
Abstract
Background:
A fast and simple tool is needed to test for the risk of mortality and rehospitalization in older patients.
Objective:
The aim of this study was to construct and validate a prognostic index using specific items from the Comprehensive Geriatric Assessment (CGA) in a large population of older hospitalized adults.
Method:
This was a prospective study of a 24-month follow-up period, between 2005 to 2008 in 3,043 elderly patients (mean age, 81 ± 6) discharged from three acute geriatric wards in the Marche region of Italy. Baseline predictors of demographics and 25 items from the CGA regarding functional and cognitive status, depression, co-morbidity, social isolation, and quality of life were used to build a summary score, the Hospitalized Older Patient Examination (HOPE) Index. The HOPE index was developed in 1,533 patients and validated in 1,510 consecutively hospitalized patients. Outcome measures were 24-month mortality and rehospitalization.
Results:
Three risk categories of HOPE based on the best sensitivity and specificity for mortality and rehospitalization were: Low (≤4), moderate (4–8), and high (≥8). Categorizing data across the HOPE index, mortality ranged from 7.9% to 14.5% in the development cohort and 6.2% to 14.0% in the validation cohort, whereas rehospitalization ranged from 68.3% to 79.4% and 69.8% to 79.8%, respectively. Kaplan–Meier survival curves demonstrated that risk for mortality increased with a worsening across the HOPE index (p < 0.001). In the development and validation cohorts, a close agreement was found for HOPE on mortality and rehospitalization with a receiver operating characteristic (ROC) of 0.69 (95% confidence interval [CI] 0.61–0.74) vs. 0.67 (95% CI 0.57–0.70) and rehospitalization of 0.62 (95% CI 0.58–0.66) vs. 0.60 (95% CI 0.56–0.63), respectively. In the development and validation cohorts, Cox proportional hazard models showed that a high HOPE index predicted risks of 2.38 (1.34–4.23) and 2.86 (1.24–6.61) on mortality and 1.27 (1.09–1.44) and 1.37 (1.10–1.64) on rehospitalization, respectively.
Conclusions:
HOPE may be useful for long-term clinical planning, discharge, and follow-up.
Introduction
A continuous decline in physical functioning plays an important role on frailty in elders. 1,2 Frail and/or vulnerable older persons have an increased risk for multiple adverse health-related outcomes, including falls, fractures, disability, institutionalization, and death. 3 –5 These individuals also account for the majority of excess health-care spending, and, due to the demographic shift in the last decades, there is a continuously growing rise in the number of frail elders. Previous studies testing diverse prognostic indexes integrating multiple domains have shown that these indexes can predict 1-year 6,7 and 2-year mortality 8,9 in both community-dwelling and hospitalized elders. 3,10,11 However, age-related risk factors of frailty on long-term rehospitalization have not been entirely identified. Considering that there are little data for hospitalized older patients, an extremely vulnerable group of individuals, the need for prognostic information remains essential for decisions concerning long term clinical planning, discharge, and follow-up.
The effect of environment on survival is complex, especially in a hospital setting, which often precedes a rapid exhaustion of functional reserves and leads to an instability of biological homeostasis. The literature is constantly increasing the awareness of diverse measures of frailty; however, such indexes are complex, time consuming, and thus difficult to apply in an acute setting. At the moment, clinicians are in need of a fast and simple approach to test for the risk of mortality and rehospitalization in older patients in the hospital setting.
Therefore, the aim of this study was to develop and validate the Hospitalized Older Patient Examination (HOPE) Index on 24-month mortality and rehospitalization derived from specific items of the Comprehensive Geriatric Assessment (CGA), a well-known geriatric tool related to clinical decision making. 12,13 We hypothesized that a global score created as the sum of specific items related to frailty and prognostic markers of the CGA would have a greater predictability on mortality and rehospitalization in older adults.
Methods
Subjects
The present study uses data from an observational study aimed at surveying general health status of elderly patients admitted to the Hospital Network of the Italian National Research Center on Aging (INRCA) of three geriatric hospitals in the Italian cities of Fermo, Appignano, and Ancona of the Marche region from 2005 to 2008. We excluded 341 persons because of the lack of information regarding 24-month in-hospital mortality; thus, our sample population consisted of two cohorts with a total of 3,043 patients aged 70 years and over. We included in both cohorts patients with the following characteristics: (1) Age over 70 years, (2) admitted to acute geriatric ward for unplanned admission, (3) had complete CGA data during hospital stay that was performed at discharge, (4) data regarding survival after 24 months from their hospital stay, and (5) signed written informed consent (or by a relative of critically ill or severely cognitive impaired patients). The first cohort created was the development cohort, which was necessary for the construction of the HOPE index. During the 2-year inclusion period of the development cohort, 1,533 patients were consecutively admitted to INRCA Hospitals. The development cohort consisted of all hospital admitted older patients from January, 2005, to December, 2006.
The second cohort was the validation cohort, which was needed to confirm the efficacy of the HOPE index on a 24-month mortality risk. The inclusion (using the same above characteristics as the development cohort) of the validation cohort consisted of n = 1,510 patients admitted consecutively from January, 2007, to December, 2008, to the same hospitals. The INRCA Review Board approved the study protocol.
Comprehensive Geriatric Assessment
All patients underwent a CGA performed by trained geriatricians, nurses, and clinical psychologists, which included the following multidisciplinary tests.
Social isolation
Social networks and informal social support were measured using the Lubben Social Network Scale (LSNS) developed for use in older adult populations in both a research and clinical setting. 14 The scale assesses the extent of social contact with family and friends. The test been associated with many health indicators, 15 and low scores on the LSNS have been correlated with higher mortality. 16 The total score from the LSNS was used in the development of the HOPE index. A cutoff score of <20 was used to categorize those at risk for social isolation and dichotomized as (<20 = 1, ≥20 = 0). 14
Co-morbidity
The Cumulative Illness Rating Scale (CIRS) was used to measure co-morbidity status. 17,18 It is made up of 14 categories, with a 0–4 grading scale of impairment in each organ system. The total score obtained represents the sum of each of the 14 individual system scores, with total scores varying from 0 to 56. The Co-morbidity index (CM2) was calculated as the number of categories with a score of 2 or greater, including psychiatric tests. 19 The total score of the CM2 was used for the HOPE index and dichotomized as follows: 0 = 0, 1–3 = 0.5, ≥4 = 1.
Measurement of cognition
Evaluation of global cognitive abilities was performed in numerous domains: Memory, orientation in time and place, attention, and other neuropsychological functions by means of Mini-Mental State Examination (MMSE). 20 The total score of the MMSE was used for the HOPE index and dichotomized as previously reported 21 as follows: ≥25 = 0, 24–21 = 0.25, 18–20 = 0.5, 11–17 = 0.75, ≤10 = 1.
Depression status
The Geriatric Depression Scale (GDS-15) was used to screen for depression. 22 Total scores were obtained by adding one point for each response for a depressive symptom, with a total score between 0 and 15. The total score of the GDS-15 was used for the HOPE index and values were dichotomized accordingly: 0–5 = 0, 6–9 = 0.5, ≥10 = 1.
Functional status
The Basic Activities of Daily Living (BADL), which defines the level of dependence/independence of six daily personal care activities, including bathing, toileting, feeding, dressing, urine and bowel continence, and transferring (in and out of bed), was used for the assessment of functional status. 23 The score for each question was based on patient ability to perform and categorized as follows: 0 = completely independent; 0.5 = partially independent; 1 = total dependence. The Instrumental Activities of Daily Living (IADL) was used to assess instrumental daily activities, such as using a telephone, shopping, food preparation, housekeeping, doing laundry, taking medicines correctly, and transfers. 24 IADL was dichotomized according to the interval 0–1 according to the number of possible available responses to each item. Thus, the HOPE index included each individual item (dichotomized according to the interval 0–1) of both the BADL and IADL.
Quality of Life Scale
The Health-Related Quality of Life Scale (Short Form SF-12) was used to assess the quality of life. 25 The SF-12 is a generic measure of health status, encompassing 12 questions covering eight dimensions of health significantly affected by medical condition—physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. In addition, the SF-12 assesses overall physical and mental function using summary scales which include the Physical Component Summary Score (PCS-12) and Mental Component Summary Score (MCS-12). SF-12 was designed as an alternative to the longer SF-36, and provides an accurate reproduction of summary measures. 26,27 A lower score in PCS reflects limitation in self-care, physical, social, and role activities, as well as severe bodily pain and frequent tiredness. Lower MCS scores indicate the presence of psychological distress and the limitation in usual social and role activities due to emotional problems.
The HOPE index included the following items from the SF-12: General health status (GH01), moderate physical activities (PF02), climbing several flights of stairs (PF04), regular daily activities accomplished less than one would like (RP2), limited in kind of work or other activities (RP3), bodily pain (BP), and mental health (MH3). 25 Each item was categorized to the interval 0–1 (from 2 to 6 intermediate responses) and each response was used for the HOPE calculation.
HOPE Index
The HOPE index was calculated using a similar method recently reported in the literature in older community-dwelling persons. 28 The index was calculated as the sum of 25 items selected from the CGA (see above) regarding functional status, cognitive status, depression, co-morbidity, basic and instrumental activities of daily living, social isolation, and self-perceived quality of life. The specific items to be included in the index were based on data from the literature regarding frailty, vulnerability, and prognosis. 10,11,28 –30 As already mentioned, individual variables were coded as follows: Binary variables used the convention that 0 indicated the absence of the deficit, whereas 1 indicated the presence of a deficit. For variables that included intermediate responses, we used additional values as necessary such as, 0.25, 0.50, etc. Thus, total scores ranged from 0 (no evidence of clinical deficits) to 25 (clinically frail/vulnerable).
Outcomes
Mortality
Vital status was assessed directly by consulting the centralized registry offices database of all intrahospital acute admissions ending in death of the entire Marche region. Dates of death were identified from death certificates that the central database of the Marche region holds. Death rates were calculated at 12 months and 24 months following enrolment. The total death rate at 24 months included that at 12 months.
Rehospitalization
All rehospitalization events refer to unplanned readmission to acute geriatric wards following study enrollment. This study refers to the use of the Italian public health-care system for hospital admissions, which is a common system capable of identifying all rehospitalization events as long as patients were readmitted to any public hospital in the Marche region. For analyses, the event of a rehospitalization was identified when an individual had an acute hospital readmission ≥2 during the study period, whereas those with ≤1 were considered not to have been rehospitalized.
Statistical analyses
Baseline clinical characteristics according to the total scores from each evaluation performed in the CGA and the total score of the HOPE index were compared between gender for each cohort using the chi-squared test or t-test when appropriate. The predictive accuracy of the cutoff points of the HOPE index used for mortality and hospitalization was calculated in both cohorts by estimating the sensitivity and specificity for each cut-off and receiver operating characteristic (ROC) analysis was applied to estimate the area under the ROC (AUC) for the overall test.
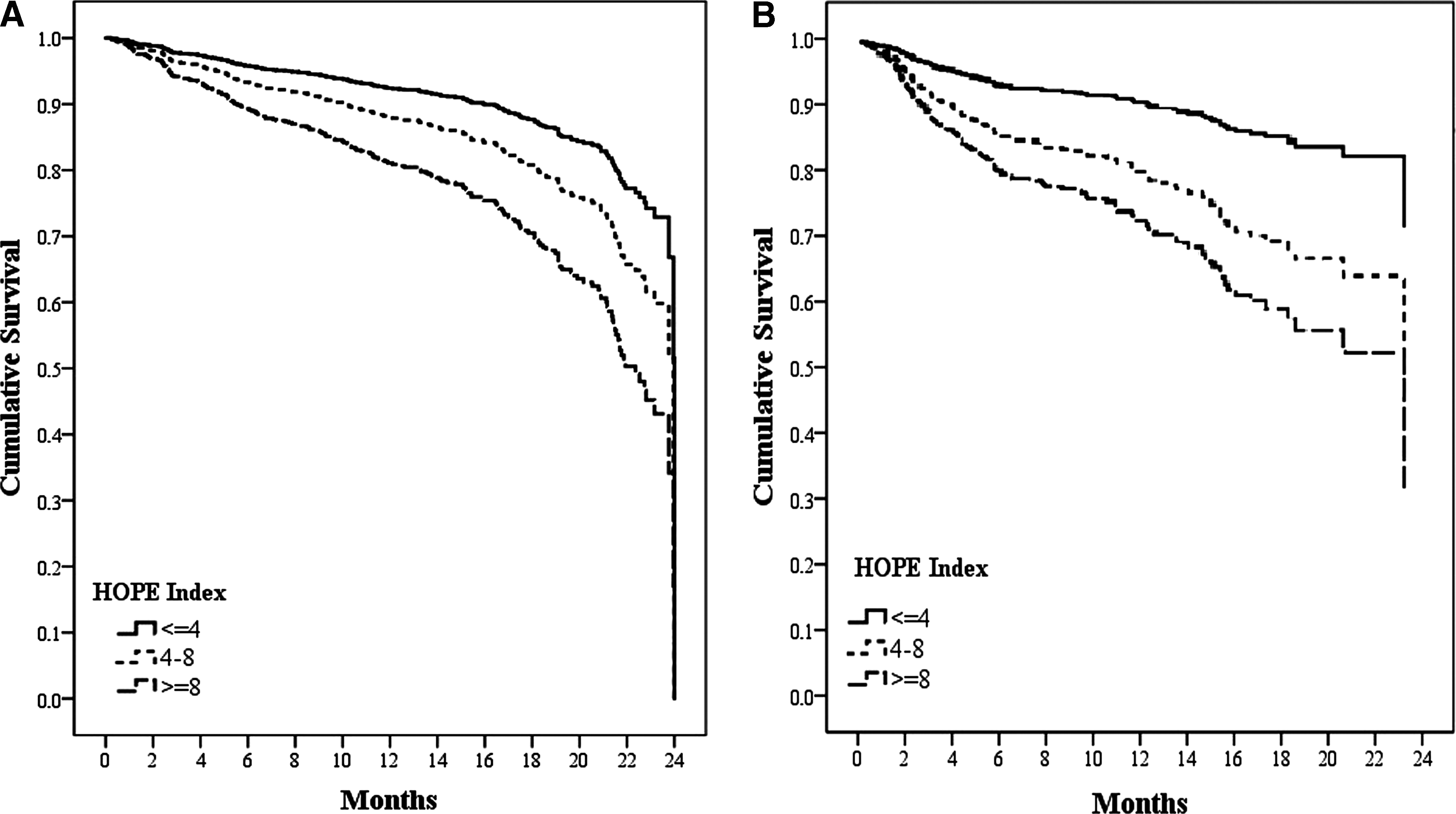
Kaplan–Meier curves were used to illustrate time to event of in-hospital mortality according to sensitivity and specificity cutoff points of the HOPE index: Low risk (0–4), moderate (4–8), high (≥8) for each cohort. 30 Having first checked for proportionality, the associations between HOPE index and time to death were established by using Cox proportional hazards regression analyses adjusted for age, sex, and years of education to estimate hazard ratios (HR) and the 95% confidence interval (CIs). Logistic regression models were used to test the odds ratio (OR) and CIs for mortality and rehospitalization for the HOPE index and its individual items to test that the index had a better predictive value than the single items.
A probability value less than 0.05 was considered statistically significant. Statistical analysis was performed using SPSS statistical software version 17.0 (SPSS Inc., Chicago, IL).
Results
Mean age of the entire study population was 81 ± 6 years with a mean length hospital stay of 13 ± 7 days. Baseline characteristics according to gender in the development and validation cohorts are summarized in Table 1. In both cohorts, women were older, more depressed, more likely to be socially isolated, presented more cognitive and functional difficulties, and had a lower perception of quality of life and a worse HOPE index compared to men (Table 1). Each score (range 0–25) from the HOPE index was tested to estimate its sensitivity and specificity toward mortality and rehospitalization (data not shown), and the best fit cutoff scores are reported in Table 2. The total score of the HOPE index also maintained comparable performance in ROC analyses in development and validation cohorts for mortality 0.69 (95% CI 0.61–0.74) vs. 0.67 (95% CI 0.57–0.70), respectively. Similar findings were also found between groups on rehospitalization at 24 months 0.62 (95% CI 0.58–0.66) vs. 0.60 (95% CI 0.56–0.63) (Table 2).
0.05.
<0.001.
CIRS, Cumulative Illness Rating Scale (CM2, co-morbidity index from the GDS); MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale; ADL, Activities of Daily Living; IADL, Instrumental Activities of Daily Living; LSNS, Lubben Social Network Scale; PCS, physical component summary; MCS, mental component summary of the SF-12 (see Methods); HOPE, Hospitalized Older Patients Examination Index.
HOPE, Hospitalized Older Patients Examination Index; HR, hazard ratio; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; AUC, area under the ROC.
The findings from the Kaplan–Meier survival curves demonstrated that the risk for mortality increased with a worsening across HOPE index cutoffs (Fig. 1A,B). When patients were stratified across HOPE index cut-point categories, mortality ranged from 7.9% to 14.5% in the development cohort and 6.2% to 14.0% in the validation cohort, whereas rehospitalization ranged from 68.3% to 79.4% in the development cohort and 69.8% to 79.8% in the validation cohort.
(
In the development cohort, Cox proportional hazard models were performed to examine the relationship among specific variables, mortality and rehospitalization. In particular, these models testing the predictive value of age, female gender, low educational level, and high HOPE index on mortality showed hazards risks of 1.04 (95% CI 1.01–1.06), 0.65 (95% CI 0.53–0.82), 0.57 (95% CI 0.39–0.83), and 2.38 (95% CI 1.34–4.23), respectively (Table 3). In particular, those in the high-risk category (HOPE score ≥8) had an approximately three-fold risk compared to those in the lowest category (HOPE score ≤4). Similar findings were also found in the validation cohort with risk estimates of death (HR) that were only slightly increased for age in the validation cohort (Table 3).
<0.05.
<0.001.
HR, Hazard ratio; CI, confidence interval; HOPE, Hospitalized Older Patients Examination Index.
Due to significant differences between genders, we tested whether a high HOPE index was correlated with death separately by gender. We found that the HOPE index in women from both the development and the validation cohorts had the following HRs (95% CI) of 2.51 (1.20–5.25] and 4.87 (1.69–14.08), respectively. Similar findings were also found in men from the above cohorts with a HR of 2.32 (1.28–4.20) and 2.60 (1.21–5.60), respectively.
Last, the prognostic value of the HOPE index compared to each individual item used for its development on mortality and rehospitalization in both cohorts was tested (Table 4). We found that beta coefficients and ORs were significantly higher for the HOPE index high cutoff compared to its single components (Table 4).
Number of deficits from BADL or IADL. (Single questions from BADL or IADL were categorized as 1 = inability to perform, 0 = complete ability.)
HOPE, Hospitalized Older Patients Examination Index; ADL, Activities of Daily Living; IADL, Instrumental Activities of Daily Living; MMSE, Mini-Mental State Examination; CIRS, Cumulative Illness Rating Scale (CM2, co-morbidity index from the GDS); GDS, Geriatric Depression Scale; LSNS, Lubben Social Network Scale; BADL, Basic Activities of Daily Living; IADL, Instrumental Activities of Daily Living.
Discussion
In a large population of hospitalized older patients, a simple prognostic index, HOPE, was developed and validated using available information from specific items of the CGA. Specific cut points were found and, in particular, a score of 8 or higher was identified as the score at which there was the best performance toward mortality and rehospitalization. A high HOPE index predicted an over two-fold risk for mortality and an approximate 1.5-fold risk for rehospitalization at 24 months. Even though men had higher mortality rates than women, the HOPE index predicted similar mortality rates in both genders. This index adds information to the existing literature regarding prognostic tools for older persons in the hospital setting. Interestingly, we found that mortality rates at 12 months compared to 24 months did not substantially increase as one would have expected. This finding may be explained by the vulnerability of patients at an older age compared to those reported by Pilotto et al. 11 This study applied a model that also encompassed many of the clinical markers of frailty in an operational manner for detecting those patients at significantly higher risk of death or rehospitalization.
The concept of frailty is not a well-defined clinical entity. Frailty embraces a range of clinical conditions such as old age, limited mobility, co-morbidity, and low social status. 3,31 Many studies have created sophisticated models for defining and grading frailty. 10,11,28 –30 Frailty is often used as an exchangeable term for disability, co-morbidity, and poor health status and is considered as an irreversible condition leading to adverse health outcomes. It is important to note that frailty is considered to be a continuous process in which several degrees of severity need to be identified to begin research and clinical intervention trials.
Vulnerability is defined as persons age 65 and older at increased risk of death or functional decline. The Vulnerability Elders Survey (VES-13), an important screening survey, only asks older persons to report their age, ability to perform six physical and five functional activities, and their self-rated health. 32 It does not take into consideration clinical observations, and, thus, may underestimate the prevalence of underdiagnosed conditions. A recent report demonstrated that higher VES-13 scores were associated with greater probability for death in older community-dwelling elders with memory problems or at risk for falls over a 4.5-year follow-up. 29 However, data regarding older hospitalized elders has been linked to the relationship between the quality of care during hospital stay on the postdischarge mortality. 33 An interesting finding was that 24-month mortality and rehospitalization were only slightly higher than those at 12 months. These data underline that the first 12 months following an acute hospital admission represent a critical time span in which intervention programs would be of the most importance in older persons. We specifically used specific parameters from the CGA that may identify both vulnerability and frailty markers (as taken from their operational definitions) to categorize older persons in the hospital setting at a severe risk for mortality or rehospitalization.
Indeed, many studies performed in well-functioning elders have shown that parameters from the CGA are important for predicting mortality and hospital admissions 4,10,30 ; however, we aimed at identifying specific components of frailty and vulnerability in a hospital setting. This study confirmed that the aggregation of information from the CGA in older hospitalized patients played an important role in prognosis. However, for the development of the HOPE index, we specifically used parameters that have been identified in the literature as important markers of frailty in older persons, independently of their living environment. Indeed the HOPE index including the co-morbidity from the CIRS score, social, functional, and cognitive items, all derived from CGA, thus underlining that the aggregation of specific items is more predictive than single parameters alone.
To some extent, our data also confirm the important findings from Pilotto et al. 11 that demonstrated that the total scores from the CGA were used to create cluster analysis of a prognostic index for older hospitalized persons. This technique was well validated, but not easy to apply in the routine hospital setting. Indeed, our study adds new information to a more simple way to weigh the specific items on all tests included in the CGA. This possibility allows for a rapid and valid response to prognosis in older hospitalized persons. Furthermore, the finding that the prognostic value of the HOPE index was superior to the predictive values of its individual items confirms that the use of a multidimensional evaluation plays a fundamental clinical role in older persons. 34 Our findings add further insight to the valid use of the CGA in the hospital setting. Although the HOPE index predicted adverse outcomes, research will be needed to test whether high-risk individuals are most likely to benefit from preventive interventions and to identify those with a lower risk that may gain more benefits from screening evaluations in which elderly persons may be excluded by their age.
Some potential limitations in our study need to be underlined. The individual components of the HOPE index were chosen on the basis of previous literature regarding their importance in the CGA for clinical decision making. 12,13 After analyzing the individual predictive values of such components on mortality, we were not able to confirm that all parameters were predictive. However, this finding emphasizes the importance of the aggregated information of the index in older persons. Another limitation is that the index was used only on hospitalized older persons and thus its applicability in community-dwelling or institutionalized elders will need further clarification. Considering that hospitalized older persons are an extremely vulnerable group of persons, we specifically aimed at investigating the use of a geriatric prognostic tool.
Some study limitations should be underlined. Unfortunately, the CGA did not include the Mini-Nutritional Assessment (MNA), an important tool for nutritional assessment, especially in older persons. However, our assessment did include the Health-Related Quality of Life Scale (SF-12), which has been shown to be highly correlated with the MNA in a large group of hospitalized older persons. 35 It is also important to underline that some data may be missing regarding mortality and rehospitalization. Due to the common hospital system employed in Italy, our data on mortality and readmissions were limited to the Marche Region. However, the use of an out-of-region hospital use is negligible, especially at an old age. Hospital readmissions were also unplanned, which strengthens our findings testing the prognostic index on these events.
Conclusion
Our data confirm the importance of the use of HOPE index in older patients, and its application is particularly appealing for acute geriatric wards. Interventions aimed at improving physical health status in high-risk older hospitalized persons will be of great importance in the future to test the ability of reducing mortality in such a critical group of individuals.
Footnotes
Acknowledgments
Author contributions were as follows: Spazzafumo, Sirolla had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Abbatecola, Spazzafumo, Sirolla, Corsonello; analysis and interpretation of data: Abbatecola, Spazzafumo, Sirolla; drafting of the manuscript: Abbatecola, Spazzafumo, Corsonello; statistical analysis: Spazzafumo, Sirolla, Abbatecola; critical revision of the manuscript for important intellectual content: Bustacchini, Guffanti.
This study was supported by the Italian National Research Center on Aging (INRCA).
Author Disclosure Statement
The authors declare no conflict of interest.