1 approach for improving adoption of specialist recommendations and, subsequently, population-level outcomes.
A novel aspect of this evaluation was the assessment of short-term economic impact of the TACos program on total cost of care through analysis of insurance claims. Cost outcomes for eConsults have not been extensively described, 39 and, based on review of the published literature, not yet examined for TACos interventions in populations with DM. Total cost PMPM was lower in both intervention groups (ITT group and per protocol group) relative to the control group, although this difference was only marginally significant for the ITT group and not significant for the per protocol group. For both intervention groups, significantly lower medical spending relative to the control group was by higher pharmacy spending.
The observed lower medical spending is consistent with outcomes reported in a systematic review in which eConsults lowered costs by replacing more expensive in-person specialty care visits, reducing the use of diagnostic tests, and lowering risk of ED admissions. 40 However, a more nuanced analysis of prescribing patterns could provide further insight for the observed pharmacy cost outcomes. Likewise, an analysis of specific medical utilization categories for a longer period of time to allow for a sufficient number of events would elucidate reasons for lower medical spending. The current observation period may be too short to observe significant cost differences across groups that could occur from a sustained decrease in medical utilization, even with increased pharmacy cost and utilization. Prior studies have shown cost savings from improved glycemic control can be achieved for 1- to 2-year periods. 10
This evaluation is not without limitations. The endocrine TACos program was implemented as a quality improvement initiative and a design that was efficient and not cost-prohibitive was selected for the evaluation. Therefore, results from this observational evaluation must be interpreted with caution given differences in baseline demographic and clinical characteristics between intervention and control groups. Although steps were taken to address these differences, they could not be fully resolved. The potential for selection bias also limits interpretation of results. The TACos program was available only to UPMC-owned primary care practices, whereas controls were selected from a population that was managed by non-UPMC PCPs to avoid treatment contamination. Practice patterns and provider characteristics may be different between UPMC-owned and nonowned practices.
In addition, HPLAN members in the intervention group were identified differently than those in the control group. Cost outcomes do not reflect all intervention costs as only billed claims paid by the HPLAN were used for cost estimates and these did not account for program costs (eg, endocrinologist salary). In addition, the 6-month observation period did not allow for a sufficient number of events to occur to determine reasons for lower medical spending by specific service categories. Inaccurate coding and other errors inherent within administrative claims and EHR data may also have influenced results. Finally, this evaluation was conducted in the context of a large integrated delivery system and included a population managed by a single payer; findings may not be generalizable to other health care settings or organizations.
Potential future directions for the described TACos program include assessment of long-term DM, cost, and utilization outcomes, assessment of other clinical outcomes important to DM management (eg, weight change, lipid and blood pressure control), the use of experimental designs to address limitations of the current analysis, exploration of barriers and facilitators to adoption of endocrinologist recommendations by HPLAN members, and an examination of outcome differences across sociodemographic groups.
Conclusions
PCPs were receptive to an endocrine TACos intervention implemented to support DM management and accepted most unsolicited therapeutic adjustments recommended by a consulting endocrinologist. A greater relative decrease in HbA1c was observed at 6 months for the intervention group compared with a control group. Medical cost at 6 months was also lower, but pharmacy costs were higher. There was a marginally significant difference for total cost of care. PCPs were receptive to treatment recommendations made by the consulting endocrinologist, but results suggest a need to address patient-related factors that may inhibit treatment intensification or acceptance of other specialist recommendations.
TACos interventions are an attractive tool for population health management as they enable rapid identification of high-risk patients, efficient use of specialist resources, and can scale across broad geographies. Findings from this evaluation show that TACos have potential for addressing key challenges in DM care by improving patient access to endocrinology services and timely treatment, supporting PCP decision-making, and facilitating the use of recommended evidence-based practices. Further research is necessary to understand the effects of TACos on clinical and economic outcomes across diverse population groups for longer time periods.
Footnotes
Acknowledgments
The authors wish to acknowledge the contributions of Oscar Marroquin, MD, FACC and the UPMC Clinical Analytics Department for the development of clinical analytic tools and methods used within their intervention.
Authors' Contributions
Conceptualization, investigation, methodology, supervision, project administration, and writing—review and editing by Dr. French and Dr. Beckjord. Writing—original draft and writing—review and editing by Mr Kanter and Dr. Williams. Methodology, formal analysis, visualization, writing—original draft, and writing—review and editing by Dr. Winger. Project administration and writing—review and editing by Ms Grumski. Conceptualization, investigation, supervision, and writing—review and editing by Dr Schuster.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This evaluation was not supported by external grant funding. All authors are paid employees of UPMC.