
Abstract
Heterotopic ossification (HO) is a devastating condition in which ectopic bone forms inappropriately in soft tissues following traumatic injuries and orthopedic surgeries as a result of aberrant mesenchymal progenitor cell (MPC) differentiation. HO leads to chronic pain, decreased range of motion, and an overall decrease in quality of life. While several treatments have shown promise in animal models, all must be given during early stages of formation. Methods for early determination of whether and where endochondral ossification/soft tissue mineralization (HO anlagen) develop are lacking. At-risk patients are not identified sufficiently early in the process of MPC differentiation and soft tissue endochondral ossification for potential treatments to be effective. Hence, a critical need exists to develop technologies capable of detecting HO anlagen soon after trauma, when treatments are most effective. In this study, we investigate high frequency spectral ultrasound imaging (SUSI) as a noninvasive strategy to identify HO anlagen at early time points after injury. We show that by determining quantitative parameters based on tissue organization and structure, SUSI identifies HO anlagen as early as 1-week postinjury in a mouse model of burn/tenotomy and 3 days postinjury in a rat model of blast/amputation. We analyze single cell RNA sequencing profiles of the MPCs responsible for HO formation and show that the early tissue changes detected by SUSI match chondrogenic and osteogenic gene expression in this population. SUSI identifies sites of soft tissue endochondral ossification at early stages of HO formation so that effective intervention can be targeted when and where it is needed following trauma-induced injury. Furthermore, we characterize the chondrogenic to osteogenic transition that occurs in the MPCs during HO formation and correlate gene expression to SUSI detection of the HO anlagen.
Introduction
Heterotopic ossification (HO) is a devastating condition in which ectopic bone forms inappropriately in the soft tissue following large surface area burns, musculoskeletal trauma, and orthopedic surgeries due to aberrant mesenchymal progenitor cell (MPC) differentiation [1,2]. Formation of HO leads to chronic pain, decreased range of motion, and an overall decrease in the quality of life [3]. The military population has been shown to be particularly at risk of HO following battlefield wounds, with occurrences in over 60% of soldiers with extremity trauma [4]. Diagnosis of HO currently relies on computed tomography (CT), magnetic resonance imaging (MRI), or x-ray imaging modalities [1]. However, these modalities are expensive, nonportable, and not always available. Most importantly, current imaging modalities are unable to identify areas in wounds and injured tissue of early ectopic soft tissue mineralization, which is indicative of the HO anlagen, sufficiently soon after traumatic injury. As a result, HO is typically visualized only after mature bone has formed, as diagnosis relies on the use of CT, MRI, and/or x-ray to identify mineralized ectopic lesions [5,6]. While technologies such as [18F]NaF PET/CT scans and Raman spectroscopy are promising technologies to identify endochondral bone formation, these technologies are yet to be effectively developed for large-scale clinical use [7 –9]. Once mature bone has formed, surgical excision of the bony lesions becomes the only treatment option. However, surgical excisions are often very technically complex, and even after excision, ectopic bone recurs in a majority of operations, leading to poor final outcomes [10 –12].
Several studies for HO mitigation in animal models have reported multiple pathways as promising targets for therapy when used during the very early stages of endochondral bone development, including modulation of bone morphogenetic protein (BMP) signaling and mechanistic target of rapamycin signaling, local antibiotic delivery, and inhibition of Hif1α [13 –17]. Hif1α inhibitors, in particular, have been shown to be highly effective when delivered immediately following traumatic injury in animal models [14]. Importantly, all potential treatments must be given during the cellular phase in which MPC migration, proliferation, and differentiation are occurring. Once these cells have transitioned from immature-mature ectopic bone, these treatments fail at inhibiting progression of HO [14,15]. Why some patients develop HO and others do not and why some parts of a patient's wound develops HO while other parts do not remain unknown and cannot be accurately predicted. Therefore, there is a critical need for effective methods for early determination of whether and where HO is developing so that effective intervention can be targeted when and where it is needed.
Ultrasound imaging is an appealing modality for assessing early changes in soft tissues, such as phases of endochondral ossification leading to mineralized HO, because it is portable, painless, cost-effective, and safe, making it an ideal candidate to frequently image post-traumatic tissue noninvasively. In this study, we expand upon a novel high frequency spectral ultrasound imaging (SUSI) technique [18] to detect sites of endochondral ossification at early time points in two animal models of traumatic HO. As opposed to traditional ultrasound imaging approaches that typically rely on grayscale images that are system and operator dependent, SUSI utilizes additional backscattered radiofrequency (RF) data to extract quantitative parameters associated with tissue intrinsic properties for high-resolution tissue characterization [18,19]. We show that SUSI allows for improved ability to quantitatively discriminate between tissue types present in two models of hind limb extremity trauma and demonstrates the chondrogenic to osteogenic progression of the HO anlagen. This chondrogenic to osteogenic transition in the MPC population is further characterized by single cell RNA analysis and correlated to SUSI parameters.
Materials and Methods
Animals
Male C57BL/6J mice were obtained from The Jackson Laboratory (Bar Harbor, ME; stock no. 000664). All mice were 6–8 weeks of age at time of injury. Adult male (11–12 week old, 350–450 g) pathogen free Sprague Dawley rats were obtained from Taconic Biosciences (Germantown, NY). Animals were housed for a minimum of 7 days for acclimatization and quarantine purposes before experimental procedures. Animals were housed and maintained under standard conditions: 72°F ± 4°F, with a 12-h light/12-h dark cycle and no diet restrictions. All experiments and animal care procedures were approved by the University of Michigan (mouse protocol PRO 7930) and the Uniformed Services University of the Health Sciences (protocol SUR-18-065) Institutional Animal Care and Use Committees. All activities were conducted in accordance with applicable regulations.
Burn/tenotomy HO procedure in the mouse model
A traumatic burn/tenotomy (B/T) injury that leads to HO formation was performed as previously described [8,20]. Briefly, mice were anesthetized with inhaled isoflurane. Dorsal hair was shaved, and a partial-thickness scald burn injury that comprised approximately 30% of the total body surface area was administered on the dorsal surface using an aluminum block heated to 60°C for 18 s. Mice also received a tenotomy of the Achilles tendon and closure of the skin over the tenotomy site with one 5-0 vicryl suture. Buprenorphine (Buprenex, Reckitt Benckiser Pharmaceuticals) at 0.06 mg/kg given subcutaneously was administered preoperatively and every 12 h for 2 days. For SUSI, six mice were assessed in a longitudinal study for 9 weeks. For scRNAseq, three mice underwent B/T and one mouse was an injured control. The site of HO formation was collected for sequencing.
Blast/amputation injury and tissue collection in the rat model
HO was induced in an established rat model of blast-related traumatic injury that incorporated the critical injury patterns associated with combat-related extremity injury. Briefly, Sprague Dawley rats were exposed to systemic blast overpressure (120 ± 7 kPa) using a pneumatically driven shock tube, followed by femur fracture and quadriceps crush injury as described previously [21]. This was followed by tourniquet application at the site of crush injury for 3 h before transfemoral amputation through the zone of injury. Animals were single housed postsurgery. Rats were administered prophylactic analgesia (Buprenex, 0.05 and 1.2 mg/kg buprenorphine SR) through subcutaneous injection before injury and repeated at 48–72 h, with further doses given as indicated based on pain assessment. Hind limbs exposed to blast/amputation (HO-limb) and contralateral blast injury only (blast injury only-limb) were collected and fixed in formalin at 3, 6, 9, 12, and 56 days postinjury (DPI). All samples were fixed for the same period of time. A total of n ≥ 6 rats per time point were assessed for the HO-limb and n ≥ 4 were assessed for the blast injury only-limb.
SUSI and analysis
A detailed description of imaging methods and analysis is provided in the Supplementary Data. Briefly, SUSI was performed with a VisualSonics VEVO770 high resolution small animal ultrasound imaging system, using a 55 and 30 MHz center frequency single element transducer for mice and rats, respectively, and analysis of the collected RF data was as previously described [18]. Ultrasound operators were not blinded to injury/control condition. Grayscale images were also obtained and used to aid the identification of normal anatomical features and suspected regions of early stage HO lesions (“HO anlagen”). To maintain consistency when selecting and evaluating HO anlagen in this study, a single trained operator who is familiar with HO formation patterns and visualization in both rodent models identified anatomical reference landmarks. This operator was not blinded to condition. In the longitudinal mouse study, HO anlagen were identified at 1-week postinjury, and the same lesion was identified and quantified each week. Analysis of SUSI parameters calculated the average acoustic concentration (AAC) and average scatter diameter (ASD) of the HO anlagen, surrounding soft tissue in the zone of injury, and calcaneus in the mouse model. In the rat model, the AAC and ASD of the HO anlagen, surrounding soft tissue in the zone of injury of the HO-limb, injured soft tissue in the blast injury only-limb, and femur were determined. All analyses included at least four consecutive image frames. AAC and ASD values were grouped by time point and tissue type for statistical comparison.
Microcomputed tomography
Injured limbs from mice subjected to the B/T model were harvested at 9 weeks postinjury and scanned by microcomputed tomography (MicroCT). Bone volumes were determined (Bruker SkyScan 1176, 35 μM resolution, 357 μA beam). Bone reconstructions were performed by blinded operators manually splining around ectopic tissue and computing volumes at 800 Hounsfield Unit threshold (GE Healthcare v2.2, Parallax Innovations rc18). Ectopic bone volumes were characterized as total volume, including calcaneus associated and soft tissue associated. MicroCT imaging of rat limbs was carried out in the Inveon small animal scanner (Siemens). Images were acquired at 435 milliseconds exposure at Bin2. Volumetric analysis of total ectopic and soft tissue-associated bone was performed by three blinded operators, and the final volume represents the average of three independent blinded readings. The Bone Morphometry Tool (Inveon Research Workplace) was used for volumetric quantification.
Single cell RNA sequencing and pathway analysis
Detailed methods for single cell RNA sequencing and bioinformatics analysis are included in the Supplementary Data and described previously [22]. Single cell data were taken from GSE150995 as follows: day 0 (uninjured) control injury site (one mouse), day 7 mobile injury site (one mouse), day 42_1 injury site, and day 42_2 injury site (two mice total at 42 DPI). No additional samples were added to this previously published data set. Immobile injury site and isolated nuclei samples from GSE150995 were not considered in this study.
Using lineage tracing Hoxa11CreER R26TdTomato reporter mice, Pagani, et al. found that a subset of the Hoxa11 lineage MPCs becomes HO in the burn/tenotomy model [22,23]. Therefore, progenitor cells of HO were identified by expression of tdTomato, platelet derived growth factor receptor alpha (Pdgfra), aggrecan (Acan), and fibrillin 2 (Fbn2). Detailed methods of tamoxifen induction and scRNA harvest in these mice are provided in the Supplementary Data. Gene overlap, pathways, and gene ontogeny at each time point were analyzed using Advaita Bio's iPathwayGuide [24 –28].
Statistical analysis
Statistical tests were performed using GraphPad Prism 7.0 (GraphPad Software, Inc., San Diego, CA) software. To assess significance, a one-way analysis of variance and Tukey's test were used to compare the average of each group to that of every other group. All data are presented as mean values with standard deviation, and P values <0.05 were considered to be statistically significant.
Results
SUSI distinguishes anatomical features in the uninjured and injured limb following burn-tenotomy
We used SUSI to identify and characterize native anatomical structures at the site of tenotomy (near the attachment of the Achilles tendon to the calcaneus) in burn/tenotomy (B/T) injured and contralateral uninjured limbs (Fig. 1A). Grayscale images were obtained and used to identify native anatomical features, including skin and the calcaneus (Fig. 1B), which were used as a reference for normal anatomy. In the injured limb, skin, calcaneus, injured soft tissue, and HO anlagen were also identified using grayscale images, as shown in Fig. 1C. Anatomical shape and location matched as expected in uninjured and injured images.
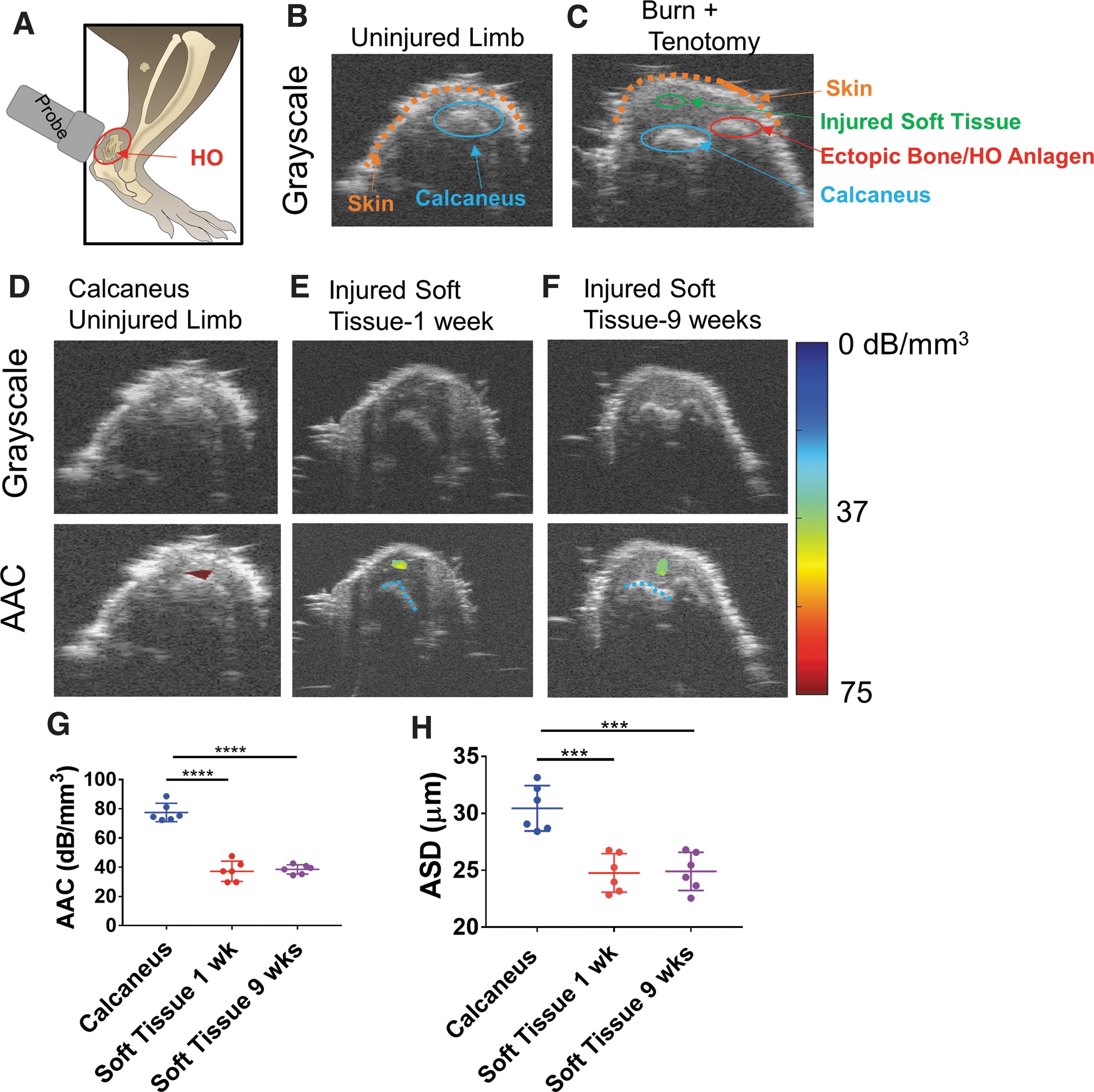
SUSI detects normal anatomical features and HO lesions in a mouse burn-tenotomy model.
To test that SUSI identified different tissue types, the calcaneus (uninjured limb) and soft tissue (1 and 9 weeks post B/T) within the zone of injury were selected for analysis, and AAC and ASD values were calculated. As shown in Fig. 1D–G, the AAC of the calcaneus was significantly higher compared with injured soft tissue at 1 and 9 weeks post B/T at the injury site (77.5 ± 6.3, 37.2 ± 6.9, 38.6 ± 3.2 dB/mm3 calcaneus, injured soft tissue at 1 week, 9 weeks, respectively; n = 6/group; P < 0.0001 for calcaneus vs. injured soft tissue at 1 week and calcaneus vs. injured soft tissue at 9 weeks; mean ± std. dev. here and throughout), indicating that mineralized tissues possess higher AAC values than soft tissue.
The ASD was also significantly higher in the calcaneus than injured soft tissue at 1 and 9 weeks post B/T (30.4 ± 2.0, 24.8 ± 1.7, 24.9 ± 1.7 μm calcaneus, injured soft tissue at 1 week, 9 weeks, respectively; n = 6/group; P < 0.0001 for calcaneus vs. injured soft tissue at 1 week and calcaneus vs. injured soft tissue at 9 weeks).
These results indicate that SUSI is capable of distinguishing native bone from surrounding soft tissue based on AAC and ASD values. Therefore, we hypothesize that the AAC and/or ASD parameters may be useful to identify sites of endochondral ossification and/or tissue mineralization that result in ectopic bone formation after traumatic injury.
SUSI detects HO formation at 1-week postinjury in mouse burn-tenotomy model
Treatment of HO is currently limited by the lack of a reliable screening method to identify sites of endochondral ossification and tissue mineralization following trauma. Therefore, we next sought to use SUSI to screen for early soft tissue endochondral ossification (HO anlagen formation) in models of hind limb extremity trauma. Our results show that as early as 1-week post B/T, HO anlagen were identified in the grayscale images of high frequency ultrasound imaging (Fig. 2A, red outline in grayscale image). While it is possible to use grayscale images to detect tissue differences, grayscale images are system and operator dependent and, thus, cannot provide an objective assessment. Therefore, we used SUSI quantification to provide objective, system independent assessment of tissue properties. A B/T was performed on six mice, and animals were followed longitudinally. As expected, at 1-week post B/T, the AAC of the HO anlagen was significantly lower compared with the calcaneus, which matches previous reports showing that the HO anlagen at 1 week postinjury is largely cartilaginous and not composed of mature bone [18]. At 1-week post B/T, the AAC of the HO anlagen was significantly different compared with surrounding injured soft tissue, indicating that quantitative measurement of AAC using SUSI distinguished the developing HO anlagen from the surrounding soft tissue in the injury zone and the calcaneus as early as 1 week post B/T, as shown in Fig. 2A, E (51.3 ± 6.1, 37.2 ± 6.9, 77.5 ± 6.3 dB/mm3 in HO anlagen, injured soft tissue, calcaneus, respectively; n = 6/group; P < 0.0001 for HO compared to calcaneus, P < 0.01 for HO compared to injured soft tissue). At 2 weeks post B/T, the AAC of the HO anlagen remained significantly different compared with surrounding soft tissue and calcaneus, as shown in Fig. 2B, E (52.7 ± 6.7, 34.3 ± 6.8, 77.5 ± 6.3 dB/mm3 in HO anlagen, soft tissue, calcaneus, respectively; n = 6/group; P < 0.001 both analyses). Similarly, the AAC of the HO anlagen was also significantly different than surrounding soft tissue (P < 0.0001) and calcaneus (P < 0.0001) at 3 weeks postinjury. By 6 weeks postinjury, the AAC of HO was similar to that of the calcaneus, indicating progressive mineralization of the HO anlagen to mature ectopic bone (70.4 ± 5.5 and 77.5 ± 6.3 dB/mm3 in HO and calcaneus, respectively, at 6 weeks postinjury, P > 0.05) and remained similar to that of the calcaneus at 9 weeks postinjury (P > 0.05) (Fig. 2C–E). MicroCT imaging confirmed ectopic bone formation at 9 weeks post B/T (Supplementary Fig. S1). Past studies in the B/T model have corroborated what we found with SUSI: MicroCT and x-ray imaging demonstrate that mineralized ectopic bone is present at the site of the tenotomy at 4–6 weeks post B/T, with a significant increase in mineralized ectopic bone volume by 9 weeks post B/T (Supplementary Fig. S1) [18,29].
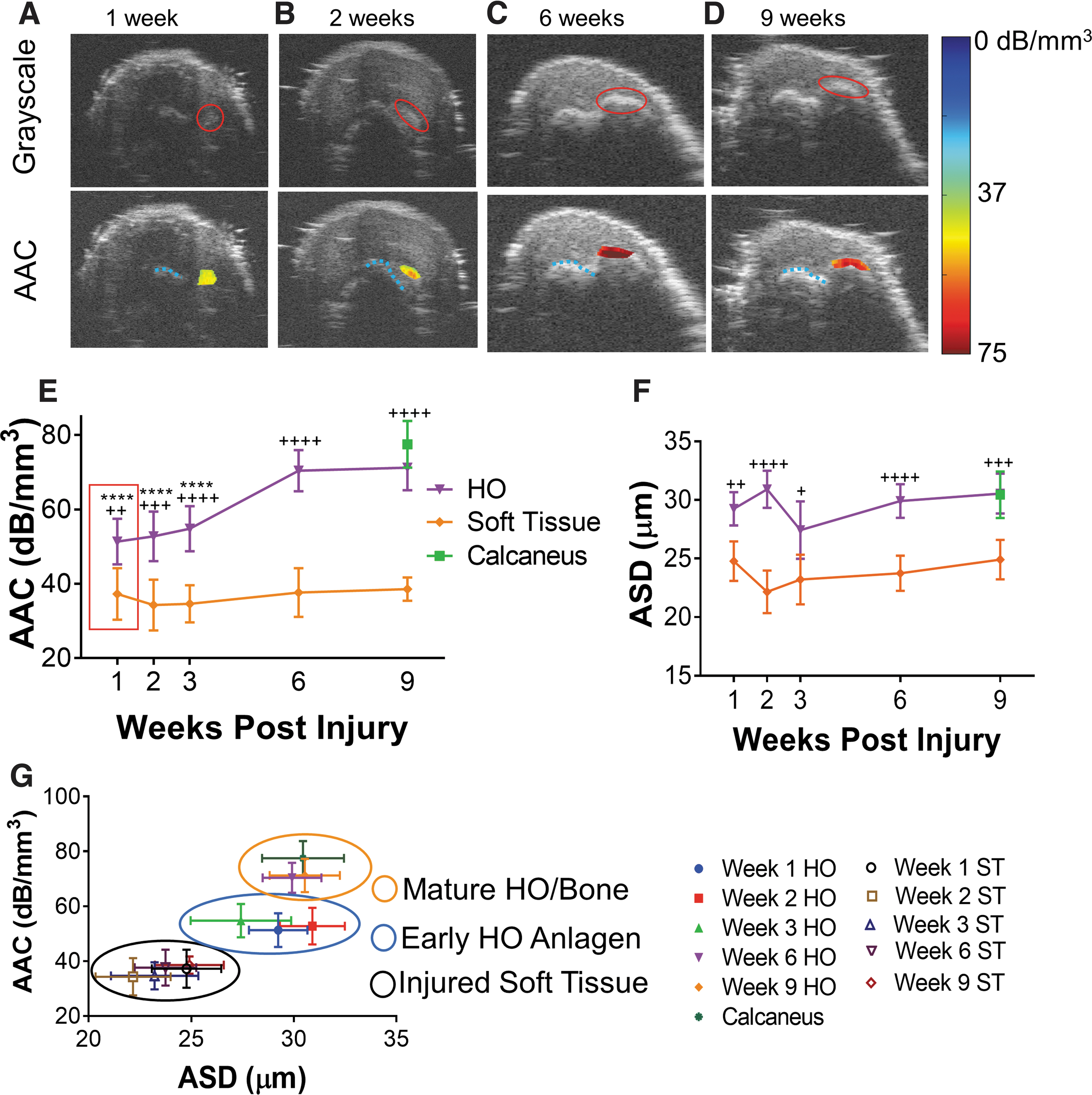
SUSI distinguishes HO anlagen at 2 weeks postinjury from surrounding injured soft tissue and native bone in the mouse B/T model. Grayscale images and AAC values overlaid on grayscale images at
Results of the ASD obtained from SUSI analysis on the HO lesion revealed significant differences from that of the soft tissue at weekly intervals, including week 1; however, the values of the ASD of the HO anlagen were similar to that of the calcaneus at each weekly analysis (Fig. 2F). Since the parameter of ASD depends on the size of ultrasound scatters, these results suggest that the characteristics of the constituents of the ectopic bone in the HO lesion, once formed, remain unchanged, while the density of such constituents, serving as the acoustic scatters, increased with time as shown by AAC (Fig. 2E). Therefore, the ASD parameter may be a useful diagnostic parameter early in HO development to distinguish HO anlagen from surrounding injured soft tissue as early as 1-week postinjury to corroborate the AAC. Combination of the ASD and AAC (Fig. 2G) demarcated clearly three groups. Soft tissue, early HO anlagen, and mature HO/bone are clustered together based on AAC and ASD values, indicating their utility for tissue characterization. In this study, we have shown that SUSI is able to distinguish sites of developing HO anlagen from surrounding injured soft tissue and native bone as early as 1-week postinjury based on the AAC and ASD values, which are unique parameters associated with intrinsic tissue property and microstructure.
Gene expression correlates with chondrogenic to osteogenic transition shown in AAC values
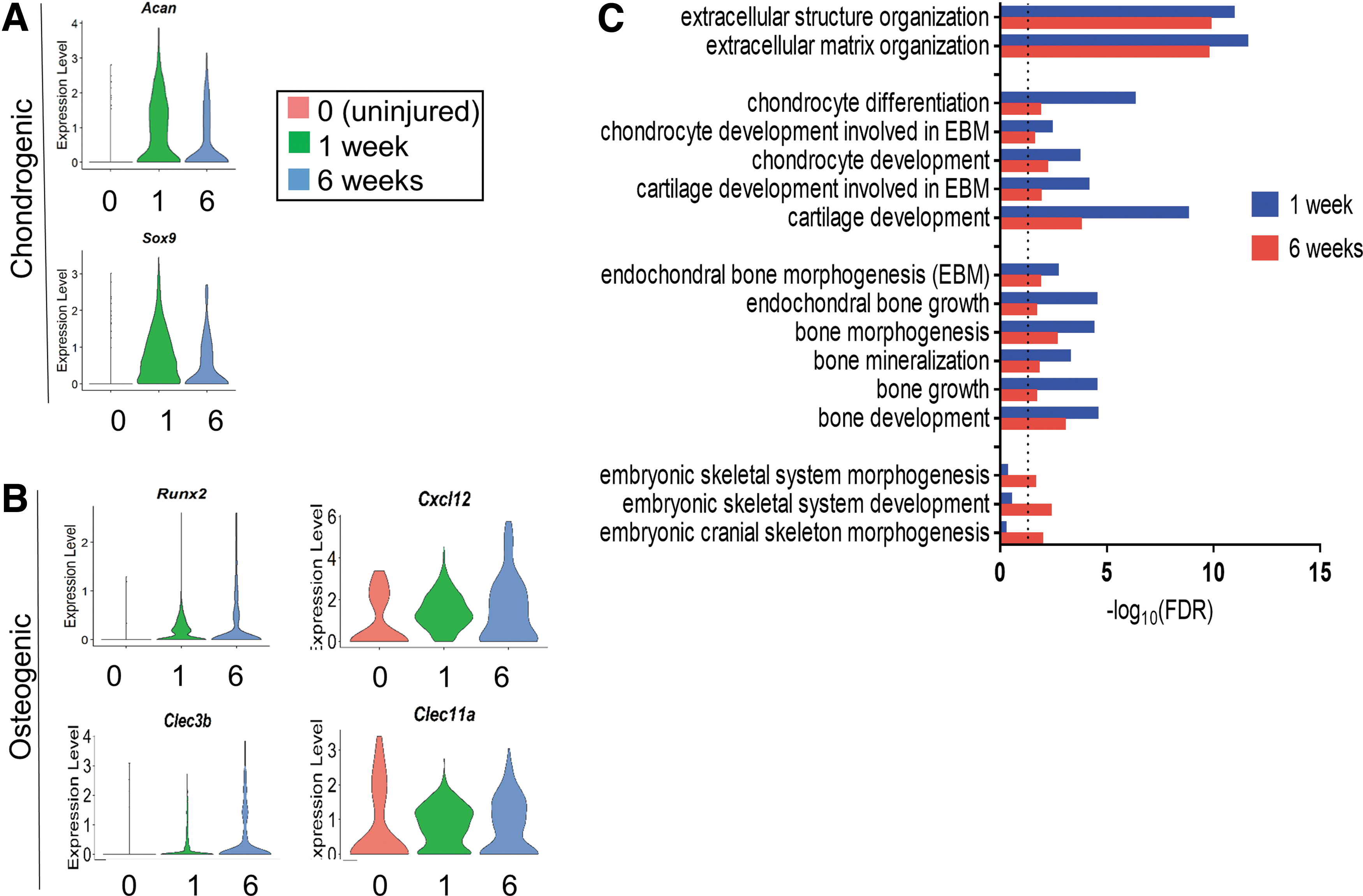
We have shown that the AAC values of the HO anlagen increase between 1 and 6 weeks postinjury, indicating an increase in mineralization of the HO anlagen through endochondral ossification (Fig. 2E). To further characterize this chondrogenic to osteogenic transition and compare with SUSI findings, we performed single cell RNA sequencing analysis of the region of HO formation in uninjured (“week 0”) and B/T injured tissue at 1 and 6 weeks post B/T. Clusters were determined by differential gene expression analyses to find highly and differentially expressed upregulated genes in each cluster. From these upregulated genes, marker genes were identified based on previous literature and used to identify populations (Supplementary Table S1) [22]. Immune, skin, muscle, vasculature, nerve, and MPC/fibroblast clusters were identified at every time point, as shown in Fig. 3. A robust immune response was seen at 1 week post B/T with expansion of the MPC/fibroblast populations. Further analysis of the MPC population shown to participate in the development of ectopic bone at 1 and 6 weeks postinjury was performed [22]. This population is characterized by expression of tdTomato (indicating Hoxa11 lineage), Pdgfra, Acan, and Fbn2 and is labeled MPC:0 in the UMAP plots (Fig. 3). A full description of this population has been described by Pagani, et al. and is included in Supplementary Table S1 [22]. We queried the MPC population for changes in expression of genes related to chondrogenesis and osteogenesis, which possess lower and higher mineralization levels, respectively. We find that at 1-week post B/T, chondrogenic genes such as Sox9 and Acan are upregulated compared to uninjured (week 0) and 6 weeks post B/T (Fig. 4A). By 6 weeks postinjury, osteogenic genes such as Runx2, Cxcl12, Clec3b, and Clec11a are also expressed, indicating a switch in the MPC population toward a more osteogenic genotype (Fig. 4B). Upregulated expression of osteogenic genes at 6 weeks post B/T corroborated with the increase in tissue mineralization detected with SUSI.
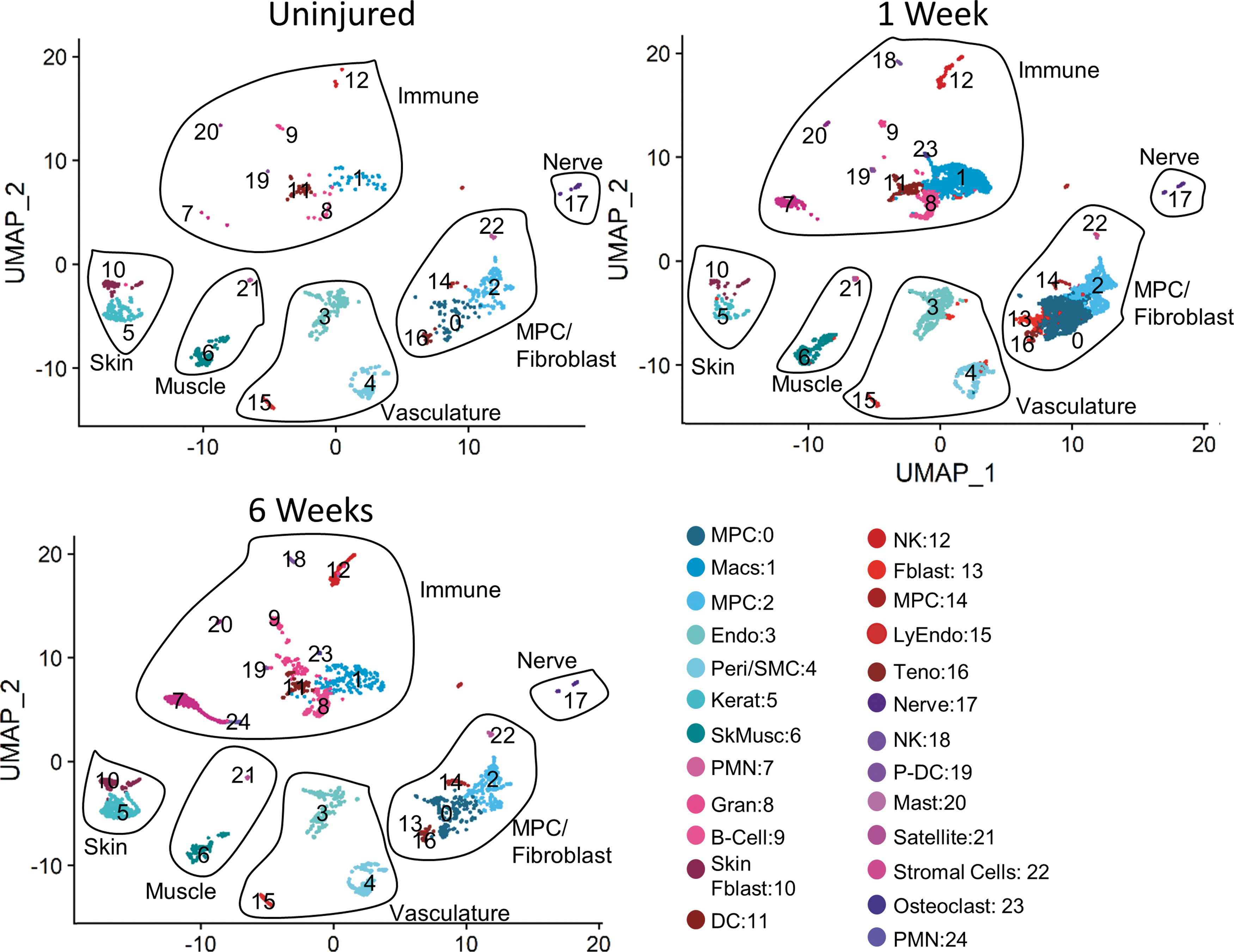
UMAP plots of cells in uninjured HO site, 1 and 6 weeks post B/T. BM, bone marrow; DC, dendritic cell; Endo, vascular endothelial cells; Fblast, fibroblast; Gran, granulocyte; Kerat, keratinocyte; LyEndo, lymphatic endothelial cell; Macs, macrophages; Mast, mast cell; MPC, mesenchymal progenitor cell; NK, natural killer T cell; P-DC, plasmacytoid dendritic cell; Peri/SMC, pericyte/vascular smooth muscle; PMN, polymorphonuclear leukocytes; Satellite, Satellite cell; SkMusc, skeletal muscle; Teno, tenocyte.
Chondrogenic to osteogenic transition in the MPC population.
Gene ontology analysis identifies chondrogenic to osteogenic transition
To more broadly characterize this chondrogenic to osteogenic transition, we probed gene ontology (GO) terms in the same MPC population at 1 and 6 weeks post B/T. Gene expression in the MPC population that goes on to form HO (MPC:0 in Fig. 3) was compared to all other clusters at the same time point to identify differentially expressed genes and GO terms in this MPC population. As expected, terms related to extracellular matrix (ECM) organization were highly enriched at both time points (Fig. 4C; GO ID, number of differentially expressed genes, and P values provided in Supplementary Table S1). GO terms involving chondrocyte differentiation, including chondrocyte development involved in endochondral bone morphogenesis (EBM), and cartilage development involved in EBM were more significantly enriched at 1 week post B/T than at 6 (Fig. 4C).
These findings are consistent with the SUSI data indicating that HO is in a chondrogenic state at 1 week post B/T, as indicated by a significantly lower AAC compared with mineralized bone. GO terms relating to bone development, including endochondral bone growth and bone mineralization, were significantly enriched at both time points after B/T, with more robust response at 1 week compared to 6 weeks post B/T (Fig. 4C). Enrichment of terms related to both chondrogenesis and osteogenesis at 6 weeks post B/T suggests than many MPC-derived cells at the site of injury repair and tissue regeneration are still in the cartilaginous phase of endochondral ossification, with a subpopulation having advanced to the osteogenic state. This further highlights the sensitivity of SUSI detection, as complete osteogenic transition in the MPC population does not appear to be necessary for HO lesion detection. Interestingly, pathways relating to skeletal development were enriched by 6 weeks postinjury and not by 1-week postinjury, further demonstrating the MPC transition toward an osteogenic state at a later time point (Fig. 4C). Taken together, gene expression and GO enrichment patterns correlated with the chondrogenic to osteogenic transition detected with SUSI at 1 and 6 weeks post B/T.
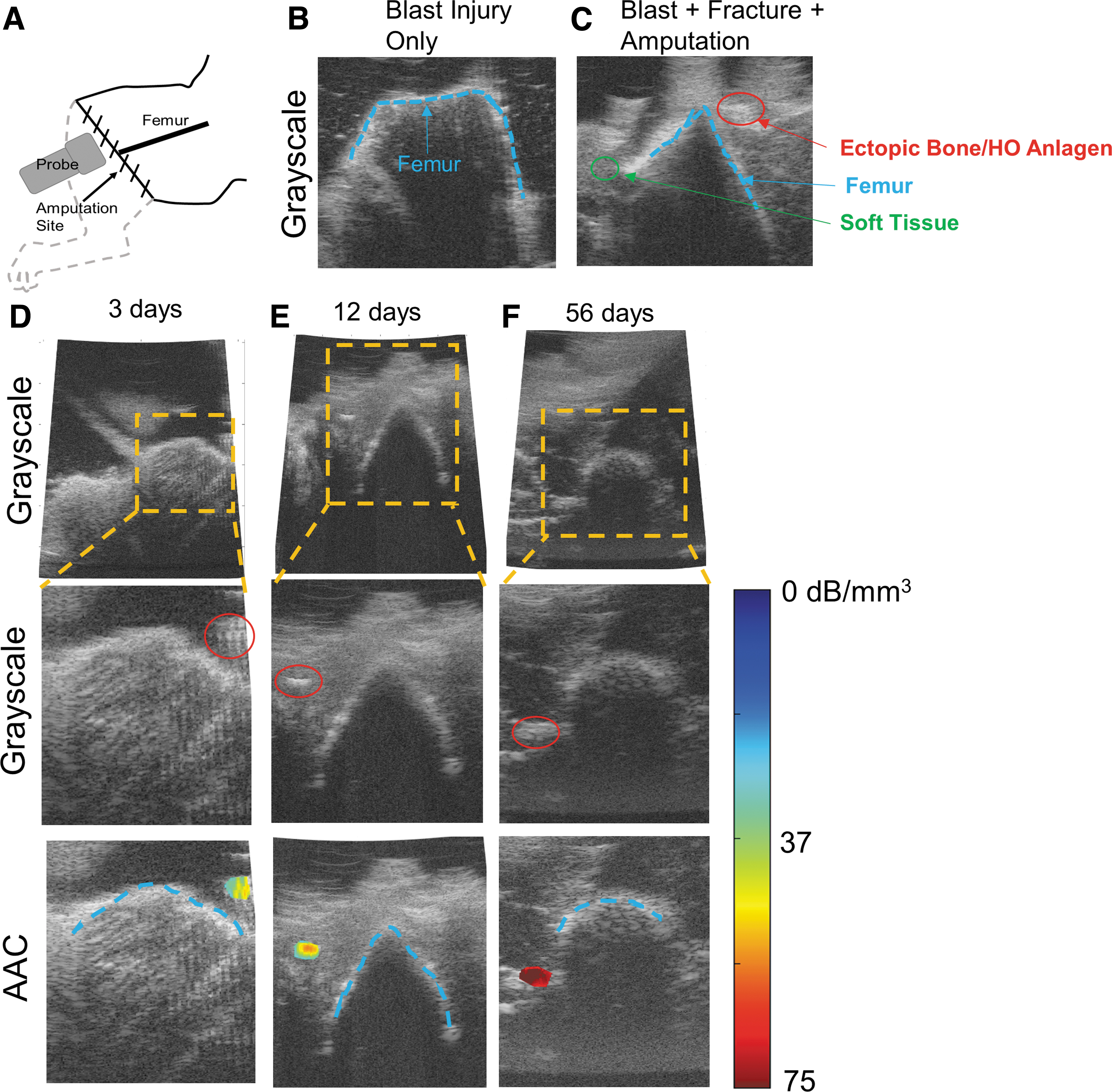
SUSI distinguishes native anatomical features and detects early HO formation in a combat HO model
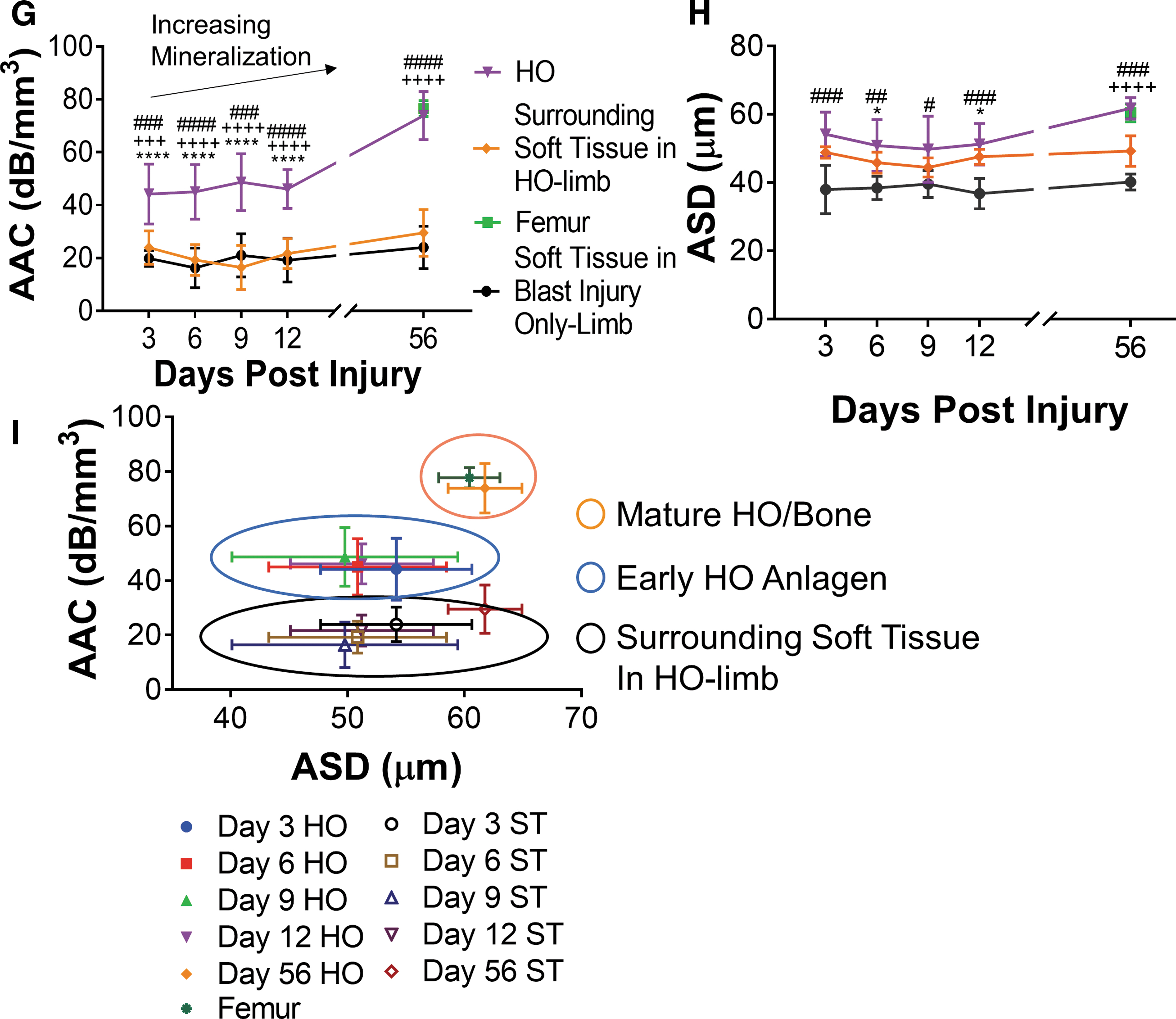
Since the B/T model is largely a tendon injury model without soft tissue insult at the HO site, we sought to investigate a model of HO formation that involved substantial soft tissue and muscular injury. The muscle niche releases multiple cytokines, chemokines, and other signal modulators after injury which modulate immune response and wound healing, all of which impact HO formation [22,30,31]. Soft tissue involvement is also present in most clinical presentations at high risk for HO, such as after traumatic injury, amputation, and hip replacement. Thus, we investigated the ability of SUSI to distinguish HO lesions from the surrounding injured soft tissue in a model of combat-related traumatic injury in a rat, which involves extensive soft and hard tissue damage. In this model, one limb was exposed to an HO-forming injury (whole body blast injury + fracture + muscle crush + amputation; referred to as “HO-limb”) and the other limb was exposed to a non-HO-forming injury (blast injury only; referred to as “blast injury only-limb”), thus serving as an injured control [30]. First, we used grayscale images to identify normal anatomy (femur) in the blast injury only-limb (Fig. 5A, B) and to identify the femur, surrounding soft tissue in the zone of injury, and HO lesions in the HO-limb at 3, 6, 9, 12, and 56 DPI (Fig. 5C–F) in separate animals for each time point (n ≥ 6/time point in HO-limb; n = 4–6 in blast injury only-limb). In this model, the AAC of the HO anlagen was significantly different compared with the surrounding soft tissue in the HO-limb, femur, and soft tissue in the blast injury only-limb by 3 DPI (44.2 ± 11.4, 24.0 ± 6.3, 76.5 ± 3.1, 19.9 ± 3.0 dB/mm3 in HO anlagen, surrounding soft tissue in HO-limb, femur, soft tissue in blast injury-only limb, respectively; P < 0.01 all analyses; n = 4–7). This distinction allows for nascent-stage diagnosis of the HO anlagen compared to soft tissue in the HO-forming injury near the HO lesion and injured soft tissue in the non-HO forming injury (Fig. 5D, G and Supplementary Fig. S2). The AAC of the HO anlagen was also significantly different compared with the surrounding soft tissue in the HO-limb and blast injury only-limb, as well as the femur at 6–12 DPI (P < 0.001; HO-limb: n = 8 at 6 DPI; n = 7 at 9 DPI; n = 6 at 12 DPI; blast injury only limb: n = 4–5), as shown in Fig. 5E, G and Supplementary Figure S2. By 56 DPI, the AAC of HO was similar to that of the femur (73.8 ± 9.1 and 76.5 ± 3.1 dB/mm3 in HO and femur, respectively, P > 0.05; n = 7), indicating a mature state of mineralization of the ectopic bone (Fig. 5F, G). Analysis of the ASD values of the HO anlagen was significantly different from that of the femur at 6 and12 DPI, as shown in Fig. 5H. Interestingly, ASD was able to consistently distinguish the HO anlagen from soft tissue in the blast injury only-limb, however not from surrounding soft tissue in the HO-limb (Fig. 5H). This may indicate that the ASD parameter detects the increased inflammation in the HO-limb compared to the blast injury only-limb, as indicated by the difference in ASD between soft tissue in each limb. By 56 DPI, ASD of the mature HO was similar to that of the femur and significantly higher compared with soft tissue in both the HO-limb and blast injury only-limb (Fig. 5H). Development of mature ectopic bone was confirmed at 56 DPI by MicroCT (Supplementary Fig. S1). In summary, three distinct clusters were present in the rat model, similar to the mouse B/T model: soft tissue, early HO anlagen, and mature HO/bone, allowing for improved characterization of tissue type (Fig. 5I). The AAC parameter consistently distinguished the HO anlagen from soft tissue in both limbs, while the ASD parameter distinguished HO anlagen from surrounding soft tissue in the HO-limb at 6 and 12 DPI and from surrounding soft tissue in the blast injury only-limb at 3–12 DPI. We have also shown that SUSI distinguishes between HO anlagen in the HO-limb and normal injury-related inflammation in the blast injury only-limb, further highlighting the ability of SUSI to distinguish early HO lesions from soft tissue inflammation. In the traumatic model of HO with soft tissue injury involvement, HO was detected as early as 3 DPI, allowing for early-stage diagnosis and initiation of treatment.
SUSI distinguishes HO anlagen at 3 DPI in rat model of blast + amputation injury.
Discussion
HO is classically detected radiographically after mature bone has formed, at which point treatment is no longer effective to arrest bone formation. Therefore, a clinical need exists for an imaging technology capable of detecting sites of early stage endochondral ossification within the injured soft tissue, which represent the HO anlagen. Prompt identification of HO anlagen would allow for early, targeted therapeutic interventions aimed at preventing bone formation and improving patient outcomes following traumatic injury and eliminate unnecessary treatment for patients that do not develop HO. In this study, we show that high frequency SUSI technique distinguishes HO anlagen from surrounding soft tissue near the HO lesion and from inflammation in a non-HO forming injury based on tissue mineralization at 1 week and 3 DPI in a mouse burn/tenotomy model and a rat blast/amputation model, respectively. In addition, tissue mineralization detected with SUSI correlates with gene expression in the HO anlagen and was also confirmed at study end points with MicroCT.
Current clinical HO diagnosis typically relies on radiography (X-ray) or CT scans, both of which require the presence of mineralized bone for accurate detection. Therefore, these methods are only useful for detecting mature HO and usually cannot detect HO until 6 weeks post-trauma, at which points potential treatments would not be effective [32 –34]. MRI has also been investigated for HO detection; however, it is also only able to reliably diagnose mineralized HO, as earlier imaging results in heterogeneous signal [34]. Three-phase bone scintigraphy (or single-photon emission computed tomography) is generally considered the most sensitive modality for HO detection, but earliest detection is still typically 2.5 weeks postinjury and local inflammation may cause false positives and high variability [32,33,35]. Raman spectroscopy and near-infrared optical imaging have shown promise in animal studies but remain to be translated to the clinic [9,36].
Ultrasound is portable, noninvasive, and nonionic, making it an ideal candidate to frequently screen injured healing tissue. Clinical grayscale, B-mode ultrasound imaging has been investigated for HO detection previously. However, B-mode ultrasound was only able to detect HO formation after mature bone had formed and symptoms were present, limiting its use to monitoring rehabilitation rather than early stage diagnosis and preventative treatment [27,37]. Importantly, grayscale B-mode ultrasound imaging is system and operator dependent, making it difficult to obtain subjective parameter based tissue intrinsic property for tissue characterization.
In contrast, SUSI utilizes the backscatter ultrasound signals and extracts parameters that are related to tissue microstructure and acoustic properties. It has previously been investigated for early HO anlagen detection, and here we expand upon the technique in several important ways [18]. First, we show that SUSI distinguishes HO anlagen from surrounding injured soft tissue in the region of HO formation, as well as from injured soft tissue in a limb with a non-HO forming injury, which is more clinically relevant than comparing to uninjured tissue, as HO anlagen typically form within the traumatic wound. We have also characterized SUSI in a clinically relevant model of blast/amputation injury in the rat, which mimics the injury patterns sustained by soldiers injured in combat. This larger rodent model also requires imaging of deeper tissues, more similar to human wounds.
An important feature of this SUSI technique is its objectivity. Unlike qualitative grayscale imaging, SUSI calculates quantitative parameters unique to the tissue properties, such as the acoustic concentration and the scatter diameter, based on a calibrated spectrum of the ultrasound backscattered signal from the tissue volume to quantify inherent properties of the tissue. These parameters can be used to identify tissue types, avoiding the dependencies of relying solely on interpretation of grayscale images. This results in less user or system dependency, more reproducibility, and improved tissue identification. Our results showed that at early time points, HO anlagen can be distinguished from surrounding reference tissues based on quantitative SUSI parameters, such as AAC and ASD. Therefore, in the future, discriminant analyses may be performed based on these parameters and less on user identification of interpretation of grayscale images, which depend on system settings.
We show that SUSI identifies the HO anlagen earlier in the blast/amputation injury (3 DPI) than the B/T injury (1-week postinjury). Inflammation has been shown to play a central role in driving HO formation, and increased inflammation at the HO site in the blast/amputation injury compared to the tendon injury is hypothesized to drive quicker HO inception and progression in the blast/amputation model [38 –40]. Indeed, previous reports have shown quicker formation of mature HO lesions in the blast/amputation model than the B/T injury [21,41]. Detection of the HO anlagen at earlier time point following blast/amputation injury further reflects the sensitivity of SUSI identification.
In addition to MicroCT scans at the study end points, we also correlate SUSI findings to differentiation state of the HO progenitor cells. Using scRNAseq in the mouse B/T model, we probe the ectopic bone-forming MPC population. We identify that chondrogenic gene expression is upregulated at 1 week postinjury in this MPC population, and by 6 weeks postinjury chondrogenic gene expression decreases and more osteogenic genes are upregulated. This transition represents the formation of ectopic bone through endochondral ossification. We find that SUSI detects the same pattern in the HO anlagen: at 1 week postinjury, the AAC of the HO anlagen is significantly different compared with the calcaneus; however, by 6 weeks postinjury the HO anlagen and native bone possess similar AAC values. We also probe GO terms in the MPC population to more broadly characterize HO development and find pathways related to ECM organization, EBM, and skeletal system morphogenesis which are increased in the HO-forming MPCs. This analysis provides important information about mechanisms of HO formation in the mouse B/T model, as well as serves as a cellular level confirmation of ectopic bone formation through endochondral ossification shown by SUSI.
Further validation and development of the SUSI technology will be crucial for its translation to clinical applications. Extrapolation to human patients will require deeper imaging. To achieve this penetration depth, a probe with a lower center frequency may be required (∼10 MHz), with a trade-off of lower spatial resolution as frequency decreases. To this end, SUSI spectral analysis has been validated at lower (5 MHz) frequencies and shown translational capabilities [42]. Identification of the early lesions may also be more challenging in much larger tissues. This may be corrected using large curved arrays or by incorporating elastography to identify stiffer regions, in addition to AAC and ASD quantification. Combination of SUSI analysis with acoustic radiation force impulse or shear wave elastography imaging may also yield improved HO lesion identification.
We foresee this technology as a valuable screening tool for patients at-risk for HO. After a high-risk surgical operation or traumatic injury, SUSI imaging can be performed at the most common sites of HO formation (hip, elbow, injury site) as early as 1–3 DPI in place of prophylactic treatment for every at-risk patient. While no broadly effective HO-specific treatment is currently available, we are hopeful that promising candidates in rodents, such as BMP and Hif1α inhibitors, will show translational efficacy to the human population. As these treatments must be given at early stages of HO formation, which we hypothesize to be within 1 week of injury in the human, early detection with SUSI will allow for the initiation of effective treatment regimes. It is also known that soldiers are disproportionately diagnosed with HO as a result of battlefield wounds. However, evacuation to a well-equipped hospital from the battlefield often takes several days to a week. Because SUSI is portable and easy to operate and interpret, we foresee this technology being especially impactful for the military population, as initial screening could be done in a field hospital setting without highly specialized medical personnel. With this early screening, initiation of treatment for these soldiers could be possible within the short window of effectiveness. Eventually, we hope that a standardized protocol of early SUSI screening, HO diagnosis, and treatment initiation will allow for effective treatment for HO patients and spare unnecessary treatment for at-risk patients who do not develop HO.
Conclusion
In conclusion, we have demonstrated that SUSI technology is capable of early detection of the HO anlagen after traumatic injury in two clinically relevant rodent models. Using the AAC and ASD signature of the tissue, SUSI allows for an objective, nonbiased assessment of the injured tissue. This technology will facilitate early, noninvasive screening of at-risk patients and allow providers to identify and treat patients to prevent the development of HO.
Footnotes
Acknowledgments
The authors acknowledge K. Kessell and members of the units for laboratory animal medicine at the University of Michigan and the Uniformed Services University of the Health Sciences (USUHS) for outstanding animal care. The authors sincerely acknowledge Ms. Shalini Jaiswal at the Translational Imaging Facility at USUHS for MicroCT imaging protocol development. The authors acknowledge Joey Greenstein and Reagan Nelson for mouse MicroCT imaging and analysis.
Author Disclosure Statement
The authors have nothing to disclose and declare no relevant conflicts of interest.
Disclaimer
The contents of this publication are the sole responsibility of the author(s) and do not necessarily reflect the views, opinions, or policies of Uniformed Services University of the Health Sciences (USUHS), The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., the Department of Defense (DoD), and the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
Funding Information
N.J.E. was supported by a Ruth L. Kirschstein Institutional National Research Service Award Postdoctoral fellowship (T32-HD007505). A.L.S. was supported by Ruth L. Kirschstein Institutional National Research Service Award Postdoctoral fellowship (T32-CA009672). GEH was supported by Plastic Surgery Foundation Research Fellowship Grant. B.L. was supported or partially supported by National Institutes of Health (NIH) R01GM123069, R01AR071379, American College of Surgeons Clowes Award, and US Department of Defense Grant W81XWH-18-1-0653 (OR170174). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.