
Abstract
Social needs, such as social isolation and food insecurity, are important individual-level social determinants of health, especially for adults ages 65 years and older. These needs may be associated with future health care utilization, but this research area has not been studied extensively. The objective of this study was to examine the independent association of 5 individual social needs with future (1) emergency department (ED) visits and (2) hospital admissions. This observational study included 9649 Kaiser Permanente Northwest (KPNW) Medicare members who completed the Medicare Total Health Assessment (MTHA) quality improvement survey between August 17, 2020 and January 31, 2022. The 5 social needs assessed by the MTHA, defined as binary measures (yes/no), included (1) financial strain, (2) food insecurity, (3) housing instability, (4) social isolation, and (5) transportation needs. ED utilization (yes/no) and hospitalization (yes/no), the current study outcome measures, were measured in the 12 months after MTHA assessment. In multivariable analyses, 3 of the 5 social needs were significantly associated with higher ED utilization: financial strain (odds ratio [OR] = 1.40, 95% confidence interval [CI] = 1.11–1.76, P < 0.05), housing instability (OR = 1.43, 95% CI = 1.02–1.99, P < 0.05), and social isolation (OR = 1.19, 95% CI = 1.05–1.34, P < 0.05), and 1, financial strain, was significantly associated with hospital admissions (OR = 1.66, 95% CI = 1.23–2.23, P < 0.05). The study results identified which social needs are most strongly associated with future ED utilization and hospital admissions. Further research is needed to better understand whether addressing social needs is associated with improved patient-level health outcomes over time.
Introduction
Social needs such as financial strain, food insecurity, social isolation, and housing instability are associated with poor health outcomes and increased use of health care services among older adults. 1 –8 The increased prevalence of social isolation during the COVID-19 pandemic highlighted the importance of identifying and addressing social needs, specifically within the population ages 65 years and over. 9 –11
Previous research has found that individuals ages 65 years and older experience high levels of social needs. For example, recent estimates suggest that ∼25% of older adults in the United States experience social isolation and loneliness, 9 ∼1 in 10 experience food insecurity, 12 and 5%–7% experience financial strain. 13 Furthermore, a significant proportion of older adults experience hospital admissions and emergency department (ED) visits that are considered avoidable, and that may be influenced by nonmedical reasons. 14 Investigating the association between social needs and health care utilization among adults ages 65 years and over may provide support to national efforts by hospitals and health systems to improve health equity among patients by working to address social needs.
Despite limited evidence showing that having social needs is associated with higher health care utilization, 15 –17 few studies have examined which needs are most important, specifically on a population level. Thus, the primary goal of this study is to examine which individual social needs have the strongest association with health care utilization (when analyzed together) for adults ages 65 years and older.
Materials and Methods
This retrospective cohort study included data from 9649 Medicare Advantage enrollees (ages 65 years or older) who were also members of Kaiser Permanente Northwest (KPNW), an integrated health system in Oregon and southwest Washington. Patients were included if they completed an operations-based survey, the Medicare Total Health Assessment (MTHA), and were ages 65 years and over (as of survey date) between August 17, 2020 and January 31, 2022.
Included patients also met 4 other criteria: (1) completed assessments for 5 social needs, including financial strain, food insecurity, housing needs, social isolation, and transportation needs; (2) had 12 or more months of continuous health plan enrollment before and after the survey index date; (3) had nonmissing information for social needs and covariate measures; and (4) were not on KPNW's research exclusion list. Survey data from the MTHA are located in the Research Data Warehouse (RDW) housed at the Kaiser Permanente Center for Health Research (CHR). The RDW is a curated clinical database that has been used for over 25 years to facilitate health services research. 18
The MTHA has been described in detail previously. 19,20 In brief, the purpose of the MTHA is to assess required and optional domains, as mandated by the Centers for Medicare & Medicaid Services (CMS), for annual wellness visits among Medicare beneficiaries. During the annual wellness visits, Medicare beneficiaries and health providers develop a collaborative care plan to address physical and mental health needs. 15,21,22 Although CMS does not require assessments of social determinants of health during these visits, KPNW screened for 5 social needs using the MTHA during the study period.
Patients were eligible for the MTHA survey if they had a scheduled Medicare Wellness Visit (MWV), and surveys were conducted by 1 of 2 methods: (1) at the time of MWV or (2) before the MWV (using electronic email administration or interactive voice recognitive technologies). The MTHA has been used in several published studies to examine social health needs in older populations.
These studies included (1) determining the prevalence of food insecurity in the ages 65 years and over population, 20 (2) examining the association between social isolation and health care utilization/health outcomes, 15,23,24 and (3) examining the association between food insecurity and falls. 19 For patients who completed >1 MTHA in the study time period, the first MTHA was used as the index date for all analyses. This study was approved by the KPNW Institutional Review Board.
Conceptual model
This study used the Andersen Behavior Model of Health Services Use as a conceptual model to inform the analysis (Fig. 1). 25 –28 This model has been used to conduct policy-relevant research examining factors associated with health care utilization over the past 25 years. 27 –31 In this iteration of the model, the authors posit that future health care utilization is a function of environment, predisposing, enabling, and need-for-care characteristics, and that the presence of social needs is an enabling characteristic of future health care utilization.
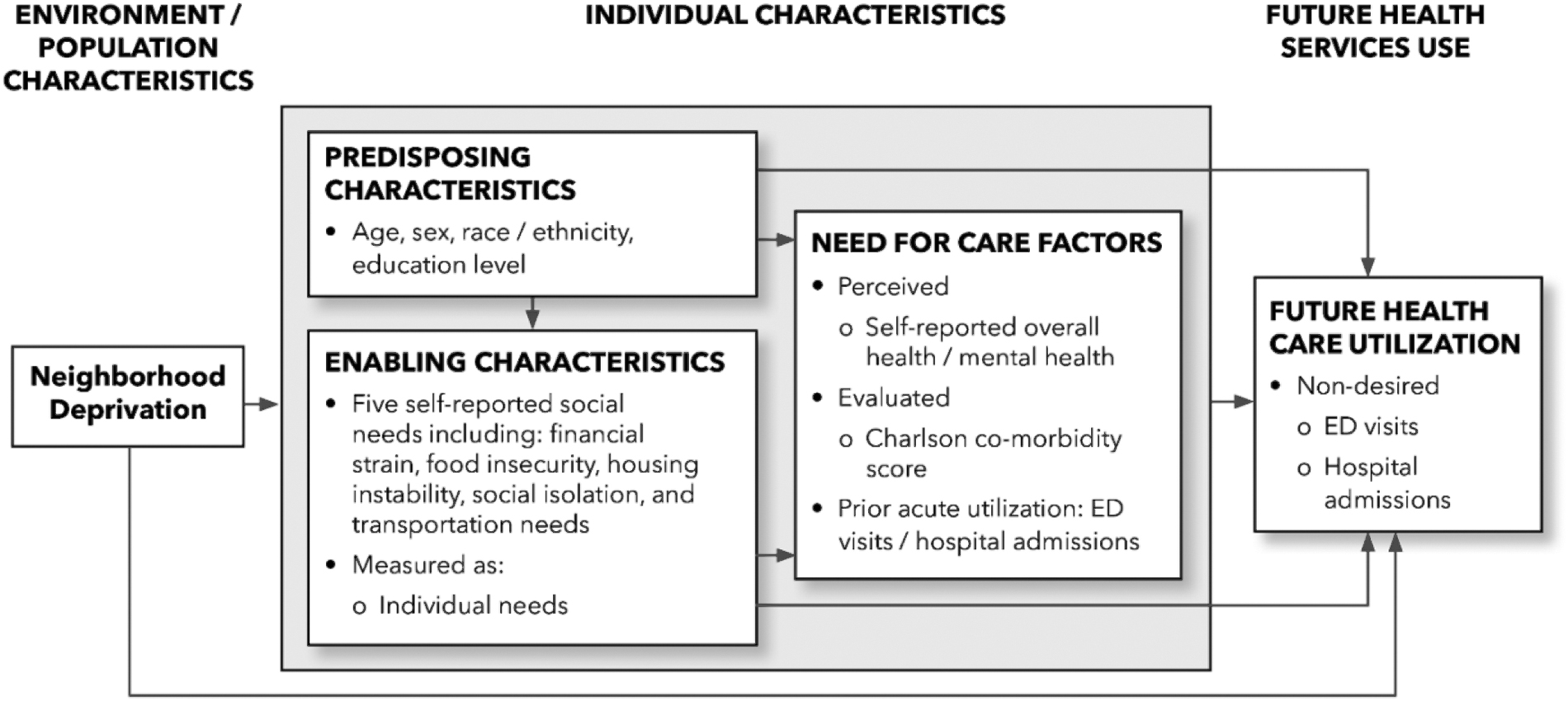
Andersen behavioral model of health care utilization.
Outcome measures
ED visits and hospital admissions were the 2 outcome measures for this analysis. Both were measured in the 12 months after the MTHA survey index date and extracted from the CHR RDW.
Independent variables
The presence of social needs was the primary independent variable in the analysis. This measure was analyzed as 5 individual binary social need items (yes/no) assessed during the index MTHA survey: (1) financial strain, (2) food insecurity, (3) housing instability, (4) transportation needs, and (5) social isolation. This analysis focused on patients' responses to questions about the presence of these social needs, irrespective of whether patients reported wanting assistance with these needs.
For example, individuals whose answers indicated that they had food insecurity were included regardless of whether the patients indicated that they wanted food assistance. These measures were selected from established measures of social needs identified in the peer-reviewed literature. 32 –39 A complete description of these measures is provided in Table 1. The exact survey questions are provided in Supplementary Appendix S1.
Description of Social Needs Measures
Covariate measures
This study included the neighborhood deprivation index (NDI) as an environment characteristic. 40 This is a neighborhood-based socioeconomic measure, derived from census-based information. This measure was extracted from the RDW.
Included predisposing characteristics were age, gender, race/ethnicity, and highest education level completed. Education level was identified through the MTHA, whereas the remaining predisposing covariate measures were identified through KPNW's electronic health record (EHR)—contained in the RDW.
Included need-for-care characteristics were the Charlson Comorbidity Index (CCI), 41,42 self-reported overall health, self-reported mental health, and ED utilization and hospital admissions in the year before index MTHA survey. The CCI and prior utilization metrics were constructed from EHR data located in the RDW; self-reported overall health and mental health were identified from the MTHA.
Analysis
Descriptive analyses
First, the authors conducted descriptive analyses for environment, predisposing, need-for-care, and enabling characteristics among the eligible study population.
Collinearity diagnostics and logistic regression model building
Collinearity diagnostics were used to assess collinearity among each of the independent (enabling) variables and the covariate measures (predisposing, environment, and need-for-care characteristics). Because no collinearity was found, all covariate measures were included in final logistic regression models.
ED utilization (Model 1) and hospital admissions (Model 2) were regressed on the each of the 4 binary social needs variables (financial strain, food insecurity, housing insecurity, social isolation, and transportation needs), with “no” as the reference group for each.
In addition, the team considered age (65–74 [ref. group], 75–84, 85+ years), gender (male [ref. group] vs. female), race/ethnicity (White [ref. group] vs. non-White), highest education level (high school or less [ref. group], some college or 2-year degree, college graduate or beyond), NDI (least deprivation [ref. group], moderate deprivation, highest deprivation), self-reported overall health (good/very good/excellent [ref. group] vs. fair/poor), self-reported mental health (good/very good/excellent [ref. group] vs. fair/poor), CCI (0 [ref. group], 1, 2 or higher), any prior ED utilization in the year before index date (no [ref. group] vs. yes), and any prior hospital admissions in the year before index date (no [ref. group] vs. yes).
Results
Sample characteristics
With respect to predisposing characteristics, ∼65% of the study population were between ages 65 and 74 years, and the average age overall was 73 years (Table 2). Over 55% of patients were female, >90% were White, and >40% reported a college degree or higher. The study population lived in neighborhoods that trended toward lower neighborhood deprivation; the mean NDI score (environment characteristic) was −0.3 ± 0.6 (min = −1.7788, max = 2.9605; lower NDI score means less neighborhood deprivation).
Population Characteristics
CCI, Charlson Comorbidity Index; ED, emergency department; NDI, neighborhood deprivation index; SD, standard deviation.
With respect to need-for-care characteristics, <20% of included patients reported their overall health and mental health as “fair” or “poor.” Indicating comorbidities were common; nearly one third of the population had a CCI score of 2 or higher. Last, a little >15% of the study population had any ED utilization in the year before the MTHA survey, whereas ∼5% had any hospitalization.
Description of social needs
About one third of the study population (33.4%) reported 1 or more social needs (Table 3). The most prevalent social needs (in descending order) were (1) social isolation (26.3%), (2) transportation needs (5.8%), (3) financial strain (5.5%), (4) food insecurity (2.7%), and (5) housing instability (2.1%).
Description of Social Needs (Enabling Characteristics)
Logistic regression results: Association between social needs and ED utilization and hospital admissions
Three social needs were independently associated with ED utilization after adjusting for other social needs and covariate measures: financial strain (odds ratio [OR] = 1.40, 95% confidence interval [CI] = 1.11–1.76), housing instability (OR = 1.43, 95% CI = 1.02–1.99), and social isolation (OR = 1.19, 95% CI = 1.05–1.34). Of the 5 social needs analyzed, only financial strain was independently associated with future hospital admissions (OR = 1.66, 95% CI = 1.23–2.23), adjusting for the same characteristics (Table 4).
Logistic Regression Results: Association of Individual Social Needs with Emergency Department Utilization and Hospital Admissions
Bolded text indicates OR and 95% CIs that are statistically significant at p < .05 level.
Models adjusted for predisposing characteristics: age, gender, race/ethnicity, education level; environment characteristics: NDI; and need factors: self-reported general (overall) health, self-reported mental health, CCI, prior hospital utilization, and prior ED utilization.
CI, confidence interval; OR, odds ratio.
Discussion
In this study of adults ages 65 years and over attending MWVs, ∼1 in 3 reported 1 or more social needs. Three of 5 social needs were associated with future ED utilization: financial strain, housing instability, and social isolation. Only financial strain was independently associated with future hospital admissions.
The current study results are similar to previous research findings. McQueen et al 17 found that increased social needs were associated with increased hospitalizations in a cross-sectional study of Medicaid recipients with diabetes. Another study conducted by Lewis et al 43 found that among an insured population receiving subsidies on the federal health exchange, housing instability was associated with increased ED and urgent care utilization.
Last, Shaw et al 44 found that the CMS spends an average of 1644 dollars more per socially isolated Medicare recipient (compared with non-Medicare recipients)—implying that social isolation is an important predictor of excess health care utilization. Moreover, similar to the current findings, Mosen et al 15 found that social isolation was associated with higher ED utilization and hospitalizations among a KPNW population that completed the MTHA survey. Unlike that prior study, this study examined the association of 5 social needs with utilization on a population level—also among a KPNW population that completed the MTHA survey.
In addition, this study results show which social needs are most strongly associated with future health care utilization, when analyzed collectively. The authors found that financial strain is associated with both increased future ED utilization and hospital admissions, whereas housing instability and social isolation are associated with future ED utilization.
The current study findings have relevance for future care improvement interventions health care systems may want to implement. To reduce excessive ED utilization, improvement efforts should prioritize patients with financial strain, housing instability, and social isolation. Meanwhile, prioritizing financial strain may be most important for reducing hospital admissions.
The current study findings have several limitations. First, the findings may not be generalizable to those in fee-for-service settings. However, regarding the demographic makeup of the population, recent research suggests that the Kaiser Permanente (KP) membership is generally representative of the communities it serves. 45 Second, the authors did not have information about survey nonrespondents, raising the concern for nonresponse bias.
However, by grouping a population with >1 years of MTHA surveys, the team constructed a sample of Medicare beneficiaries that reflected KPNW membership. Third, data on social needs were collected through self report and might be subject to recall and social desirability biases. Fourth, the population studied was ∼90% White. Although representative of the KPNW health care system, a limitation of the study is that it was not conducted in a more racially diverse population. Last, the study was conducted in an insured population residing in neighborhoods with lower than average levels of deprivation and results may not be generalizable to uninsured patients or those living in more deprived neighborhoods.
Future research should focus on 2 areas. First, this overall analysis should be replicated in (1) populations with chronic conditions and (2) more racially diverse populations—both in the under age 65 years population and the age 65 years and older population. Second, efforts are needed to (1) evaluate the effectiveness of interventions to resolve social needs and (2) determine whether resolution of social needs is associated with subsequent reductions in ED utilization and hospital admissions.
Conclusions
In this study of ∼10,000 KPNW Medicare patients seeking wellness visits, the authors found about one third reported 1 or more of 5 social needs. When adjusting for other social needs and population characteristics, financial strain, housing instability, and social isolation were independent predictors of future ED utilization, whereas financial strain was the only independent predictor of future hospital admissions.
Footnotes
Acknowledgments
The authors thank Jill Pope, who provided editorial assistance with the article, and Summer Rivera, who assisted in formatting references.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Support for this project was provided by the following: (1) National Institutes of Health (NIH), National Cancer Institute (NCI) Grant No. R01CA253028, (C. Kroenke, PI) and (2) Kaiser Permanente's Office of Community Health through the Social Needs Network for Evaluation and Translation (SONNET). SONNET is a national Kaiser Permanente (KP) program that convenes evaluators and researchers from its 8 regional care delivery systems, the KP Bernard J Tyson School of Medicine, KP's Office of Community Health, and from the Social Interventions Research and Evaluation Network (SIREN), a KP- and Robert Wood Johnson Foundation-supported network housed at the University of California, San Francisco. SONNET seeks to improve health of KP members and the communities they live in by developing and implementing new, scientifically driven strategies to shape social health practice and policy.
Supplementary Material
Supplementary Appendix SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.