
Abstract
External skin-stretching devices have been developed and used for wound closure since 1970s. Devices such as Miami STAR®, SureClosure®, TopClosure®, and WiseBand® have their own advantages and disadvantages. The modified external skin-stretching technique of this case series study has the advantage to improve tension distribution and simplified the application. Between January 2014 and June 2017, 20 patients were treated with the modified external skin-stretching device for the closure of the skin defects of the trunk (n = 6) and extremities (n = 14). Skin defects ranged from 8 × 5 to 19 × 16 cm achieved primary closure with the utilization of the modified skin-stretching device without major complications. Subsequent minor revisions were performed under local anesthesia between 6 and 12 months postoperatively. The modified skin-stretching device utilized biomechanical properties and mechanical creep of skin tissue to achieve a reliable and effective primary closure for moderate to extensive skin defects. Therefore, this modified external skin-stretching technique provided, in the appropriate setting, an effective alternative to skin grafts or free flaps.
Introduction
Skin defects caused by trauma, radical resection, or scar excisions frequently pose challenges for surgeons. Plastic surgeons usually offer skin grafting or flap transfer to solve these issues. However, the dilemma of a large defect with insufficient surrounding tissue volume had constantly questioned the operators for decades. Although free tissue transfer or perforator flaps are considered an ideal option in several situations, these may be limited by a few factors such as availability of donor site, patient health's condition, and comorbidity or the need of expert microsurgical techniques. Wilson 1 first described the concept of tissue expansion when he observed a repeatedly incremental stretching of the skin in serial wound excisions.
Neuman 2 utilized a subcutaneous postauricular balloon to regularly expand the skin tissue for the reconstruction of a partially avulsed ear. Later on, Gibson and Kenedi 3 investigated the mechanical properties of the skin at cellular level, observing that a progressive elongation of the skin resulted by the structuring and realignment of collagen fibers. Finally, tissue expansion technique was globally promoted by the research of Radovan 4 and Austad et al. 5
As is documented that progressive linear tension will cause mechanical creep and stress relaxation of skin tissue, traditional expanders will cause biological creep, but their value in stimulating mechanical creep is doubtful. Following the acceptance of the conventional intrinsic tissue expansion, extrinsic forces were also applied to recruit additional skin tissue for reconstruction. In 1976, Barrer et al. 6 described a retention-bridging device for skin closure after laparotomy. Consequently, Hirshowitz et al. 7 in 1986 reconstructed the nasal tip and alar nose with additional skin created by load cycling intraoperatively. Liang et al. 8 used a presuturing technique to close preoperatively the skin defects ranging from 4 up to 10 centimeters. achieving 40% less tension.
Since then, different devices have been developed for the purpose of external skin stretching. In 1992, Cohen and Cosmetto 9 first published a suture tension adjustment reel called Miami STAR®. This device included seven functional components and it was used intraoperatively for immediate tissue expansion. One year later, Hirshowitz et al. 10 introduced a skin-stretching device named SureClosure® to join extra skin in a delayed manner. Furthermore, different skin-stretching products include TopClosure® and WiseBand®, which use similar concepts with variable results.
The external tissue expansion mainly stimulates the mechanical creep of the skin tissue. The external traction of the skin is considered to be a safe procedure with the manipulation of the device being extremely simple to use. Moreover, this technique can be used on several different anatomical sites, especially on limbs where internal expansion is often difficult to apply. Other indications to apply the external skin-stretching technique include defects that are not suitable for grafting or limited by the donor site availability for flap reconstruction or need an improvement of the cosmetic appearance after primary closure. In this study, an external skin-stretching device (KeKe®, Henan, China) was used. This case series presents clinical experiences with the use of novel device, which applied modified technique for external tissue expansion.
Patients and Methods
From January 2014 to June 2017, a total of 20 patients underwent external skin-stretching expansion to cover soft tissue defects of the trunk and extremities. Of these 20 patients, 9 were male and 11 were female, with an average age of 32 years (range 22–58 years). The applications ranged from burn scar revision, abdominal wall reconstruction after tumor resection, reconstruction postexcision of giant congenital melanocytic nevus, closure of traumatic soft tissue defects, and closure of flap donor sites (Table 1).
Patient Characteristics
BS, burn scar; GCN, giant congenital nevus; MT, metastatic tumor; SL, skin laceration.
All procedures were performed by an expert plastic surgeon (P.R.M.). The patients were fully informed and this study was considered exempt from institutional review board approval (SH9H-2020-T326-1) since the data were collected retrospectively.
Surgical technique
First stage
A preoperative or intraoperative pinch test was used to assess the laxity and possibility of a primary closure of the defect. Based on previous experiences and concepts summarized in Table 2, the borderline ranges could be primarily closed with the assistance of a modified external skin-stretching device in a cohort of Asian patients.
Defect Management in Different Anatomic Area
Anterior tibial defect is excluded.
The modified skin-stretching device used consisted of a pair of stainless steel shafts, two bolts each with a small hook and a spring scale on it and a stabilizing wrench to lock the devices (Fig. 1). The stainless steel shafts were in three sets of lengths (11, 14, and 17 cm) to accommodate the size of the defect. The size chosen was based upon the measurement of the defect or due to anatomical factors over the defect (e.g., whether the shaft can be placed comfortably in the area to be expanded).
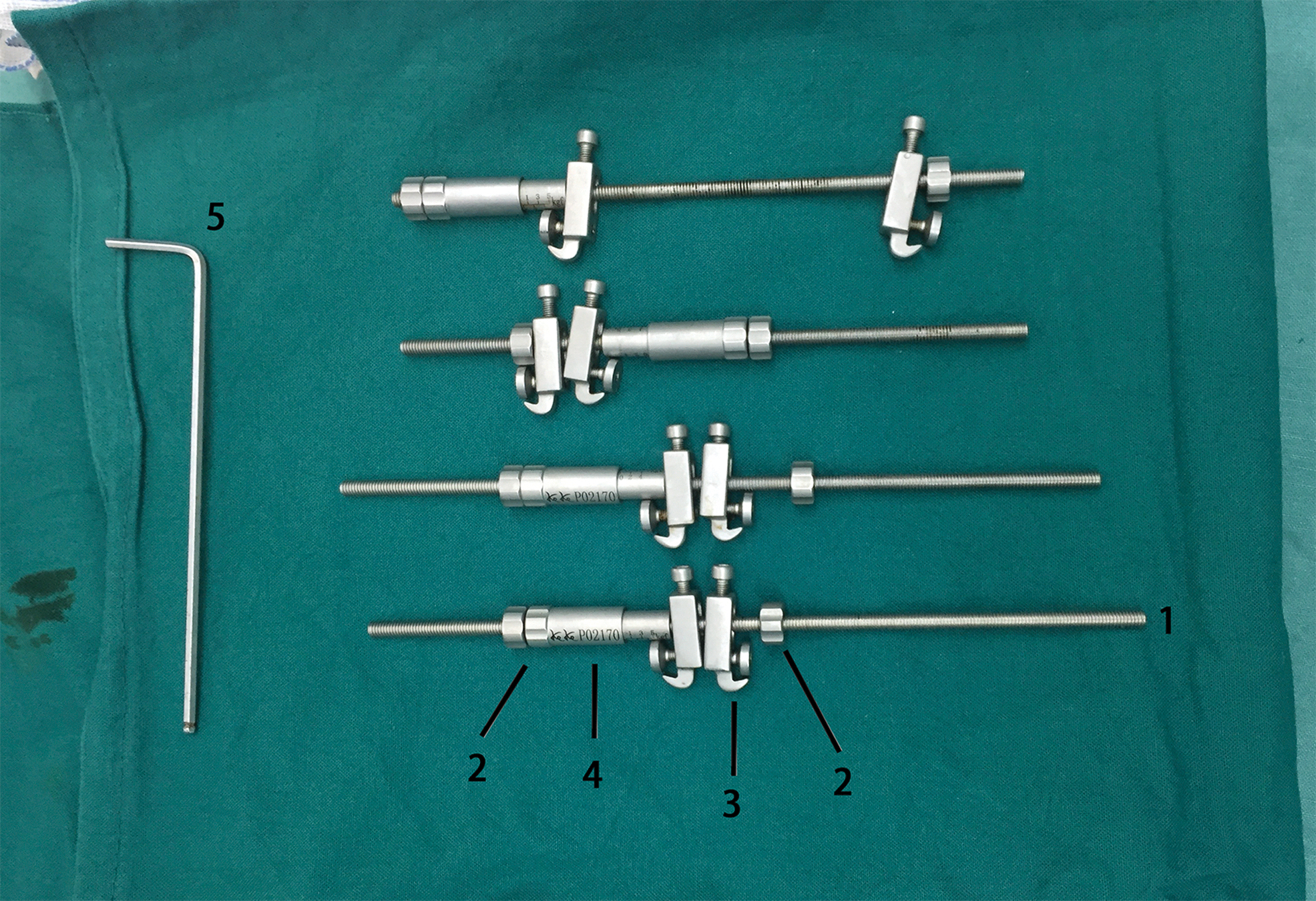
Modified skin-stretching device csomponents. 1: stainless steel shaft, 2: nut, 3: hook, 4: spring scale, and 5: the stabilizing wrench.
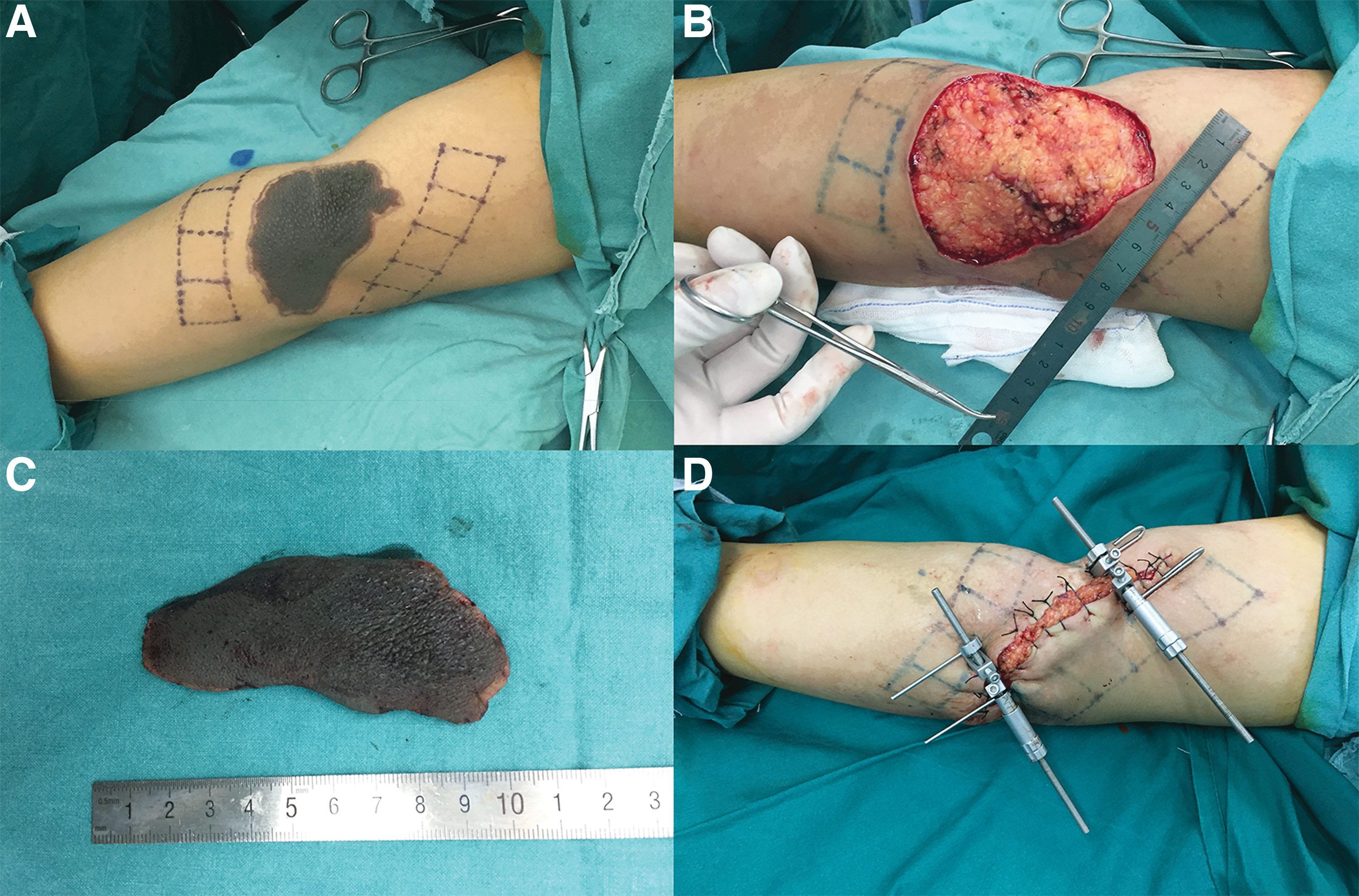
Before inserting the device, the skin flaps to each side of the defect were undermined at the suprafascial or subfascial plane to up to 5 cm from the wound edges. All the visible perforators (>0.3 mm size) were carefully preserved during the blunt dissection. Therefore, the skin paddle was partially elevated on a perforator-flap pattern ensuring an adequate skin perfusion. A 2-0 nylon suture was temporarily applied along the longitudinal axis to shrink the defect and reshape the defect into an oval size.
A pair of Kirschner wires (2.0 or 2.5 mm diameter) were inserted intradermally on each side along the longitudinal axis of the defect where the two ends pierced the skin surface and were bent at an oblique angle of 30°. Each Kirschner wire was placed at1.0–1.5 cm away from the edge of the defect. The device was then inserted to the exposed ends of the Kirschner wire, with the two hooks locked by a stabilizing wrench. The two nuts on the stainless steel shafts were used to adjust the tension across the shafts (Fig. 2A–D). For most of the cases, a single pair of Kirshner wires was sufficient. However, an additional pair of Kirshner wires was placed for a progressive skin stretching, if there was a strong tension after the primary closure. The soft tissue defect on the central area was carefully covered by silver-impregnated dressings.
(
Tissue stretching
The skin stretching was commonly started 24 hours postoperatively. The applied tension was usually determined based on the skin tissue properties such as color, temperature, and capillary refill. Normally, a constant tension of maximum 4 kg for adults, and 3 kg for children, was applied based on previous cases and other authors' recommendations using similar devices. 7 –10 The tension applied was reduced further for individual with comorbidities such as diabetes, or where the involved tissue had been previously incisioned or irradiated. The strength was adjusted by rolling the nuts with the parameter shown on the spring scale. The blood supply to the skin flaps was monitored every 2 hours by an experienced physician or nurse.
The tension was instantly reduced if the overlying skin appeared to be compromised. A handheld infrared thermal camera (FOTRIC® 228s; Thermal Intelligence, Shanghai, China) was utilized as an objective evaluation of skin vascularization (Fig. 3). 11 The palette was set on “Iron” mode, and the temperature threshold was adjusted from 25°C to 37°C. A difference less than 2° of skin temperature was considered safe to use on stretched skin and contralateral normal skin (Fig. 4).

Infrared themography device. The device was used for the evaluation of skin temperature.
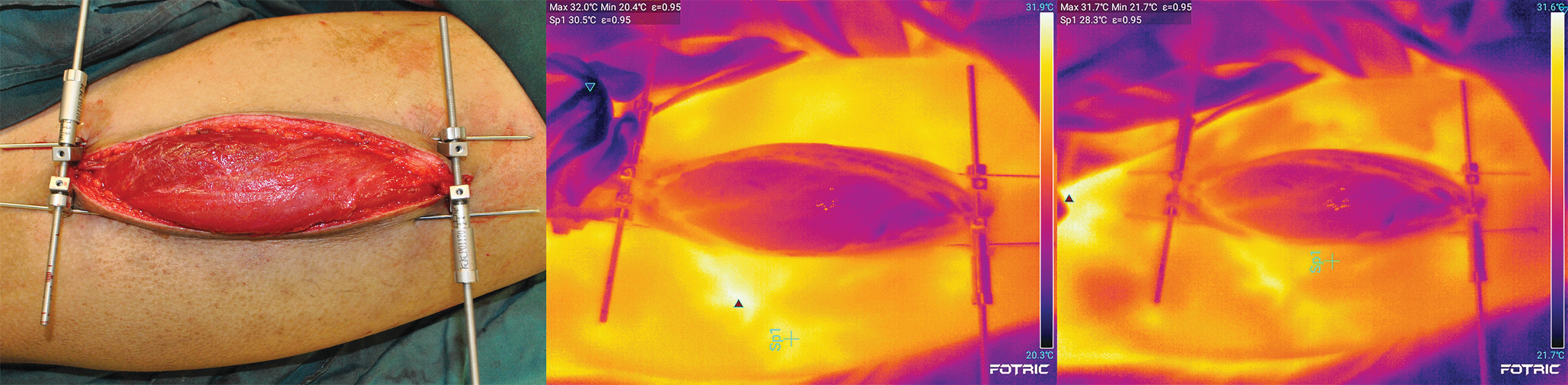
Using infrared themography for the evaluation of skin temperature. Left. The skin-stretching device was used for the closure of donor site after harvesting the anterolateral thigh flap. Middle, Right. The skin temperature of the wound edge and adjacent normal skin was evaluated by infrared themography. The temperature of adjacent normal skin was shown as 30.5° and the temperature of wound edge was shown as 28.3°.
After the tightened skin gradually became more elastic, the tension was subsequently increased up to 4 kg for five to eight times per day according to the assessment measured by the infrared thermography camera. The dressings were changed daily and the expansion was usually completed after 14 days. Commonly used analgesics such as Tramadol or Dezocine were prescribed.
Second stage
Once sufficient skin tissue was obtained, the wounds were closed under local or general anesthesia. The skin was closed by layers using 2/0 PDS, 4/0 Vicryl, and 5/0 Prolene, for the fascia, deep dermal, and epidermal layer, respectively. Suction drains were placed and removed when <30 mL/24 hour. The skin-stretching device and Kirshner wires were removed once the wound was closed.
Results
A total of 20 patients underwent modified skin-stretching technique. Surgical sites included forearm (n = 3), upper arm (n = 2), thigh (n = 2), lower leg (n = 7), trunk (n = 5), and dorsum of the foot (n = 1). The average skin defect size was 107.7 cm2, ranging from 8 × 5 to 19 × 16 cm. One patient developed a small wound dehiscence, which was managed conservatively with dressings. One patient developed early symptoms of forearm compartment syndrome, which recovered with temporary release of tension. Two patients who underwent abdominal wall reconstruction for metastatic bowel cancer passed away at 1 month after the delayed primary closure due to multiorgan failure caused by their metastatic disease.
The patients were followed up for 3–6 months. Laser treatment was offered to all patients for scar management. 12,13 All the patients were satisfied with their esthetic outcomes.
Representative case series
Case 1
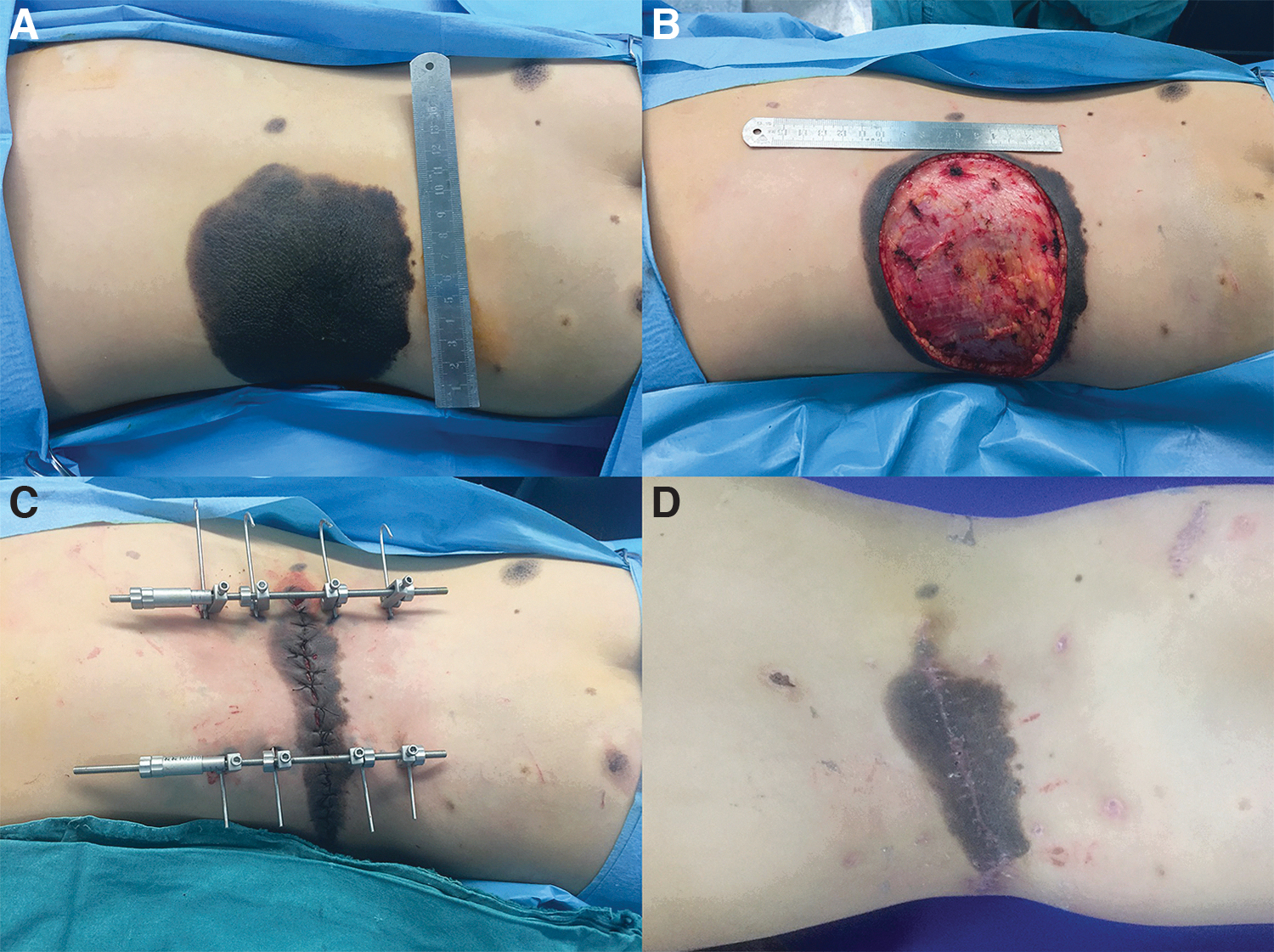
A 12-year-old girl presented with a giant congenital melanocytic nevus (14 × 10 cm) involving her lateral and posterior trunk (Fig. 5A). Traditional tissue expander was not a feasible option due to the patient and parents' preference. It was decided that an external skin-stretching device would be used to maximize the portion of the nevus that could be resected in one operation. After resecting most of the nevus (Fig. 5B), we undermined the surrounding area, preserving all perforators, and applied the skin-stretching device as described above (Fig. 5C). After 14 days of expansion, the skin-stretching device was removed and the skin flaps were sutured by layers. A satisfactory outcome was observed at 3 months postoperatively (Fig. 5D). Further excision will be carried out in the near future.
Case 2
A 28-year-old young man had a traumatic skin loss over the left leg. The skin defect size was 20 × 6 cm (Fig. 6A), which was not amenable for primary closure. After a radical debridement and tissue undermining were performed, the skin-stretching device was applied to the wound (Fig. 6B). After 14 days of expansion, the wound was primarily closed without the need of skin grafts (Fig. 6C). The final result at 3 months was excellent (Fig. 6D).

Case 3
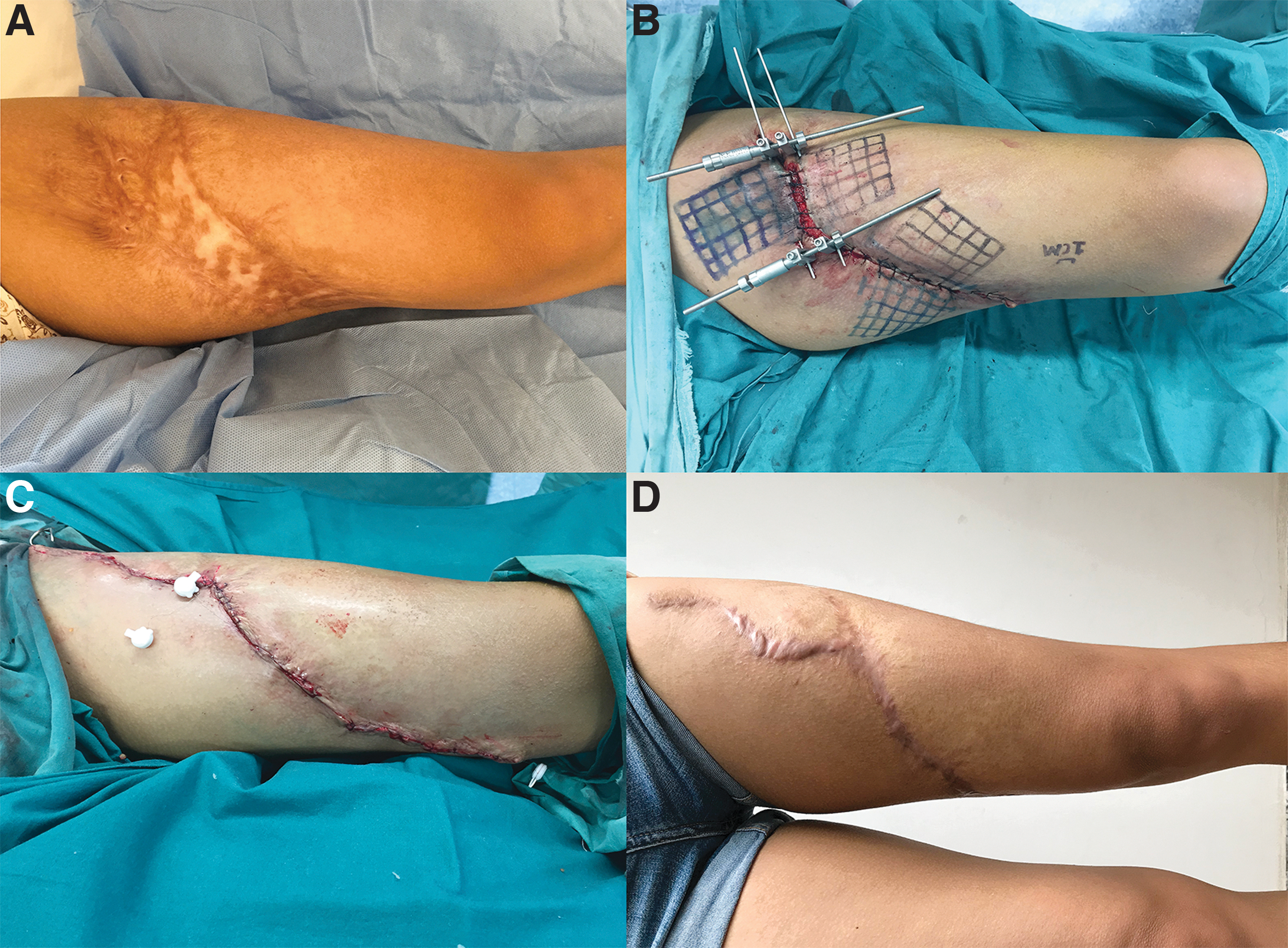
A 20-year-old woman presented with a burn scar on her left thigh, which was sustained at the age of 3 years (Fig. 7A). After resection of the scar, the defect measured 20 × 8 cm. Moderate undermining was performed under the deep fascia layer at the margins of the defect. All visible perforators (caliber >0.3 mm) were carefully dissected and preserved during the blunt dissection. The external skin-stretching device was then applied (Fig. 7B). After stretching for a period of 14 days, the skin flap was able to be closed primarily (Fig. 7C). The result at the 6-month follow-up was excellent (Fig. 7D).
Case 4
A malnourished 59-year-old man with multiple comorbidities presented with a recurrence of mucinous colorectal adenocarcinoma and peritoneal metastases (Fig. 8A). The patient underwent an adhesiolysis, a colorectal resection, and anastomosis performed by general surgeons (Fig. 8B) with a subsequent postoperative abdominal wall defect measuring 20 × 15 cm (Fig. 8C).
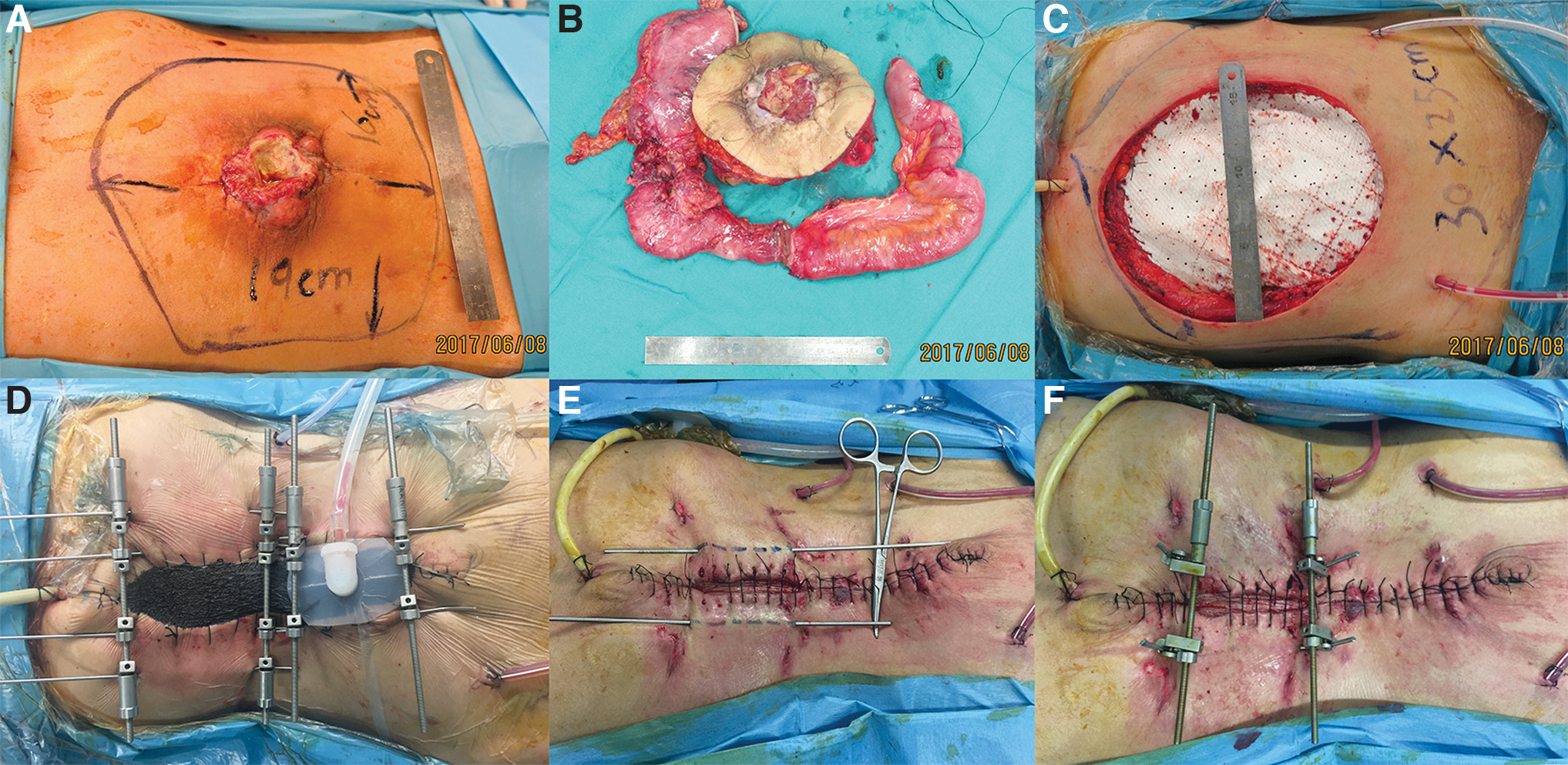
Due to the patient's comorbidities and previous abdominal scars, we opted to perform a two-sequential skin-stretching technique and negative pressure dressings to achieve a delayed primary closure (Fig. 8D), instead of using traditional techniques to close the defect such as abdominal component separation or local/free flap reconstruction.
After 14 days of expansion, extra additional tissue was gained. However, this volume was not sufficient to achieve a primary closure. Therefore, the “double pattern” sequential stretching devices were converted into a single skin-stretching device under local anesthetic and followed by a further cycle of expansion before achieving a primary closure (Fig. 8E, F). Unfortunately, the patient died 1 month after the wound closure due to multiorgan failure related to his metastatic colorectal cancer.
Discussion
When it is not possible to perform a direct closure, there are currently several surgical options available such as free flaps or skin grafts to cover moderate to extended skin defects. 14,15 However, for Asian patients, the significant risk of developing a hypertrophic or keloid scar, drives us to reconsider treatment options to achieve the best postoperative results for the recipient and donor sites. 16,17 Most frequently, free flaps provide an ideal tissue with adequate volume for functional or esthetic reconstructions. 14,18 However, these surgical operations require microsurgical techniques, long recovery time alongside cautious postoperational monitoring, which leave obvious scars at the donor site. 16 –19
Skin grafts offer a less-than-ideal outcome for skin defect coverage with a relatively simple technique, while resulting in a relatively severe donor site morbidity. 20,21 Tissue expansion is a valuable technique as it provides “like with like” tissue to reconstruct defects and offers excellent esthetic result in terms of a color and texture match. 22,23 Furthermore, skin expansion avoids additional donor site morbidity, reducing the risk of hypertrophic scars and keloids, especially in the Asian population. However, traditional internal tissue expansion requires a long time, usually several months to produce an adequate volume of tissue, which may be inconvenient for patients due to multiple visits for injections into the expander. 23
Since Barrer et al. 6 reported his novel retention-bridging device as an external expansion instrument in 1976, a number of external skin-stretching devices became commercially available. SUTUREGARD®, Miami STAR, Sureclosure, TopClosure, and Canica Wound Closure System® were developed according to the biomechanical properties of skin tissue, while being different from each other in certain details. 7 –10,24 –27 SUTUREGARD similarly takes advantage of the retention sutures under high tension without damage of underlying tissue. 24,25 The Miami STAR gathered up the slack skin and closed the defect by leaning the progressive tension on the sutures penetrating the skin. 9 The skin would be finally cut tangentially if the defect measured large. Sureclosure was first introduced in 1993 and was widely used. 10
However, when an increasing tension was exerted on the device, the hooks tend to slip and torque. Furthermore, the hooks that ploughed through the subcutaneous tissues were found to halt the skin-stretching process. Cin and Seal 26 first introduced Canica Wound Closure System in 2006, followed by Topaz et al. 27 who described the TopClosure 3S System in 2012. These two products require placement of multiple anchoring plates along the wound edges, and thus has been found to cause significant pigmentation and hypertrophic scars along the wound edges in Asian patients.
The modified skin-stretching technique (KeKe) innovatively utilized intradermal Kirschner wires with external fixation hooks to stabilize the device. Compared to the above-mentioned devices, the tension formed during skin-stretching process could be linearly distributed along the entire K-wire instead of being delivered to just a number of stretched points. Consequently, in this study, a relatively slighter force was carried out per unit area; therefore, none of the skin paddles was damaged by the stretching. Furthermore, only two residual scars resulted at the end of each Kirschner wire.
Considering the already published external skin-stretching techniques, 9,10 we modified the technique by performing a moderate undermining of the adjacent skin flaps, while preserving all visible perforators. Before the angiosome and perforasome theories were thoroughly investigated by Taylor 28 and Saint-Cyr et al., 29 the viability of skin was deemed compromised as the undermining procedure entailed cutting feeding vessels inevitably. However, we found it reliable when the perforators were carefully preserved during the undermining process in a perforator-flap style. This procedure provided a robust blood supply by preserving perforators that originated from the underlying main vessels, and allowed maximal skin advancement after device placement.
The undermined skin paddle enhanced the tissue “creep,” promoting an extremely shortening time of the stretching period. The expansion was completed within 14 days for the majority of the cases and the application of the skin-stretching device was found simple to use with minimal assembly time required for each case. Compared with similar products, 7 –10,24 –27 the modified external skin-stretching technique was found to better distribute the tension along the wound by adjusting the placement of the Kirschner wire. However, during the early phase of the study, one patient developed a wound dehiscence around the elbow joint that was healed by secondary intention, applying traditional dressings at the outpatient clinic. This complication can be the result of an overwhelming perpendicular tension applied to the wound.
Although 15 N is indicated as the maximum force applicable on scalp wounds, the relevant force on different areas such as trunk and limbs needs further investigations. 30 Therefore, to avoid possible wound dehiscence, the biodynamic excisional skin tension lines concept was adopted in majority of the cases. 31 However, this principle was not applied for a few patients when an extensive skin defect was present (e.g., the case 4). Although “Best lines” on the trunk run in the horizontal direction, the extremely large defect of the abdominal region cannot be closed by simply stretching the adjacent skin tissues from the cranial to caudal side. Therefore, a vertical excision was carried out using the extra skin laxity of the lumbar area. 32 In general, wounds were closed taking into account the way the wound lies following excision. Relaxed skin tension lines were used as a guide rather than a rule. 33
In a two-stage procedure with delayed primary closure, the local tissue can be recruited over a shorter period of time with minimal donor site morbidity. Therefore, it is preferable to address a patient with multiple comorbidities to a simple and safer two-stage surgical procedure with relatively shorter operating time rather than a more complex and longer single-stage operation under general anesthesia for microsurgical free tissue transfer. The external tissue-stretching technique may offer a useful alterative in patients with such indications. However, caution should be taken during the expansion process where an overwhelmed tension should be always avoided.
In previous studies, Hirshowitz et al. 10 recommended a force by the device ranged from 0.5 to 3 kg. Mingli et al. 34 applied a maximum traction force of 6 kg for his external expansion cases. Topaz et al. 35 suggested a maximal overstretching load of 3 kg. As there is no general consensus, this criterion still remains controversial. Previous incisions/scarring, radiation, and diabetes can increase the risk of ischemia. Therefore, a constant monitoring of the skin-stretching forces was applied to evaluate the skin circulation by an infrared thermography camera. The skin temperature was assessed and a difference less than 2° was considered safe when compared to the adjacent normal skin. The evaluation of the skin tissue with the infrared thermography camera can be easily estimated by simple training of the device. 11
For extensive abdominal wall defects with a delayed primary closure, in addition to a “double pattern” sequential skin-stretching technique, an adjuvant negative pressure dressing (Kulavac®; BioAlpha, Inc., Korea) was applied as in Case 4. Two stretching devices were placed oriented perpendicular to the longitudinal axis of the defect to better distribute the tension in skin stretching. With more cutaneous tissue enrolled by the two paralleled skin-stretching devices, mechanical creep was better facilitated for the sake of wound closure. Meanwhile, the negative pressure system synergistically contracted the wound, promoting vascularization and granulation tissue formation, and facilitated the wound drainage. 36 –38
The plastic drape was placed before inserting the stretching device to ensure that negative pressure was maintained (Fig. 8D). However, the “double pattern” skin-stretching technique was not applied for the same defect size of the upper or lower extremities due to the less skin volume size and shape of the location.
With the skin-stretching technique, we obtained both stress tension relaxation and mechanical creep, therefore achieving a delayed primary closure for moderate and extended skin defects with an adjacent skin matching color, texture, and thickness. The technique not required a weekly saline injection or microsurgical skills, with the treatment's time lasted less than conventional tissue expander (usually 3–6 months). The modified external skin-stretching technique included the following: The use of intradermal K-wires for a linearly even tension distribution during tissue stretching. A moderate undermining of the adjacent skin to preserve all visible perforators. The monitoring of skin temperature to evaluate the skin perfusion where a difference less than 2° was considered safe in case of overstretching. The “Double pattern” sequential skin-stretching technique was experimentally adopted for the closure of extensive abdominal wall defects.
There are a few limitations of this technique. The device is not suitable for scalp defects due to the convexity of the scalp that limits the application of the Kirschner wires. Furthermore, the Kirschner wire pin site can cause a sinus tract or a hypertrophic/keloid scar, which may require a debridement or laser treatment. 17,39,40 Skin defects of the chest or abdominal wall may result in an increased respiratory effort; therefore, patients are requested to practice a compensated breathing pattern to minimize the impact on their respiratory function. Moreover, when this technique is applied to lower or upper limbs, it is important to carefully monitor and promptly identify a potential compartment syndrome.
One of the patients in this study developed early symptoms of compartment syndrome, which required a temporary release of the tension and a subsequent retightening with a 4-hour interval time, and no further issues developed. Therefore, accurate postoperative cares are essential.
Conclusion
The modified external skin-stretching technique obtained both stress relaxation and mechanical creep, therefore achieving a successfully delayed primary closure for moderate to extensive skin defects and providing a like-with-like reconstruction. We propose this technique as a useful option to cover large and complex trunk or limb defects. Our outcomes indicate that it is a safe, reliable, and effective method to cover such soft tissue defects with minimal complication rates when appropriately applied and utilized.
Footnotes
Acknowledgments
We thank Dr. Fabio Nicoli (Newcastle University—Northumbria NHS Trust, United Kingdom) for comments on the article.
Ethics Approval and Consent to Participate
This study is considered exempt from institutional review board approval since the data were collected retrospectively. Informed consent was obtained from all the patients.
Consent for Publication
All patients provided written informed consent for publication of pictures and personal data.
Availability of Data and Materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (No. 81801918 and No. 81772098).