
Abstract
Background:
Although increased survival among females is observed throughout much of adult life, supporting evidence among the oldest old is lacking.
Objective:
We examined the hypothesis that gender differences in survival diminish with advancing age.
Methods:
The Jerusalem Longitudinal Study follows a representative cohort born 1920–1921, comprehensively assessed at ages 70, 78, 85, and 90 (n=463, 927, 1224, and 673, respectively). Mortality data were collected during 1990–2013. Kaplan–Meier survival curves and mortality hazards ratios (HRs) were determined, adjusting for gender, marital status, education, loneliness, self-rated health, physical activity, functional status, neoplasm, diabetes mellitus, hypertension, and ischemic heart disease.
Results:
Survival between ages 70–78 was 77.3% (n=358/463), 78–85 was 68.9% (n=635/927), 85–90 years was 71.1% (n=870/1224), and 90–93 years was 80.5% (n=542/673). With advancing age, the survival advantage among females versus men declined—at ages 70–78 (85.6% vs. 71%, p<0.0001), 78–85 (74% vs. 63%, p=0.001), 85–90 (74% vs. 67.5%, p=0.06), and 90–93 (80% vs. 81%, p=0.92). Compared to females (HR=1.0), the adjusted HR for male mortality at ages 70–78 was 2.93 (95% confidence interval [CI] 1.75–4.91), ages 78–85 was 2.1 (95% CI 1.5–2.92), ages 85–90 was 1.6 (95% CI 1.2–2.2), and ages 90–93 was 1.1 (95% CI 0.7–1.8).
Conclusions:
Our findings confirm the hypothesis that the increased longevity observed among females at age 70 gradually diminishes with advancing age, and disappears beyond age 90.
Introduction
G
Literature that does exist among older people is often contradictory. Findings from some cross-sectional studies have suggested a convergence of differences in co-morbidity between the genders in several areas of health, function, and disease among the oldest old. 9 Similarly, among acutely ill older people age 85 and over, gender per se failed to predict subsequent mortality at 3 months following acute hospitalization. 10 In contrast, a 12-year follow-up of 2200 Japanese community-dwelling subjects aged over 60 years old at baseline, suggested that gender differences in mortality and morbidity remained pronounced throughout follow-up. These findings did not however extend to the oldest old, aged 85 years and older. 3
Attempts to understand the gender differences in longevity often highlight the conceptual issue—whether males die younger due to increased risk of mortality, or whether females survive longer due to some perhaps more intrinsic survival benefit. It is probable that increased risk of mortality among males is the predominant vector, certainly at younger ages, rather than a specific intrinsic survival benefit associated with female gender. 8 However, the malignant profile of risk factors associated with male gender at younger ages is subject to change with advancing age. Indeed, males reaching very old age are by definition “survivors,” and may display a different, less malevolent, profile of risk. Therefore, it is possible that among males reaching very old age, gender differences in mortality would be expected to decline.
The aim of this study was to examine the hypothesis that gender differences in longevity gradually decline with advancing old age, among an age-homogeneous birth cohort of community-dwelling older people followed up from ages 70 to 93 years old.
Methods
Study sample
The Jerusalem Longitudinal Cohort Study has followed a birth cohort of Jerusalem residents (born June, 1920–May, 1921) from age 70 at baseline in 1990 until the present time. A detailed description of study methodology has been described previously. 11 –13 Comprehensive geriatric assessment was performed at baseline at age 70 (phase 1, 1990–1991), at age 78 (phase 2, 1997–1998), at age 85 (phase 3, 2005–2006), and again at age 90 (phase 4, 2010–2011). The present study is based upon data collected at each of the four successive phases, describing the cohort at ages 70, 78, 85, and 90.
The study sample, which formed about one-third of the total birth cohort, was randomly selected from the electoral registry. The representative nature of the study sample was confirmed by finding similar rates of hospital in-patient morbidity, health service utilization, and mortality between the study sample, subjects who refused, and those not approached to enroll. 14 To maintain study sample size and to counteract the attrition caused by the mortality, the original baseline sample was augmented with additional randomly selected new subjects (from the same 1920–1921 birth cohort) at subsequent phases in 1998 (age 78), 2005 (age 85), and again at 2010 (age 90). No significant differences existed for either co-morbidity or subsequent mortality rates among subjects enrolled at later stages. Proxy informants, with consent from legal guardians, were used for extremely frail or demented subjects unable to provide factual information. Each participant, or legal guardian, provided informed consent, and the Hadassah Hebrew University Medical Center Institutional Review Board approved the study.
The present study examines the survival of 463, 927, 1224, and 673 subjects, enrolled at ages 70, 78, 85, and 90 (at 1990–1991, 1997–1998, 2005–2006, and 2010–2011, respectively) followed up from ages 70–78, 78–85, 85–90, and 90–93 years, respectively.
Measures and data collection
The study instrument was a structured questionnaire, performed by interview at home, by a trained study nurse or occupational therapist (demographic characteristics, personal history, lifestyle, function, and cognitive status) and the study physician (medical history, system review, and examination).
Study measures
Socio-demographic measures
These included educational status (dichotomized to <12 years or >12 years schooling), financial status based upon self-reported difficulty getting through the month, marital status (married versus all others), living arrangements (living alone versus all others), and loneliness. Subjects were asked how often they felt lonely (dichotomized to not lonely versus lonely). 15,16
Functional measures
These included physical activity levels. Subjects were questioned: “How often are you physically active?” answers being: (1) <4 hr/week, (2) about 4 hr/week, (3) at least 1 hr/day (e.g., regular physical activity such as walking), or (4) vigorous sports at least 2/week (e.g., jogging, swimming). Physical activity was dichotomized to inactive (answer 1) versus active (answers 2, 3, or 4). This questionnaire was adapted from the Gothenburg 70-year-olds Longitudinal Study and predicts functional status and morbidity among our cohort 17,18 ; frequency of leaving the house (dichotomized to less than 1/week versus more than 1/week); frequency of reading (dichotomized to rarely <1/week versus >1/week); functional status was assessed by self-report according to direct questioning for each of the various basic Activities of Daily Living (ADLs) (transfer, dressing, bathing, toilet hygiene, eating, continence). 19 Subjects were graded as either completely independent without any difficulty, independent with difficulty, or dependent on another person. Subjects who reported being independent yet with difficulty in at least one of the basic ADLs were defined “performing ADLs with difficulty,” and subjects requiring help from another person in one or more of the basic functions was defined being “Dependent on another person.” Hearing was assessed using the whisper test (dichotomized to impaired or not); vision was assessed using Snellen chart testing, and dichotomized to impaired (best eye corrected vision ≤20/40) or not.
Common geriatric problems
Evaluation included the following: Self-rated health was evaluated using the question: “Do you feel healthy in comparison to people your age?”; sleep satisfaction; depression according to the Brief Symptoms Inventory (BSI) 20 ; cognitive status according to the Mini-Mental State Examination (MMSE), 21 with impairment defined as a MMSE score <24/30; the presence of at least one fall in the previous year.
Disease status
Hypertension was defined by either self-reported history or treatment with antihypertensive medications 22 ; diagnoses of ischemic heart disease (IHD), diabetes mellitus (DM), history of neoplasm (excluding non-melanoma skin cancer); and other major diseases were made by the study physician, according to the International Classification of Disease (ICD-9). 23
Outcomes
Death from any cause was the primary outcome throughout the study period of June, 1990–June, 2013. Mortality data were obtained from review of all obligatory notifications of death issued by the Ministry of Interior. This provided 100% surveillance of mortality data for subjects in Israel.
Statistical analysis
Descriptive statistics were performed using chi-squared tests for categorical variables (Table 1). Among subjects who died during follow-up, we calculated the mortality risk ratios (RR) with 95% confidence intervals (CI), for males compared to females, according to numerous baseline characteristics. Survival differences between males and females were examined using Kaplan–Meier survival curves and the log rank test. Cox proportional hazard models determined the hazards ratios (HRs) associated with male gender compared to females. Unadjusted and adjusted HRs were determined in separated models at ages 70, 78, and 85, with mortality follow-up from ages 70–78, 78–85, 85–90, and 90–93, respectively. Different models were constructed to account for various domains of confounding variables. The models included those variables for which significant gender differences were observed between mortality RRs, and considered to be important mortality risk factors. Model 4 combined significant co-variables from models 1, 2, and 3.
The following models were thus constructed: 1. Model 1 (socio-demographic): Gender, marital status, education, loneliness. 2. Model 2 (geriatric and functional): Gender, self-rated health, sleep satisfaction, pain, depression, physical activity, ADL dependence, MMSE score <24. 3. Model 3 (medical): Gender, neoplasm, diabetes mellitus, hypertension, IHD. 4. Model 4 (combined variables): Gender, marital status, education, loneliness, self-rated health, physical activity, ADL dependence, neoplasm, DM, hypertension, IHD.
p values between male versus females: * p<0.05, ** p<0.01, ** p<0.001.
M/F ratio, male/female ratio; ADL, Activities of Daily Living; MMSE, Mini-Mental State Examination.
All p values were two-tailed, and p<0.05 was considered significant. The sample size was sufficient to achieve a power of 80% with an alpha coefficient of 0.05. Data storage and analysis were performed using SAS v. 9.1e (SAS Institute, Inc., Cary, NC).
Results
At ages 70, 78, 85, and 90, a total of 463, 927, 1224, and 673 subjects, respectively, were included in the study. Table 1 shows the gender differences in baseline characteristics, and the changing male/female (M/F) ratio for common function impairments, geriatric syndromes, and co-morbidities, with increasing age. Profound socio-demographic changes occurred with increasing age, with the majority of males remaining married at 90 compared to a minority of females (58% versus 9.1%), and 50.8% of females living alone at age 90 compared to 24.4% of males. Nonetheless, self-reported loneliness remained remarkably consistent irrespective of age, being twice as common among females. Functional differences between the genders were observed throughout, with males consistently being more physically active (up to age 85), leaving the house more often, and reporting consistently reduced levels of functional impairment as measured by both difficulty in performing ADL and also dependence in ADL. The magnitude of differences observed between the genders was seen to gradually diminish with increasing age, with few significant differences observed by age 90.
Decreased co-morbidity was observed among males compared to females for most common geriatric problems throughout follow-up, with reduced likelihood of poor sleep satisfaction, depression, cognitive impairment, chronic pain, as well complaints of poor self-rated health among males throughout the entire period of follow-up. With the exception of neoplasm, which was more frequent among males with rising age, the gender differences observed for the common chronic illnesses remained fairly stable throughout follow-up.
During the period of follow-up from ages 70–78, 78–85, 85–90, and 90–93, the overall survival rates among the study sample were 77.3% (358/463), 68.9% (635/927), 71.1% (870/1224), and 80.5% (542/673). Figure 1 shows the Kaplan–Meier unadjusted survival curves for males and females. Survival rates among females versus males at ages 70–78, 78–85, 85–90, and 90–93 years were 85.6% versus 70.5% (log rank p<0.001), 73.9% versus 62.6% (log rank p=0.001), 74.1% versus 67.5% (log rank p=0.011), and 79.8% versus 81.2% (p=0.92).
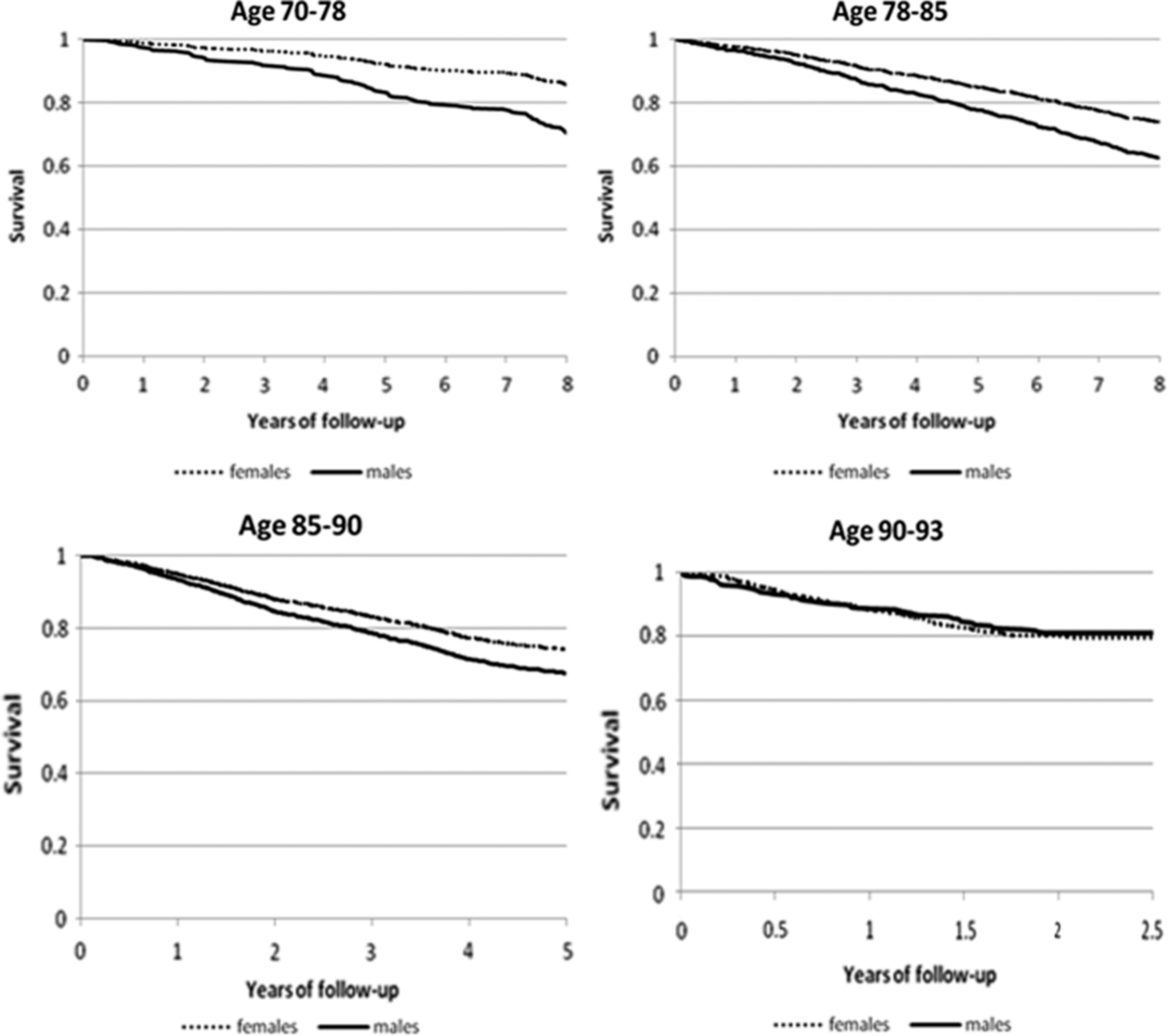
Gender differences in survival with advancing age. Kaplan–Meier survival charts showing the differences in survival for males and females during follow-up from ages 70–78 (p<0.001), 78–85 (p=0.001), 85–90 (p=0.011), and ages 90–93 (p=0.67).
An analysis of relative risk of mortality during follow-up for males compared to females according to baseline characteristics is shown in Table 2. Higher RRs of mortality were observed without exception for males compared to females at ages 70, 78, and 85; however, the magnitude and significance of this difference declined progressively, and by age 90 no significant differences in RRs were observed between the genders. The equalization of RR between the genders and disappearance of gender differences at age 90 were observed uniformly across social, functional, geriatric, and medical domains.
ADL, Activities of Daily Living; MMSE, Mini-Mental State Examination.
Results of Cox proportional hazards models are shown in Table 3. Both unadjusted and adjusted mortality HRs for males compared to females (reference HR=1.0) were seen to decline consistently with advancing age. This was true after adjusting for socio-demographic characteristics (model 1), for common geriatric and functional problems (model 2), medical status (model 3), as well as a combination of significant variables from socio-demographic, functional, and medical domains (model 4).
Model 1—Gender, marital status, education, loneliness; model 2—gender, self-rated health, sleep satisfaction, pain, depression, physical activity, ADL dependence, MMSE <24; model 3—gender, neoplasm, diabetes mellitus, hypertension, ischemic heart disease; model 4—gender, marital status, education, loneliness, self-rated health, physical activity, ADL dependence, neoplasm, diabetes mellitus, hypertension, ischemic heart disease.
df, degrees of freedom; ADL, Activites of Daily Living; MMSE, Mini-Mental State Examination.
At age 70, male gender remained a significant predictor of subsequent mortality despite adjustment for numerous variables. With advancing age, the magnitude of this effect declined progressively, as did the significance, and by age 90 gender no longer was independently associated with mortality.
Discussion
This prospective longitudinal study of a representative birth cohort of community-dwelling people followed up from age 70 to 93 years old confirms the hypothesis that gender differences in survival gradually decline with advancing age. Indeed, beyond the age of 90 years, survival was identical for men and women. Although gender differences in co-morbidity were consistently observed across a range of socio-demographic, functional, and medical characteristics despite increasing age, nonetheless the magnitude of the gender differences observed among many of the variables also showed a gradual decline with increasing age, as did the associated relative risk of mortality. Our finding of declining gender differences in co-morbidity and its associated mortality risk, and the complete disappearance of gender differences in survival among the oldest old, is, to our knowledge, a novel finding.
In contrast to research that exists concerning gender differences among middle-aged subjects, there is surprisingly little research among older people in general and the oldest old in particular. Indeed a recent meta-analysis investigating gender differences in mortality included a total of 72 studies. 8 The majority of studies included younger subjects drawn from a very wide age span, with subjects aged over 75 present only in eight of the 72 studies, and only six studies focused specifically upon the subjects aged over 65. Although male mortality was consistently higher below age 64, a blunting of this effect was observed beyond age 65.
Growing doubt exists concerning the assumption that risk assessment and survival trajectories can be accurately extrapolated from middle-aged populations to very old people. 23 –26 Indeed many of the common conventional risk factors and health predictors of middle age are becoming to be accepted as less important predictors of health outcomes among the increasingly older population, whereas functional parameters and non-conventional measures often serve better to predict well-being and survival at the extremes of old age. 27 –29
In a hospital-based study of acutely ill older people, 10 gender differences were evaluated according to a comprehensive multi-dimensional assessment spanning clinical co-morbidities, functional status, as well as physiological measures. Male gender was associated with far worse health parameters at younger ages, and yet among patients aged 90 or older no significant gender differences in either morbidity or mortality were observed. Although these findings are limited to the acute care environment, they nonetheless provide further evidence in keeping with our findings, which also describe the absence of gender differences in both co-morbidity and survival among the oldest old. A related issue concerns potential gender differences in delivery of care among the elderly. Disagreement exists and findings are often conflicting as to whether or not the intensity of care among very old people is equivalent between the genders. Some authors have suggested that females receive less aggressive care due to their apparent greater baseline co-morbidity, whereas others have noted that the poorer outcomes among males may be in part be due to perceived gender differences in life expectancy. 30
Gender differences in survival and longevity have been observed by several researchers to be population specific. 31 Both cross-national and historical comparisons suggest that the male-to-female ratio among the very old is most likely reflective of differences in rate of changes in survival among middle-aged populations over the last century. Furthermore, gender-specific differences in longevity have been found to vary according to different geographical regions within the same country. Thus, in an analysis of Italian centenarians, wide differences in male-to-female ratio were observed, with highest male longevity found in the most isolated regions, where in-breeding was greatest. 32 The authors suggest that female survival into extreme old age may be less dependent upon genetics than their male counterparts, and that oldest old females exploited a healthier life style and enjoyed more favorable environmental and cultural conditions. Age-related differences in both pro-inflammatory status and pro-/anti-inflammatory gene variants have been shown to exhibit gender differences, with the suggestion that a genetic predisposition to a weakened inflammatory response may actually serve as a protective factor in the pathogenesis of coronary heart disease. 33 The differences in geographic and demographic evidence underline the complex and changing interplay of population-specific genetic factors, environment, and chance and their role in longevity. 34
Limitations to our study exist. Because the methodology of our study included a narrow birth cohort, our conclusions are thus limited to a specific age strata of elderly people. The study cohort was highly heterogeneous in origin, and only 16% were native born at baseline, with the remainder reporting over 40 different countries of birth. Furthermore, the study reflects an urban population. Nonetheless, the study sample has been shown to be representative of the entire age cohort within the Jerusalem area (including non-urban elderly), with similar morbidity and mortality rates. 9,10,11,12 Similarly, the representative nature of our study cohort concerning older people in other societies deserves mention. Although the profile of health, function, and co-morbidity among our cohort is very similar to that of similar aged cohorts in Europe, 35,36 nonetheless there is a need to confirm our findings in similar aged cohorts from other countries and cultures. Cross-cultural studies and comparisons between different cohorts would be useful in determining whether the disappearance of gender differences among the oldest old is intrinsic to the biological process of aging, and to help in differentiating and quantifying the influence of social and societal changes. Further limitations include the lack of in-depth assessment of specific gender-related roles at home, as well as more detailed sociological assessment of gender-sensitive issues. The comprehensive nature of our assessment precluded in-depth questions, but it enabled a breadth of question covering numerous domains.
In conclusion, this study not only confirmed the hypothesis that gender differences in survival decline with advancing age, but actually described their complete disappearance among the oldest old.
Footnotes
Acknowledgments
This work was supported by funds from the Ministry of Senior Citizens of the State of Israel and Eshel—the Association for the Planning and Development of Services for the Aged in Israel. These funds were used exclusively to support the research effort, primarily as salaries to ancillary staff. No research funds were received by any author of this paper. The sponsors had no role in the study design, data analysis, preparation, or approval of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Author contributions: Study concept and design, J.S., A.C., E.E.M., J.M.J.; acquisition of data, J.S., A.C., J.M.J.; analysis and interpretation of data, J.S., A.C., E.E.M., J.M.J.; drafting of the first manuscript and critical revision of the manuscript for important intellectual content, J.S., A.C., E.E.M., J.M.J.; statistical analyses, E.E.M., J.S., A.C., J.M.J.; administrative, technical, or material support, J.S.; obtained funding, study supervision, J.S.