
Abstract
Duchenne muscular dystrophy (DMD) is a lethal X-linked disorder caused by mutations in dystrophin gene. Currently, there is no cure for DMD. Cell therapies are challenged by limited engraftment and rejection. Thus, more effective and safer therapeutic approaches are needed for DMD. We previously reported increased dystrophin expression correlating with improved function after transplantation of dystrophin expressing chimeric (DEC) cells of myoblast origin in the mdx mouse models of DMD. This study established new DEC cell line of myoblasts and mesenchymal stem cells (MSC) origin and tested its efficacy and therapeutic potential in mdx/scid mouse model of DMD. Fifteen ex vivo cell fusions of allogenic human myoblast [normal myoblasts (MBN)] and normal human bone marrow-derived MSC (MSCN) from normal donors were performed using polyethylene glycol. Flow cytometry, confocal microscopy, polymerase chain reaction (PCR)-short tandem repeats, polymerase chain reaction-reverse sequence-specific oligonucleotide probe assessed chimeric state of fused MBN/MSCN DEC cells, whereas Comet assay assessed fusion procedure safety testing genotoxicity. Immunofluorescence and real-time PCR assessed dystrophin expression and myogenic differentiation. Mixed lymphocyte reaction (MLR) evaluated DEC's immunogenicity. To test MBN/MSCN DEC efficacy in vivo, gastrocnemius muscle of mdx/scid mice were injected with vehicle (n = 12), nonfused MBN and MSCN (n = 9, 0.25 × 106/each) or MBN/MSCN DEC (n = 9, 0.5 × 106). Animals were evaluated for 90 days using ex vivo and in vivo muscle strength tests. Histology and immunofluorescence staining assessed dystrophin expression, centrally nucleated fibers and scar tissue formation. Post-fusion, MBN/MSCN DEC chimeric state, myogenic differentiation, and dystrophin expression were confirmed. MLR reveled reduced DEC's immune response compared with controls (P < 0.05). At 90 days post-DEC transplant, increase in dystrophin expression (20.26% ± 2.5%, P < 0.05) correlated with improved muscle strength and function in mdx/scid mice. The created human MBN/MSCN DEC cell line introduces novel therapeutic approach combining myogenic and immunomodulatory properties of MB and MSC, and as such may open a universal approach for muscle regeneration in DMD.
Introduction
Duchenne Muscular Dystrophy (DMD) is a lethal X-linked progressive disease of skeletal and cardiac muscles characterized by lack of functional dystrophin [1 –3], which is critical anchor protein between the subsarcolemmal cytoskeleton and extracellular matrix [4,5]. Lack of dystrophin leads to muscle degeneration and loss of function. Currently, there is no cure for DMD.
Transplantation of allogenic myoblast or satellite cells showed negligible functional improvements [2,3] due to early massive loss of transplanted cells [4 –7].
During the past two decades, research reports emphasized that ideal donor cell for skeletal muscle regeneration should be easily accessible, able to expand, engraft, preserve myogenic phenotype, and high survival rate. Low immunogenic profile is also critical for long-term engraftment without the need for immunosuppressive therapy. Recent studies applying genetically modified autologous myoblasts [8] and highly proliferative stem cell populations [3,9 –11] received attention; however, their routine clinical applications are unclear due to safety concern of the fate of genetically modified cells, including off-target mutations, sensitization, and potential carcinogenic transformation [2,12,13].
To develop a novel cell-based therapies with unique prerequisites, including a low immune profile and tolerogenic properties, we applied our ex vivo cell fusion technology, which was established for creation of chimeric cells of hematopoietic, mesenchymal, and myoblast stem cell lineages. [14 –18]. We adopted fusion protocol concept for muscle regeneration applicable to DMD, and developed dystrophin expressing chimeric (DEC) cells by fusion of normal myoblasts (MBN) with myoblasts from the DMD affected donors. We confirmed feasibility and efficacy of fusion that correlated with dystrophin expression, and improvement of muscle function after DEC transplant to mdx and mdx/scid mouse models of DMD [14,17].
To further assess regenerative potential of chimeric cells in DMD, we searched for different parent cell candidates with regenerative and immunomodulatory properties to create new DEC lines. Owing to immunomodulatory and anti-inflammatory characteristics, mesenchymal stem cells (MSC) were considered as attractive cell population tested in stem cell-based therapies [5,19 –26]. Autologous MSC are applied in clinical trials for treatment of chronic inflammatory and degenerative diseases, including DMD [27,28]. Moreover, MSC have shown a myogenic potential after differentiation to myoblasts [29]. Thus, based on the reported regenerative and immunomodulatory qualities of MSC and clinical reports, we have chosen MSC as an optimal parent cell candidate to create a new generation of DEC cells of myoblasts and MSC origin.
In this study, we confirmed creation of new human MBN/normal human bone marrow-derived MSC (MSCN) DEC cell line of myoblasts—MBN and MSCN originating from normal human donors. In vitro, we characterized the phenotype, genotype, and proliferative potential of parent and DEC cells, whereas in vivo, long-term engraftment and increased dystrophin expression correlated with improved function and reduced allogenic immune response at 90 days post-DEC transplant to mdx/scid mouse. This study introduces human DEC (MBN/MSCN) as novel therapeutic approach combining myogenic and immunomodulatory properties of MB and MSC for muscle regeneration in DMD.
Materials and Methods
Experimental animals
University of Illinois at Chicago Institutional Animal Care and Use Committee approved animal care and experimental protocols. Six- to eight-week-old mdx/scid mice (B10ScSn.Cg-Prkdcscid Dmd mdx /J) with respective background wild-type mice (C57BL/10ScSnJ) were purchased from Jackson Laboratories.
Ex vivo creation of human DEC cells
Human myoblast culture
MBN (Lonza, Inc.) were cultured in skeletal myoblast growth medium SkGM (SkGM-2; Lonza, Inc.) supplemented with human epidermal growth factor, Fetuin, 5 mL bovine serum albumin, 5 mL dexamethasone, 0.5 mL insulin, 5 mL gentamicin/amphotericin-B, 0.5 mL. Upon reaching 60%–70% confluence, MB were harvested [0.25% trypsin-ethylenediaminetetraaceticacid (EDTA); Gibco-Thermo Fisher Scientific] between passages 5 and 7.
Human MSC culture
MSCN (Lonza, Inc.) were cultured in MSC growth media (Lonza, Inc.), supplemented with MSC growth supplement,
Cell fusion procedure
Fifteen human MBN/MSCN DEC fusions were performed as previously reported [14,17]. In brief, after harvesting, parent MBN and MSCN were fluorescently labeled using either PKH26 or PKH67 dyes (Paul Karl Horan dye-PKH, Sigma Aldrich) according to manufacturer's instruction. Fusion was performed using 1.46 g/mL polyethylene glycol (PEG) solution (PEG 4000; EMD), containing 16% dimethyl sulfoxide (Sigma). Next, fused cells were transferred to Dulbecco's phosphate-buffered saline (DPBS)-based sorting buffer containing 5% HEPES, 1% EDTA, and 1% fetal bovine serum. Finally, cells presenting double PKH26/PKH67 staining were sorted through fluorescence-activated cell sorting (MoFlow Astrios; Beckman Coulter) and used for in vitro and in vivo analysis. The viability of MBN, MSCN and MBN/MSCN DEC was assessed at each stage of fusion procedure using 0.4% Trypan Blue staining solution as previously reported [14,17,30].
Flow cytometry and confocal microscopy analysis for confirmation of DEC fusion
Samples of sorted PKH26/PKH67 labeled DEC and corresponding single-stained and unstained controls were fixed in 4% paraformaldehyde and analyzed using Fortessa flow cytometer (Becton Dickinson). For confocal microscopy cells were spun onto positively charged lysine coated slides, counterstained with 4′,6-diamidino-2-phenylindole (DAPI; Vector Laboratories), examined on Zeiss Meta confocal microscope and analyzed with ZEN software (Zeiss).
Genotype analysis polymerase chain reaction-short tandem repeats and polymerase chain reaction-reverse sequence-specific oligonucleotide probe DNA profiling
Polymerase chain reaction-short tandem repeats (PCR-STR) and polymerase chain reaction-reverse sequence-specific oligonucleotide probe (PCR-rSSOP) profiled DNA samples of parent MBN and MSCN and MBN/MSCN DEC, as previously reported [17]. The 10 studied STR loci included TH01, D21S11, D5S818, D13S317, D7S820, D16S539, CFS1PO, Amelogenin, vWA, and TPOX. The raw data were uploaded to GeneMapper® 5.0 analysis software (Applied Biosystems) to create allelic profile(s).
For PCR-rSSOP, samples were typed for HLA-A, -B, -Cw, -Bw, -DR, -DQ, -DR52/DR53 (LABtype rSSO Typing Test, OLI). Fluorescence signals were identified by Luminex 200 (Luminex), and the HLA typing was obtained from the HLA Tools software.
The single cell gel electrophoresis assay (Comet assay)
The alkaline single cell gel electrophoresis (SCGE) was performed according to the manufacturer (Cell Biolabs, Inc.) instructions. In brief, samples of Paul Karl Horan dye (PKH) labeled MBN and MSCN and DEC were resuspended at 1 × 105 cells/mL in DPBS and mixed with Comet Agarose at 1:10 ratio (v/v), immediately layered onto microscopy slides. After standard single cell electrophoresis, DNA was visualized using Vista Green dye (1:10,000) and samples were examined using LSM 710 fluorescence microscope Meta (Zeiss). The DNA damage was assessed by visual presence of the comet tail.
Quantification of dystrophin expression by Taqman real-time PCR
Total RNA was isolated from cells as previously reported [17] and 600 ng/μL of total RNA was reverse-transcribed to cDNA in a total volume of 20 μL, using High Capacity cDNA Reverse Transcription Kit (Applied Biosystem). Quantitative assessment of dystrophin expression (Hs00758098_m1) was performed using the 7300 Real-Time PCR detection system with 7300 System SDS software (Applied Biosystem). Amplification was carried out in TaqMan Universal PCR Master Mix (2 × ), and Gene Expression Assay Mix (20 × ) [17]. Expression of all examined genes was compared with endogenous controls of Gapdh (Hs99999905_m1; Applied Biosystem).
Immunofluorescence detection and quantification of dystrophin in vitro
MBN/MSCN DEC (n = 4 fusions/line) and parent MBN and MSCN cells (n = 4/cell type) were cultured in a SkGM-2 Medium on poly-
Myogenic differentiation of MBN/MSCN DEC
MBN/MSCN DEC (n = 4 fusion) and controls of MBN and MSCN were cultured on poly-
Mixed lymphocyte reaction
Mixed lymphocyte reaction (MLR) assessed immunomodulatory properties of MBN/MSCN DEC. The responder peripheral blood mononuclear cells (PBMC), derived from the same donor as the DEC's parent MSCN (Lonza, Inc.), were stained with Cell Proliferation Dye eFluor 670 (Thermo Fisher Scientific) and cultured in media, or cocultured with third-party allogeneic T cells, with MBN, or MSCN that represented DEC parent cells, or with fused MBN/MSCN DEC cells. Responder PBMC (T cells) were activated with irradiated third-party allogeneic T cells derived from PBMC and served as positive controls. After 4 days of culture, cells were collected and proliferation rate was analyzed by flow cytometry (Gallios; Beckman Coulter).
Transplant of MBN/MSCN DEC
MBN/MSCN DECs were suspended in 60 μL of DPBS in tuberculin syringe with 27G needle (Thermo Fisher Scientific). Under 1.5% isofluorane anesthesia, skin on left posterior mice calf was prepared. Based on template, six microinjections were delivered into gastrocnemius muscle (GM) [14,17].
After randomization of age-matched 6–8 weeks old mdx/scid mice were assigned to experimental groups: vehicle control (n = 12, 60 μL DPBS), nonfused MBN and MSCN (n = 9, 0.25 × 106/donor- total 0.5 × 106 in 60 μL DPBS), MBN/MSCN DEC (n = 9, 0.5 × 106 in 60 μL DPBS). Animals were followed up for 90 days and in vivo and ex vivo muscle strength tests were performed.
Histology and immunofluorescence analysis
Paraffin embedded GM were cut at 5-μm sections, stained with hematoxylin and eosin (H&E) to analyze muscle structure and quantify centrally nucleated fibers (CNF). Five standardized ROI of three nonserial cross sections for a total of 15 ROI of n = 3/group were analyzed for CNF and normalized to total nuclei number.
Frozen GM samples were cut at 4
Muscle strength evaluation
Wire hanging and grip strength test
Mice motor function was monitored up to 90-day endpoint; wire hanging test and modified grip strength test were performed as previously reported [14,17]. Wire hanging muscle force assessed general muscle strength of the MBN/MSCN DEC-injected mice versus controls. Using grip meter (Digital Force Gauge, HL-50), a modified grip strength test for posterior limbs was used to measure GM-specific force [31,32].
In situ muscle force test
In situ muscle force measurements were performed under isoflurane anesthesia at 90-day endpoint as previously reported [17]. In brief, sciatic nerve was isolated and stimulated with a bipolar electrode. Muscle force was measured after optimal voltage and length were determined. Fatigue was measured after 10 min of submaximal tetanic stimulation as described previously [33].
Ex vivo muscle force test
After euthanasia, the contractile and passive properties of GM were measured ex vivo using Aurora Scientific ex vivo muscle test system [31]. After dissection GM was placed in a Radnoti glass chamber tissue bath. The Achilles tendon and proximal pole of muscles were attached to force transducer. Muscle force was measured through a standardized stimuli pattern until reaching maximal wave and maximal strain.
Statistical analysis
Data are presented as mean ± standard deviation. OriginPro 2017 were used for statistical analyses. Differences between respective groups were assessed using Student's t-test. P values were considered significant below 0.05.
Results
Confirmation of human MBN/MSCN DEC line creation
New human DEC cell line was created from MBN and MSCN as a clinically relevant concept of fusion (Fig. 1A). Flow cytometry revealed heterologous cell fusion (Fig. 1B), and confocal microscopy confirmed a chimeric state of DEC by presence of overlapping fluorescence images (PKH26/PKH67) (Fig. 1C). Analysis of DEC's genotype by STR-PCR (Fig. 1D) and rSSOP-PCR (Fig. 1E) confirmed presence of loci and alleles specific for each parent cell of myoblasts and MSC donor origin.
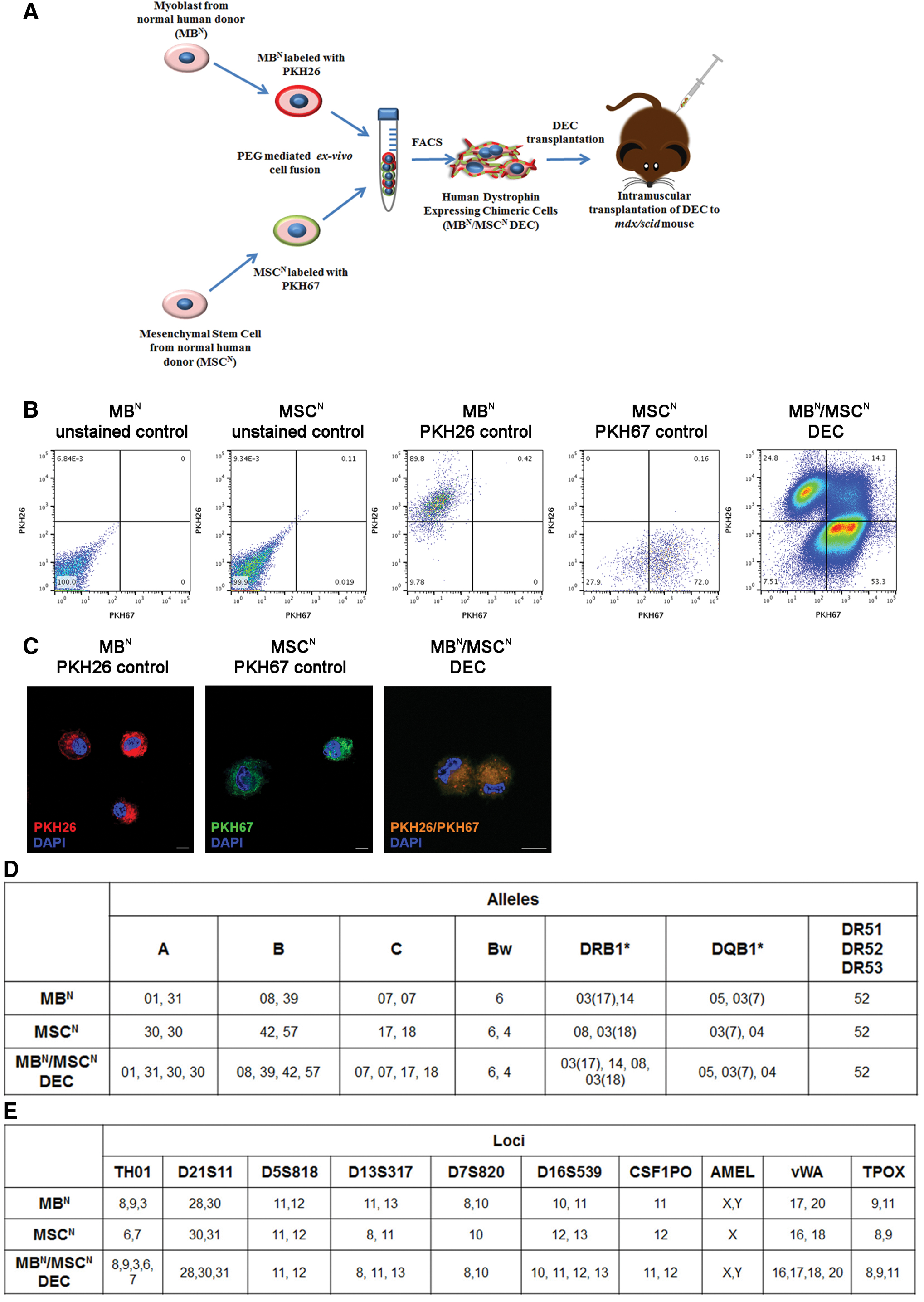
Confirmation of ex vivo creation of DEC cell line derived from normal donor's myoblasts (MBN) and normal donor's MSCs (MSCN).
In vitro confirmation of MBN/MSCN DEC safety after fusion
The SCGE assay confirmed lack of genotoxic properties of fusion procedure. No DNA damage was observed in PKH labeled MBN or MSCN donor cells and MBN/MSCN DEC (Fig. 2).
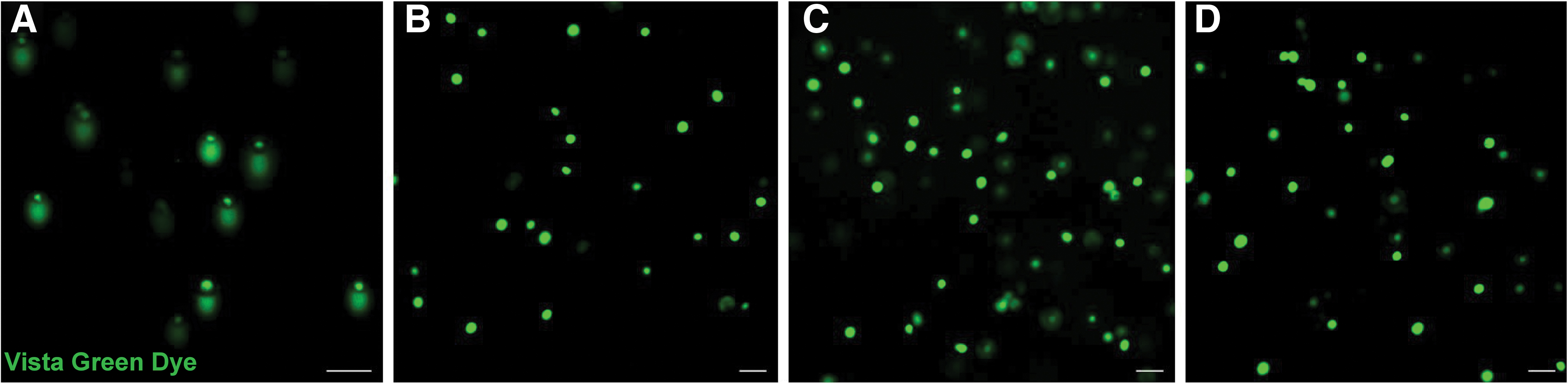
Confirmation of safety and lack of genotoxicity of ex vivo cell fusion protocol applied for creation of MBN/MSCN DEC cell line using the SCGE (COMET) assay.
In vitro confirmation of dystrophin expression after MBN/MSCN DEC fusion
To evaluate therapeutic potential of DEC in vitro, dystrophin expression was detected by immunofluorescence in DEC cell line up to 21 days after fusion (Fig. 3A). Dystrophin expression in cultured DEC was confirmed by quantification of immunofluorescence intensity on images acquired by confocal microscope (Fig. 3A), and by real-time PCR (Fig. 3B). Dystrophin expression was the highest at day 1 postfusion on confocal images, whereas real-time PCR showed highest expression at day 14 postfusion.
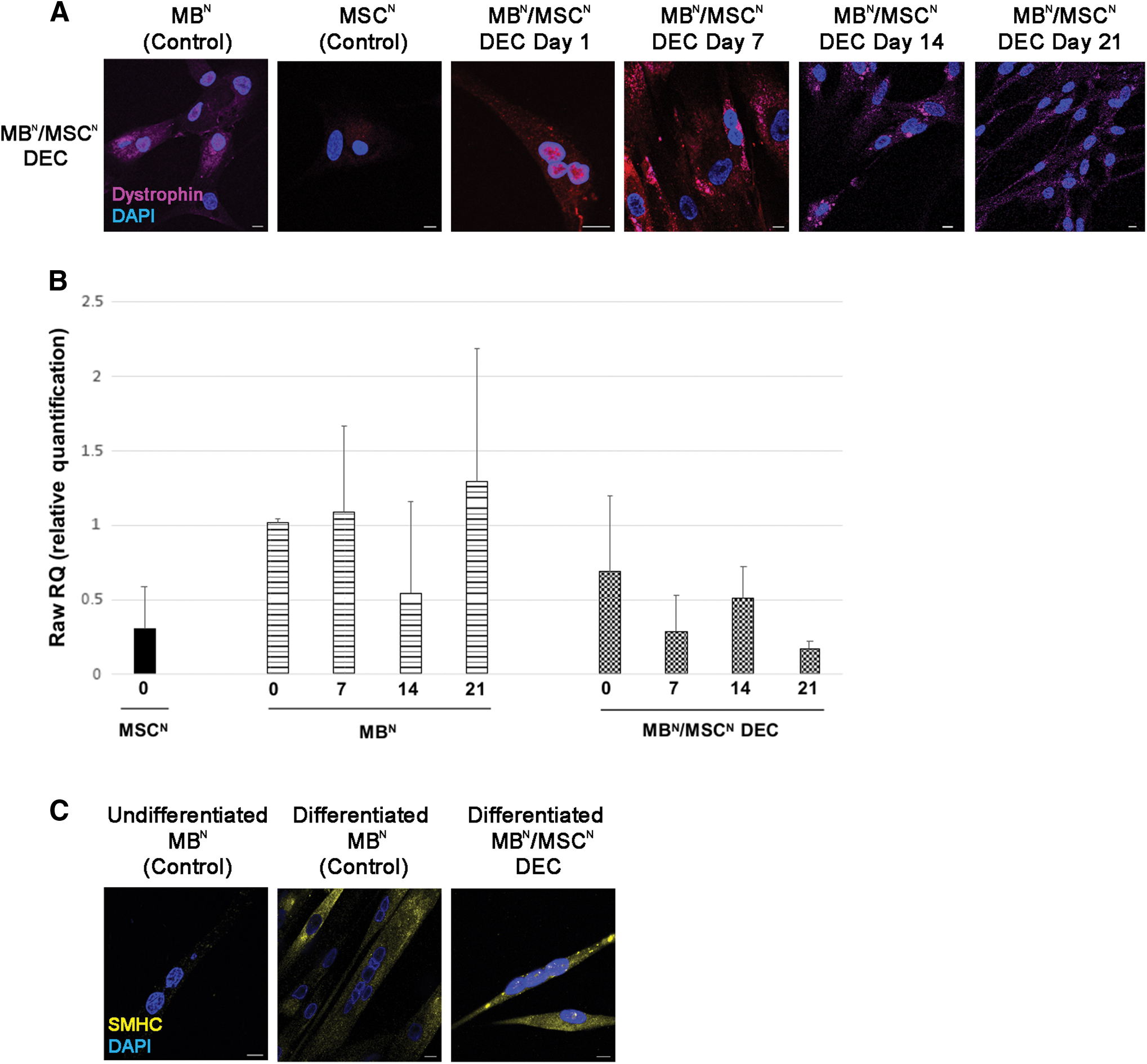
In vitro characterization of MBN/MSCN DEC.
Confirmation of myogenic differentiation after MBN/MSCN DEC fusion
A 7-day culture of MBN/MSCN DEC in myogenic differentiation medium revealed maintenance of DEC's myogenic differentiation potential as confirmed by co-expression of SMHC and dystrophin (Fig. 3C).
Confirmation of reduced alloreactivity of MBN/MSCN DEC by MLR
MLR assessed immunogenic properties of MBN/MSCN DEC. As expected, medium (negative control) and autologous MSCN showed low-level proliferation of responder PBMC-derived T cells (0.6% ± 0.05%, 1.74% ± 1.21%, respectively). The proliferation rate of responder T cell after stimulation with MBN/MSCN DEC was significantly lower (5.50% ± 2.85%, Stimulation Index [SI] = 3.16, P < 0.05) compared with response to third-party allogenic T cells (positive control, 54% ± 7%, SI = 31.03, P < 0.05), or to allogenic MBN (10.23% ± 2.11%, SI = 5.88, P < 0.05). This confirmed decreased immunogenicity of MBN/MSCN DEC and thus, pro-tolerogenic profile of the DEC cell line (Fig. 4).
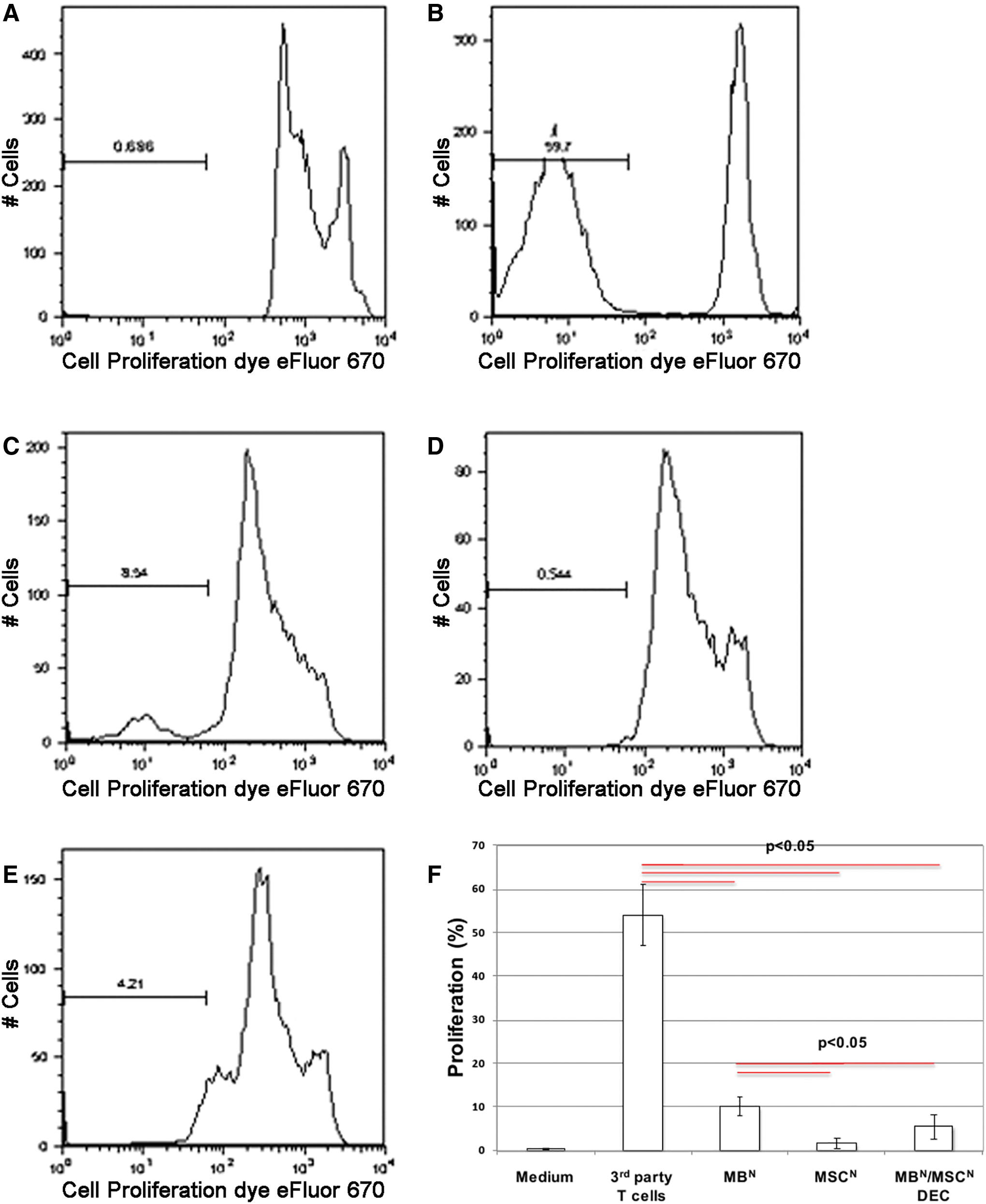
Immunogenic characteristics of MBN/MSCN DEC.
Confirmation of MBN/MSCN DEC engraftment and dystrophin expression in vivo at 90 days after DEC transplant
Immunofluorescence confirmed early (7 days) and long-term (90 days) engraftment and dystrophin expression in MBN/MSCN DEC-injected GM compared with vehicle-injected mdx/scid controls (Fig. 5A). Restoration of dystrophin expression after DEC transplantation was confirmed by immunofluorescence, and human origin of dystrophin was confirmed by co-localization with HLA-ABC in the GM of DEC-injected mdx/scid mice (Fig. 5A).
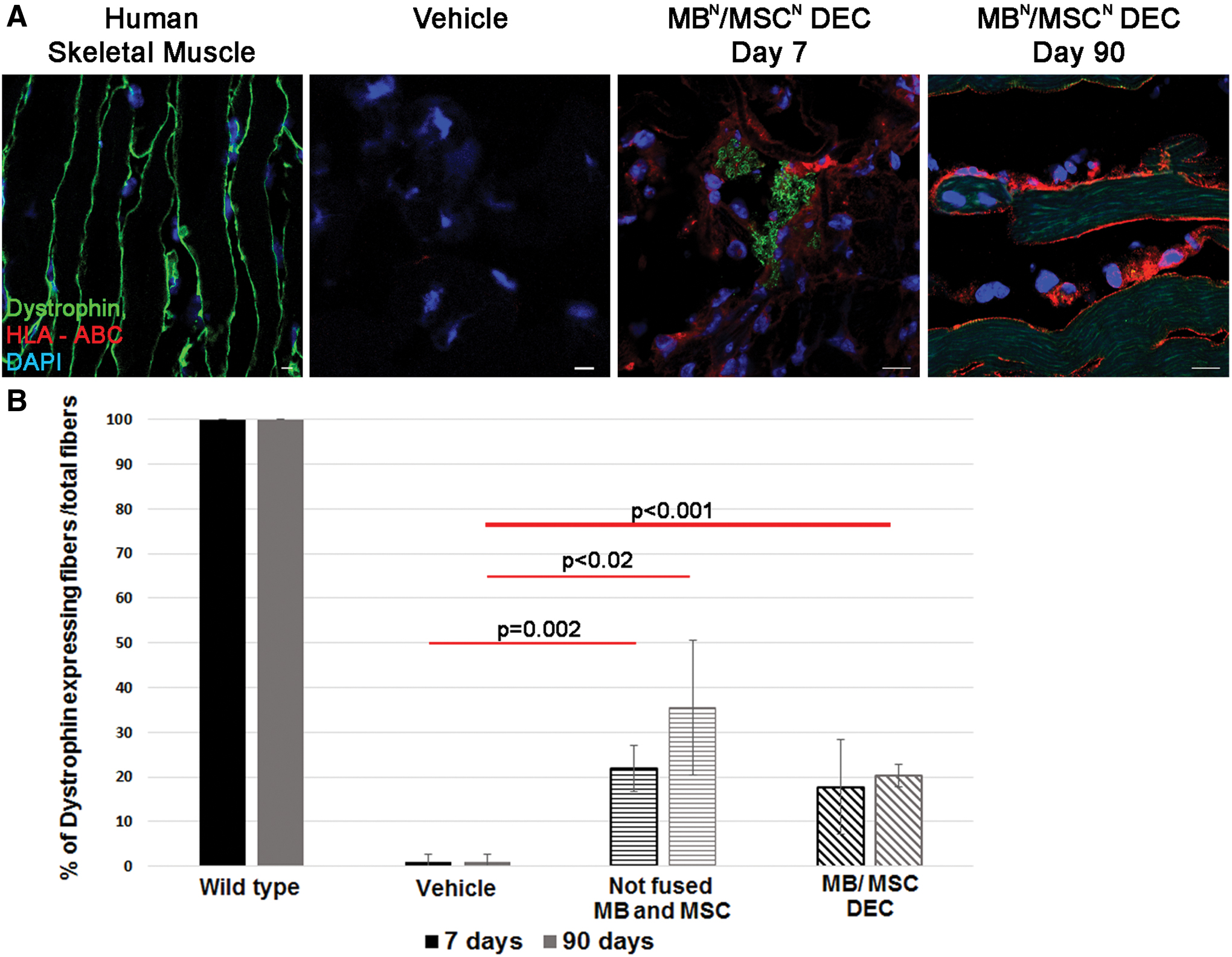
Human MBN/MSCN DEC engraft, differentiate into skeletal muscles, and maintain dystrophin expression up to 90 days after intramuscular injection to the GM of the mdx/scid mouse.
Quantification of dystrophin expressing fibers at 7 and 90 days post-DEC transplant confirmed increase in MBN/MSCN-injected muscles compared with vehicle-injected controls (17.7% ± 10.5% vs. 0.95% ± 1.65% at 7 days and 20.3% ± 3.25% vs. 0.98% ± 1.69% at 90 days, respectively (P < 0.05). Muscles transplanted with nonfused myoblasts and MSC revealed increased dystrophin expression at level of 21.89% ± 5.2% at day 7, and 35.6% ± 15.04% at day 90 (P < 0.05) (Fig. 5B).
Histological and immunofluorescence analysis
Structural analysis of H&E stained cross sections of GM injected with nonfused MBN and MSCN (Fig. 6A) and DEC (Fig. 6B), revealed decreased number of CNF compared with vehicle-injected controls (Fig. 6C) indicating reduced muscle pathology. Masson's Trichrome staining of GM samples indicated lack of muscle damage or scar tissue formation after MBN/MSCN DEC injection (Fig. 6D, E) to GM of mdx/scid mice.
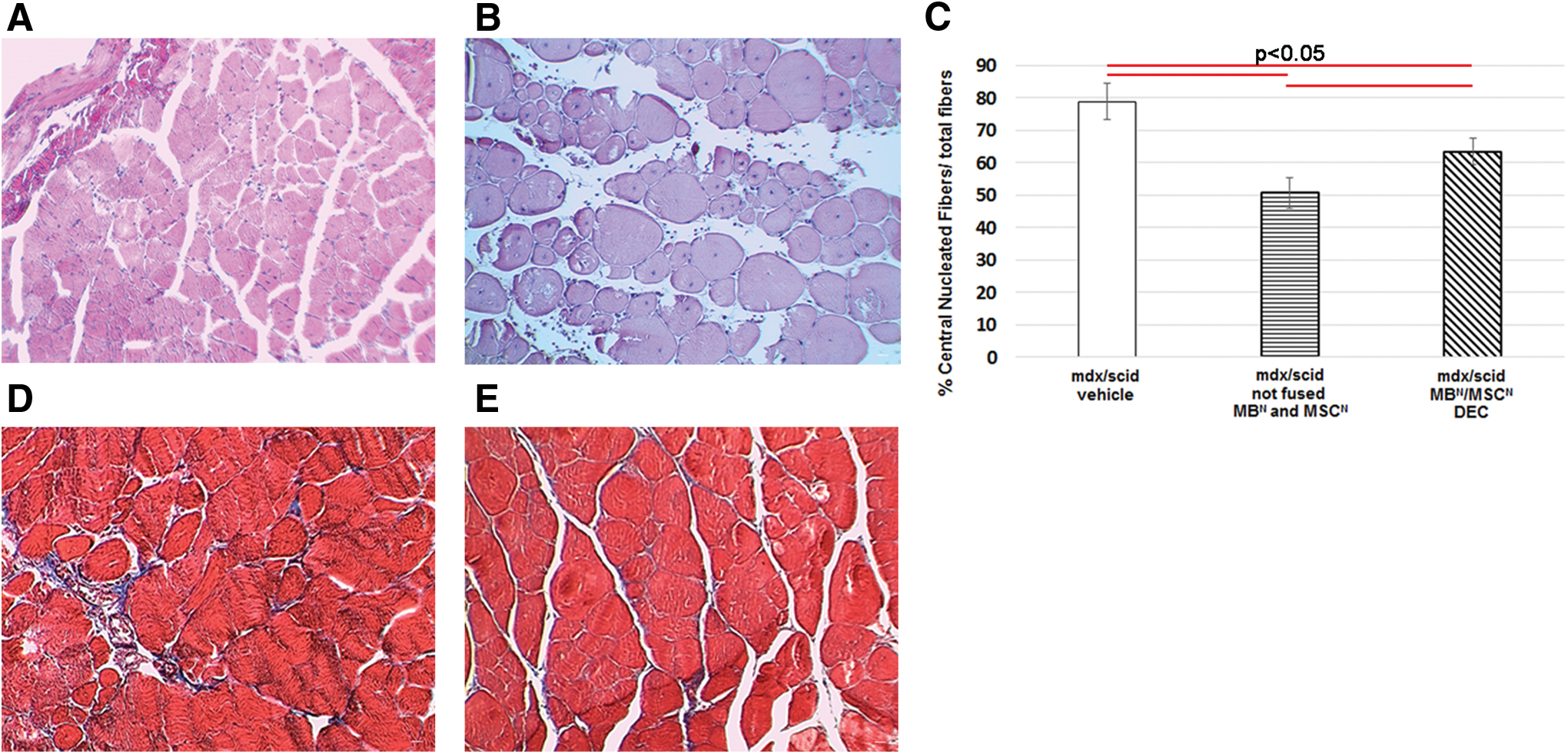
Muscle structure analysis of GM at day 90 after intramuscular MBN/MSCN DEC transplant to the mdx/scid mice.
Assessment of functional outcomes 90 days after MBN/MSCN DEC transplant
In vivo and ex vivo muscle force assessments tested efficacy of DEC on GM function at 90 days post-transplant (Fig. 7A–D). MBN/MSCN DEC-injected mdx/scid mice significantly improved in vivo muscle force (Fig. 7A) compared with vehicle-injected controls and nonfused MBN and MSCN cells. Improved muscle force was consistent with results of grip strength and wire hanging tests, which revealed an improvement in muscle force between day 14 and 42 in DEC-injected mice (Fig. 7E, F); however, due to the behavioral/cognitive learning bias influencing test outcomes, we present these results as supportive data.
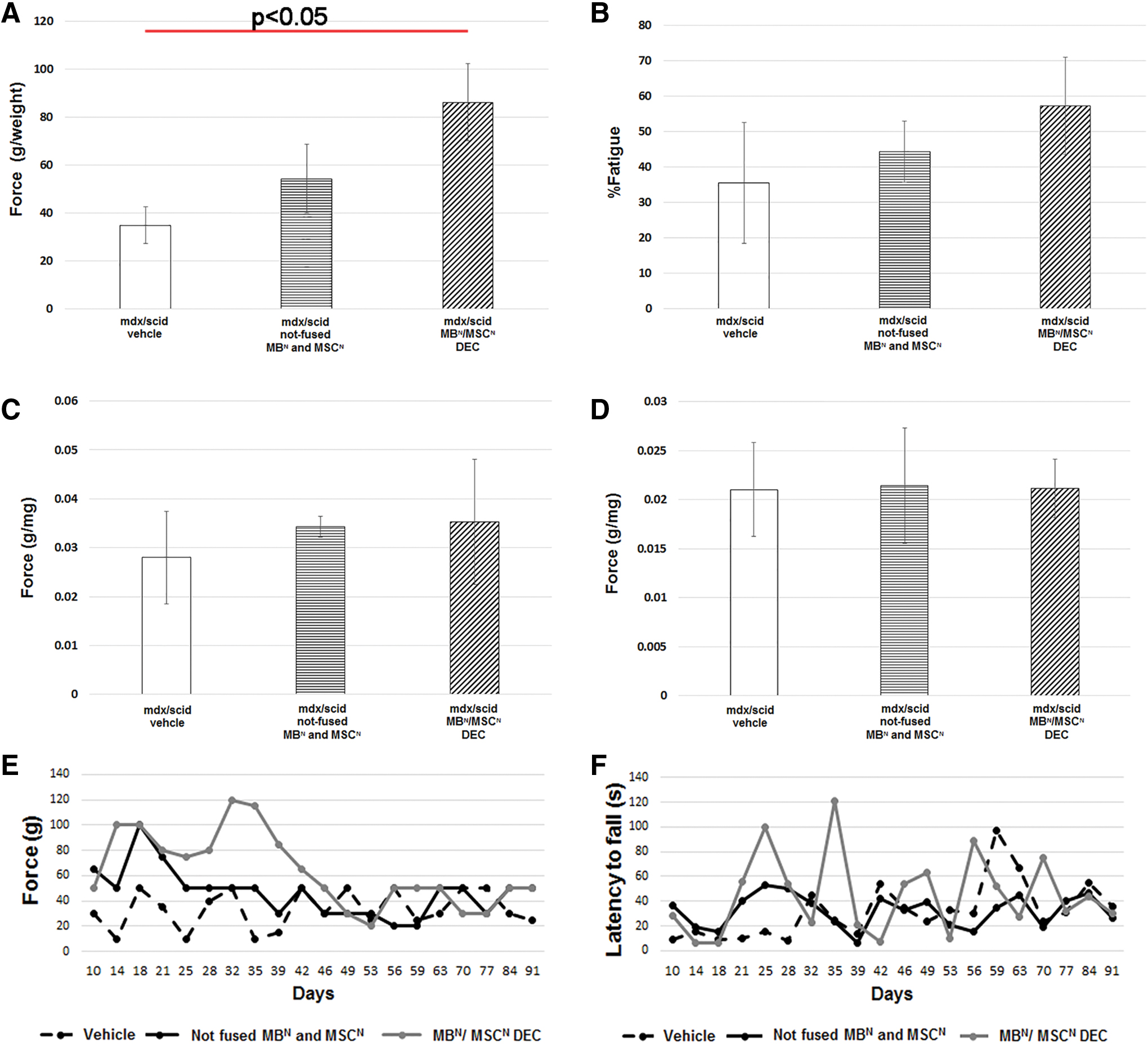
MBN/MSCN DEC improves muscle force, grip strength, and wire hanging time 90 days after intramuscular injection to dystrophic muscles of mdx/scid mice.
Discussion
DMD is a progressive lethal X-linked recessive disease [1], characterized by lack of functional dystrophin that leads to loss of motor, cardiac and respiratory function, and premature death [2,3]. Despite significant scientific and clinical efforts to introduce new therapies [3,9 –11], currently there is no cure for DMD patients.
The emerging myoblast and satellite stem cell-based and gene therapies show promising results in clinical trials [34,35]. Although promising, satellite cells showed to be difficult to isolate and obtain number of cells sufficient for therapeutic application [36] and satellite cells culturing impaired in vivo engraftment potential after transplantation [37].
Experiments testing type 2 pericytes and their progeny mesoangioblasts for treatment of muscular dystrophies showed cells delivered through intra-arterial injection improved skeletal muscle function [38]; however, achieving successful results is significantly limited by delivery timing of the therapy [39].
Thus, limited engraftment, low cell survival, and the need for immunosuppression to prevent cell rejection precluded their routine applications.
MSC represent good candidates for MD treatment as they proliferate rapidly, undergo myogenic conversion, and exhibit immunomodulatory properties; however, limited survival and myogenic differentiation within defected muscles remains unsolved [34]. Thus, there is an urgent need to develop new more effective strategies for DMD patients.
In the search of new approaches for DMD, we developed a novel DEC cell lines through ex vivo fusion of normal and dystrophin-deficient myoblasts [14,17]. These DEC lines were successfully tested in the preclinical models of mdx and mdx/scid mice [14,17]. We confirmed increase in dystrophin expression that correlated with significant improvement of muscle strength and function at 90 days after DEC transplant [17].
Based on these encouraging results, we explored new parent cell candidates for DEC creation. Since MSCs were previously tested in experimental models and clinical trials in DMD patients, we have chosen bone marrow-derived MSC as a new parent cell candidate for creation of human DEC line of myoblast and MSC origin (MBN/MSCN).
Successful generation of new human MBN/MSCN DEC line was confirmed by confocal microscopy, flow cytometry and PCR indicating that concept of cell fusion from two different cell lineages is feasible, reproducible, and safe as confirmed by lack of DNA damage by COMET assay. At 90 days post-transplant DEC preserved MBN/MSCN phenotype and maintenance of dystrophin expression that correlated with significantly improved muscle strength and function and reduced allogenic immune response confirmed by MLR.
These findings correlated with assessments of DEC lines of myoblast origin tested in the mdx and mdx/scid mouse models of DMD [14,17]. Interestingly, increased dystrophin expression after nonfused cell injection did not correlate with improvement of muscle function observed after transplant of fused MBN/MSCN DEC cells. We have recently observed similar outcome, where protective cardiac effect was confirmed after systemic-intraosseous transplant of fused MBN/MSCN DEC cells but not after injection of nonfused cells [30].
In contrast to the previously reported DEC studies [14,17,30], the novelty of this study is the generation of a new MBN/MSCN DEC cell line that was created for the first time from human cells of two different linages; the myoblast carrying dystrophin delivery potential and MSC carrying immunomodulatory properties.
Myoblasts fusion is a key cellular process responsible for muscle formation and repair. Thus, cell fusion has long been suggested as a potential therapeutic approach for the targeted cell fusion and complementation of genetic deficiencies in vivo. This therapeutic approach has been tested extensively in the context of DMD, indicating that exogenously delivered cells arising either from muscle or hematopoietic lineage could contribute to myofiber formation through cell fusion and support regeneration of the damaged muscle [40]. We have adapted myoblast fusion as a therapeutic approach in our previous DEC studies [14,17,30] as well as in this study by transplant of MBN/MSCN DEC cells to the dystrophic muscles of mdx/scid mice model of DMD for restoration of dystrophin expression and regeneration of the dystrophic muscles.
In the clinical scenario, myoblast (MBN) component of DEC will be from muscle biopsy of normal allogeneic donor, whereas MSCDMD component from bone marrow biopsy of the DMD-affected donor representing the autologous component of DEC to reduce immune response and need for immunosuppression.
There are several limitations of this proof-of-concept study, which was focused on confirming feasibility of creating new DEC cell line of two different cell linages MB and MSC and confirming functional efficacy of the created DEC cells. However, we have not evaluated interactions of DEC cells with myogenic and nonmyogenic cell populations. We have addresses safety of the fusion procedure by COMET assay, but have not performed karyotype assessment in this study. However, in the currently ongoing DEC study, we tested the karyotype of both the parent cells before fusion as well as the DEC cells after fusion and confirmed presence of normal karyotype without aneuploidy or chromosomal aberrations. We are planning to address these issues in the future studies.
For future clinical applications MBN/MSCN DEC can be propagated, cryopreserved, and stored for re-dosing without the need for additional biopsy, which represents advantages over nonfused cell therapies. When compared with current gene or viral vector-based therapies, MBN/MSCN DEC does not require viral vectors, genome editing, or cell reprogramming, therefore may be considered as a potentially safer therapy for clinical applications in DMD.
Conclusions
This study introduces novel concept of ex vivo creation of new human DEC cell line of MB and MSC origin as a potential therapy for DMD patients, alone, or in combination with other therapies where access to myoblasts and/or MSC is limited and re-dosing is challenged by occurrence of sensitization.
Footnotes
Acknowledgments
The authors thank Enza Marchase, MS, and Katarzyna Futoma, PhD, for technical assistance in this study, staff members of Core Imaging Facilities at University of Illinois, for acquiring confocal microscope images, and staff of Flow Cytometry Core, for technical assistance with DEC sorting.
Author Disclosure Statement
K.S. is CEO and shareholder of Dystrogen Therapeutics SA, the company holds a license for DEC therapy. M.S. is CMO and shareholder of Dystrogen Therapeutics SA, the company holds a license for DEC therapy. A.H. is the adviser to the Dystrogen Therapeutics. The authors declare a potential conflict of interest. M.S. is the inventor on the patent application filed by University of Illinois at Chicago related to chimeric cell therapy for Duchenne muscular dystrophy (WO/2016/201182). The authors J.C., A.H., J.G.-M., A.D.-S., and E.S. have no financial conflict of interest. University of Illinois at Chicago has approved the Nepotism Disclosure and Management Plan for M.S. and K.S. The authors M.S., J.C., A.H., J.G.-M., E.S., A.D.-S., and K.S. do not have any nonfinancial interest.
Funding Information
This study was supported by University of Illinois Chancellor's Innovation Fund Proof of Concept Award. A.D.-S. research fellowship was supported by The Kosciuszko Foundation.