
Abstract
Stem cell therapy holds promise for Parkinson’s disease (PD). To identify optimal stem cell regimens in PD mouse models and inform translational research, we conducted a network meta-analysis (NMA). Specifically, we systematically searched for studies on stem cell therapy in PD mouse models up to September 2024 in PubMed, Embase, Scopus, Web of Science, China National Knowledge Infrastructure, WANFANG, and VIP. Based on the data collected, we conducted an NMA using GeMTC-0.14.3 software. The results of traditional meta-analysis of 148 studies demonstrated superior efficacy of most interventions versus controls at biweekly intervals (2–8 weeks post-treatment), with neural stem cells engineered with neurotrophic factors (NSC-NFs) showing the lowest weighted mean difference, indicating optimal therapeutic effect. NMA demonstrated that NF-engineered NSC therapy ranked the highest at biweekly time points (2–8 weeks post-treatment). Doses of 105 cells showed optimal efficacy at 2, 4, and 6 weeks, peaking within this range, whereas doses of 103 cells showed the best efficacy at 8 weeks. Medial forebrain bundle (MFB) administration showed superior efficacy at weeks 2 and 8, while striatum (STR) infusion showed greater therapeutic effects at weeks 4 and 6, with both approaches significantly outperforming nasal and intravenous delivery at all evaluated time points (2, 4, 6, and 8 weeks). Taken together, these results suggest that NSC-NF (dosage of 105) delivered via MFB (at 2 and 8 weeks) or STR (at 4 and 6 weeks) may represent the optimal strategy. It provides important guidance for optimizing preclinical and clinical trial designs and offers valuable insights for clinical translation.
Introduction
Parkinson’s disease (PD) is one of the most common chronic neurodegenerative diseases, primarily characterized by resting tremors, bradykinesia, rigidity, and postural instability. The disease was first described in the 19th century as “shaking palsy.” 1 In 2014, the International Parkinson and Movement Disorder Society working group defined Parkinson’s disease as “a core clinical motor syndrome (Parkinson’s disease), accompanied by neurodegeneration of the substantia nigra (SN) and synuclein deposits.” 2 The disease has an incidence rate of approximately 572 cases per 100,000 people in those aged 45 and older. 3 After adjusting for age and sex, its mortality rate is approximately 60% higher than that of the general population. In the United States, its economic burden is projected to rise from $52 billion in 2017 to $79 billion in 2037. 4
In PD animal model studies, behavioral assessments are an important means of measuring therapeutic effects. The rotation test is one of the most commonly used methods for evaluating motor function in PD mouse models. In the unilateral 6-hydroxydopamine (6-OHDA) lesion model, due to the unilateral damage to the nigrostriatal pathway, animals treated with dopamine receptor agonists (such as apomorphine) exhibit contralateral rotational behavior, with the number of rotations reflecting the extent of damage to the nigrostriatal dopaminergic (DA) neurons. 5 By measuring the changes before and after the rotation test, the therapeutic effects of treatments such as stem cell transplantation on PD symptoms can be objectively evaluated.
Although PD was initially considered sporadic, increasing evidence suggests that it has a significant genetic component, which may contribute to or affect 10% to 25% of cases, particularly in younger patients. 6 Other potential mechanisms include the Braak hypothesis, 7 which suggests that PD pathology may actually originate in the nasal or gut neurons and eventually spread from these more peripheral regions to the central nervous system (CNS). In addition, mutations in PARKIN and PINK1 have been reported to be associated with impaired lysosomal degradation of dysfunctional mitochondria. 8 Furthermore, PARKIN indirectly regulates mitochondrial biogenesis, and exposure to MPTP or rotenone also impacts mitochondrial mechanisms. 9
Currently, the main treatment methods include pharmacotherapy, surgical treatment, and physical rehabilitation. Levodopa (l-Dopa) is the most commonly used drug and can effectively improve the motor symptoms of PD. However, long-term use can lead to diminished efficacy in advanced stages of the disease 10 and the development of l-Dopa-induced dyskinesia. 11,12 In addition, dopamine receptor agonists (such as pramipexole 13 ) and monoamine oxidase B inhibitors (such as selegiline and rasagiline 14 ) are also commonly used in the treatment of PD. In terms of surgical treatment, deep brain stimulation can improve motor symptoms and is suitable for advanced patients who do not respond well to pharmacotherapy. 15 However, its high cost and surgical risks limit its widespread use. While the above treatments can alleviate symptoms, they do not halt the progression of the disease. Therefore, finding therapeutic strategies that can delay or even reverse the pathological damage of PD has become a research focus.
Stem cells have proliferative abilities and can differentiate into various cell types, showing great potential in repairing damaged tissues. In recent years, stem cell therapy has been widely studied as a potential treatment strategy for neurocognitive disorders such as Alzheimer’s disease and PD. 16 Stem cells include mesenchymal stem cells (MSCs), neural stem cells (NSCs), embryonic stem cells (ESCs), and induced pluripotent stem cells (iPSCs). MSCs have a wide range of sources, such as bone marrow, adipose tissue, and umbilical cord, and possess immune-regulatory and differentiation potential, making them widely applied in regenerative medicine. 17 NSCs can differentiate into neurons and glial cells, and are mainly used for nervous system repair. 18 ESCs are derived from blastocysts and are pluripotent, but face ethical concerns. 19 iPSCs are obtained through genetic reprogramming, combining the pluripotency of ESCs with the advantages of personalized treatment, making them the most promising for research. 20
Neurotrophic factor (NF) is a small secretory protein that supports the development, maturation, and survival of neurons. When injected into the brain, NFs can rescue and regenerate specific neuronal populations lost in neurodegenerative diseases, suggesting that it has the potential to cure the disease, not just alleviate symptoms. 21 NFs include nerve growth factor (NGF), brain-derived NF (BDNF), fibroblast growth factor (FGF), neurotrophin-4 (NT-4), and glial cell-derived NF (GDNF). Current research mainly focuses on GDNF. GDNF is the first NF member of the GDNF family ligands, isolated by Lin et al. in 1993 from the rat glial cell line B49. 22,23 Based on the positive effects of GDNF on the survival and morphological differentiation of midbrain DA neurons in culture, GDNF has been proposed as an effective therapeutic agent for the treatment of PD. 12
In conclusion, stem cell therapy and stem cell combined with NF therapy, as emerging strategies for PD treatment, hold promise in overcoming the limitations of traditional therapies and improving treatment outcomes. However, there is still a lack of systematic comparison of different stem cell types and treatment strategies. Therefore, this study aims to provide a scientific basis for the best treatment strategies for PD by conducting a network meta-analysis (NMA) based on animal models to comprehensively evaluate the effects of different stem cell therapies on improving motor function in mouse.
Stem cell-based therapies show promise for PD, but direct comparisons among all treatment options are limited. NMA, an extension of traditional meta-analysis, allows simultaneous comparison of multiple interventions by integrating direct and indirect evidence. 24 Direct evidence comes from randomized controlled trials (RCTs) directly comparing A and B, while indirect evidence is inferred via a common comparator such as C, when A versus C and B versus C trials exist. It can estimate treatment rankings and guide optimal therapeutic choices. 25
The network diagram is a core component of NMA. It visually displays the relationships among interventions—each node represents a treatment, and lines between nodes indicate direct comparisons from RCTs. 26 Within the connected network, relative treatment effects can be estimated between any pair of interventions, allowing for the ranking of all included treatments. The primary estimands in NMA are relative effect measures, such as odds ratios for dichotomous outcomes and standard mean differences 27 for continuous outcomes, calculated within either a Bayesian or frequentist framework. Results are typically presented using league tables or SUCRA (surface under the cumulative ranking curves), which provide the probability of each intervention being among the most effective treatments. 28 The validity of NMA hinges on the following three principles: comprehensive trial inclusion, bias minimization, and transitivity across studies. These are addressed via systematic searches, risk-of-bias tools (e.g., SYRCLE 29 in animal studies, funnel plots), and inconsistency checks such as the node-splitting method. 30
In summary, NMA offers a robust approach to compare multiple treatments when direct evidence is limited, providing reliable insights to guide therapeutic decisions in PD.
Materials and Methods
Study design
In this NMA, we compared the effects of different types of stem cells on the improvement of motor function in PD mouse models. To investigate the optimal transplantation approach, we also ranked the effects of different doses and administration routes. Although data from the rotarod test and TH+ (tyrosine hydroxylase-positive cells) levels were included in the literature screening and suggested some improvement, they were not incorporated into the NMA due to the limited sample size and potential small-sample bias. This systematic review and NMA were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. We did not register a protocol for the review.
Search strategy
Using the search terms “Parkinson disease” and “stem cell,” or “帕金森” and “干细胞” in Chinese, a comprehensive search was conducted in PubMed, Embase, Scopus, Web of Science, China National Knowledge Infrastructure, WANFANG Database, and Chinese Scientific Journal Database (CSJD-VIP) for studies on stem cell therapy in PD mouse models from initiation to September 2024. To identify any additional potentially relevant studies, gray literature, reference lists of the included articles, and pertinent systematic reviews were manually searched. The full texts of the articles were accessed through the university library’s electronic resources. The full search strategy for each database can be found in Supplementary Table S1 in the Supplementary Data. All citations and abstracts of the retrieved studies were imported into EndNote X9 (Clarivate Analytics, Philadelphia, PA, USA) for removal of duplicates.
Inclusion and exclusion criteria
Inclusion criteria included the following points: Original studies specified the topic of mouse PD. Studies using the rotation test or rotarod test or TH+ cell level to assess its efficacy for motor functional recovery. RCTs. Control groups treated with saline or culture medium. Publication in English or Chinese.
Exclusion criteria included the following points: The type of literature specified as conference presentations, reviews, letters, commentaries, etc. Studies involving animal models other than mice, such as pig, monkeys, or other PD animal models. Duplicate or overlapping data. Clinical trial.
Study selection
Two independent reviewers evaluated the titles, abstracts, and full texts of studies retrieved from the databases. After screening, the results were imported into EndNote for comparison and discussion. Any disagreements were resolved through consensus, and a third reviewer was consulted if necessary to ensure uniformity in applying the inclusion criteria and data extraction process.
Data extraction
Two trained reviewers independently extracted data using a pre-established checklist. In cases of disagreement, consensus was reached, and a third reviewer was consulted if necessary. To ensure consistency, a preliminary test of the data extraction sheet was conducted on a small sample of studies (n = 5). The following key data were extracted: Study information: Authors, title, publication year, journal, and research location. Participant information: Animal species, age, sex, weight, and modeling technique. Stem cell information: Type and source of stem cells used. Study design: Sample size, dosage, route of administration, treatment interval, follow-up duration, and control group treatment method. Outcome measures: Rotation tests, rotarod tests, and DA neuron (TH+ cell) levels.
Risk of bias and quality of evidence
The risk of bias in the included studies was independently assessed by two trained reviewers using the SYRCLE Risk of Bias Tool, specifically designed for systematic reviews of non-human experimental studies. The following domains were evaluated: selection bias, performance bias, detection bias, and attrition bias. The outcomes were classified as follows: Low risk of bias: “Yes.” High risk of bias: “No.” Unclear information: “Unclear.”
Statistical analysis
Traditional meta-analysis
Data analysis was performed using STATA 16.0 software. Effect size data were treated as continuous variables, and weighted mean differences (WMD) with 95% confidence intervals (CIs) were calculated. Heterogeneity between studies was assessed using the χ2 test with a significance level of P = 0.1. The I 2 statistic was used to quantify the degree of heterogeneity. If no significant heterogeneity was detected, a fixed-effect model was applied; otherwise, a random-effects model was used after eliminating obvious clinical heterogeneity factors, with statistical significance set at P = 0.05.
Network meta-analysis
A Bayesian meta-analysis was conducted using GeMTC-0.14.3 software (MRC Biostatistics Unit, Cambridge, UK), with the Markov chain Monte Carlo method applied to assess the data based on a Bayesian model for NMA. The initial iteration number was set to 50,000, with 4 chains and an initial value scaling set to 2.5, and 20,000 iterations for optimization. Inconsistency between direct and indirect evidence was assessed utilizing the node-splitting method, where an indicating P value >0.05 indicated no significant inconsistency. Direct evidence and indirect evidence inconsistency was assessed using a node-splitting model, and the differences between the two were calculated. The potential scale reduction factor (PSRF) was used to test the convergence of the results. A PSRF value close to or equal to 1 indicates that the model has fully converged and is stable, making the analysis results reliable. The NMA was conducted using a consistency model, with a significance level set at P < 0.05. 31 To visually display the available evidence, network diagrams were constructed. In these diagrams, each node corresponds to a specific intervention or comparator. The relative number of studies comparing two connected nodes is indicated by the size of the nodes and the thickness of the lines connecting them. The interventions for each outcome were ranked based on the SUCRA. 32,24 SUCRA values range from 0% to 100%, where higher values indicate a greater likelihood of a treatment being in the top rank or among the highest ranks. 33 Graphs were generated using the network command in STATA 16.0 software (StataCorp LP, College Station, TX, USA) to identify evidence plots, compare different interventions, and detect potential publication bias.
Sensitivity analysis
Funnel plots were generated to detect potential biases and small-study effects.
Results
Literature search results
A total of 42,516 relevant studies were identified. After removing duplicates, 22,025 studies remained, including 18,403 English articles and 3,622 Chinese articles. Studies that did not meet the inclusion criteria were excluded, and an additional nine articles were identified by reviewing the references of relevant reviews. Finally, 148 articles were included, with 130 in English and 18 in Chinese. The literature search flow for the included studies is shown in Fig 1.
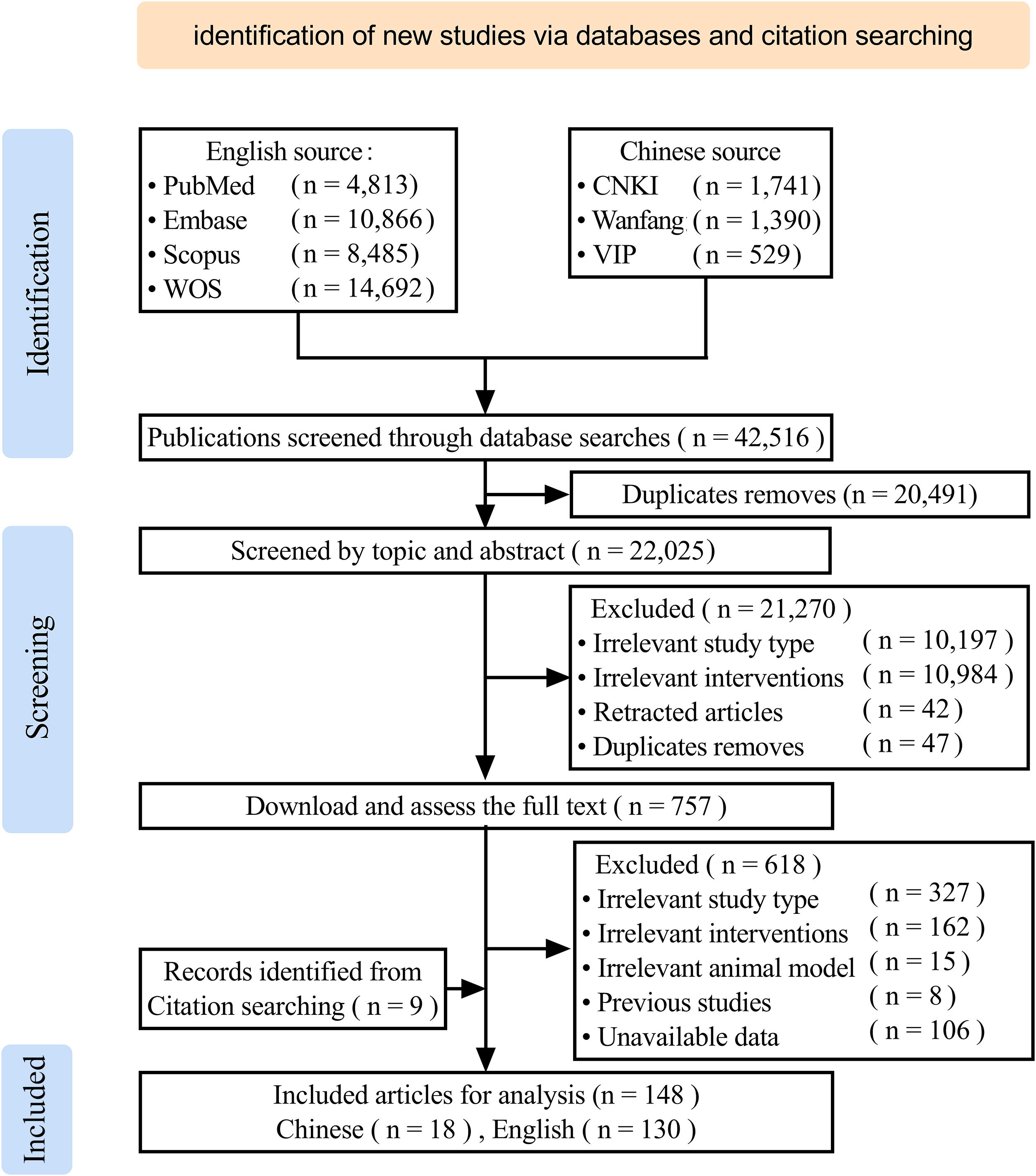
Literature search flowchart.
Inclusion criteria of the studies
Among the 148 included studies, all were randomized controlled trials. The strains of mouse included Sprague–Dawley (74 studies), C57BL/6 (30 studies), Wistar (29 studies), BALB/C (3 studies), Swiss (3 studies), 129/SV (2 studies), albino rat (1 study), C3H/HeN (1 study), Fisher344 (1 study), FVB/N (1 study), and NOD/SCID (1 study), with 2 studies not specifying the mouse strain. The sex of the mouse included male (90 studies), female (35 studies), both male and female (5 studies), and 18 studies did not specify the sex of the mouse. The mouse weighed between 20 and 350 g, of ages from 4 weeks to 20 months, and the sample sizes ranged from 6 to 81 mouse. The modeling method included 6-OHDA (114 studies), MPTP (25 studies), rotenone (8 studies), and 1 study utilized ASO technology, as shown in Fig. 2A.
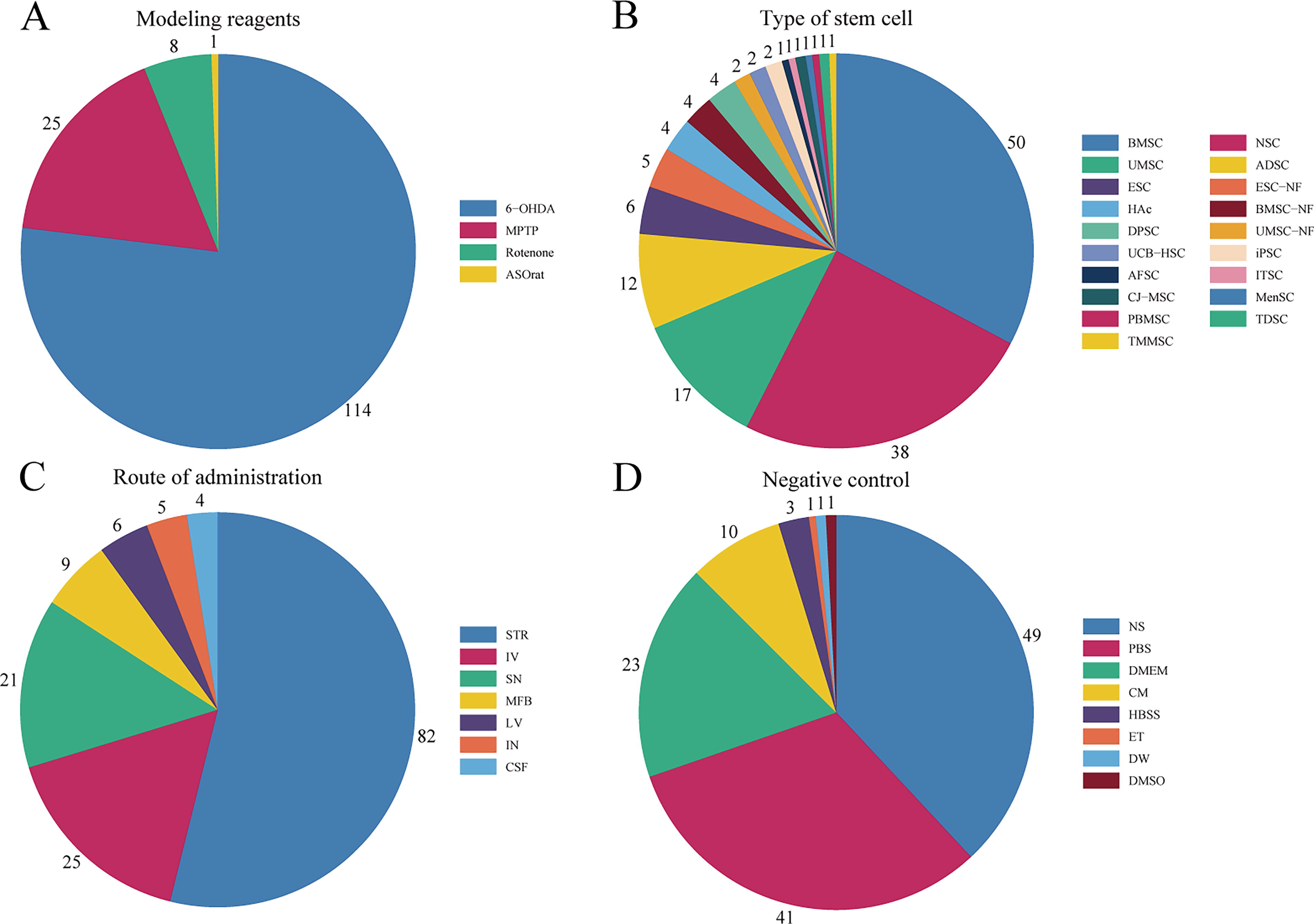
Basic characteristics of the included studies. [
The included studies involved 21 types of stem cells, including bone marrow MSCs (BMSCs, 49 studies), NSCs (38 studies), umbilical MSCs (UMSCs, 17 studies), adipose-derived stem cells (ADSCs, 11 studies), BMSC-NFs (10 studies), ESC-NFs (6 studies), ESCs (5 studies), NSCs-NFs (5 studies), dental pulp stem cells (DPSCs, 4 studies), human amniotic cells (HAc, 5 studies), ADSCs-NFs (3 studies), iPSCs (2 studies), umbilical cord blood hematopoietic stem cells (UCB-HSC, 2 studies), UMSCs-NFs (2 studies), conjunctiva-derived MSCs (1 study), DPSCs-NFs (1 study), inferior turbinate-derived stem cells (ITSCs, 2 studies), ITSCs-NFs (1 study), menstrual blood-derived endometrial stem cells (1 study), peripheral blood MSCs (PBMSCs, 1 study), trabecular meshwork-derived MSCs (1 study), as shown in Fig. 2B.
The transplantation routes included striatum (STR, 82 studies), intravenous injection (IV, 25 studies), SN (21 studies), medial forebrain bundle (MFB, 9 studies), lateral ventricle (LV, 6 studies), intranasal injection (IN, 5 studies), and cerebrospinal fluid (CSF, 4 studies), as shown in Fig. 2C.
The negative controls included sodium chloride solution (49 studies), phosphate-buffered saline (41 studies), Dulbecco’s modified Eagle’s medium (23 studies), cell culture medium (10 studies), Hank’s Balanced Salt Solution (3 studies), dimethyl sulfoxide (1 study), distilled water (1 study), and ethanol (1 study), as shown in Fig. 2D.
Complete information of the included studies can be found in Supplementary Table S2 in the Supplementary Data.
Risk-of-bias assessment
All the 148 studies included were randomized controlled trials, but only 6.08% (9/148) reported the use of random number tables or computer randomization to randomize experimental animals. Only one study implemented concealed group allocation, and one study blinded the animal handlers and researchers. A total of 95.27% (141/148) of the studies clearly reported baseline characteristics of the rats, such as age, sex, and weight. A total of 50.68% (75/148) of the studies reported the random placement of rats during the experiment. Due to limited information provided by the included studies, it was not possible to determine if animals were randomly selected for outcome measurement. All experimental results were objective data, so the risk of bias for blinding was considered low. A total of 93.24% (138/148) of the studies included all rats in the final analysis. Original data were unavailable for all studies, but all the expected outcomes were clearly reported. The risk-of-bias assessment results are shown in Fig. 3. The detailed risk-of-bias assessment for all studies can be found in Supplementary Table S3 in the Supplementary Data.
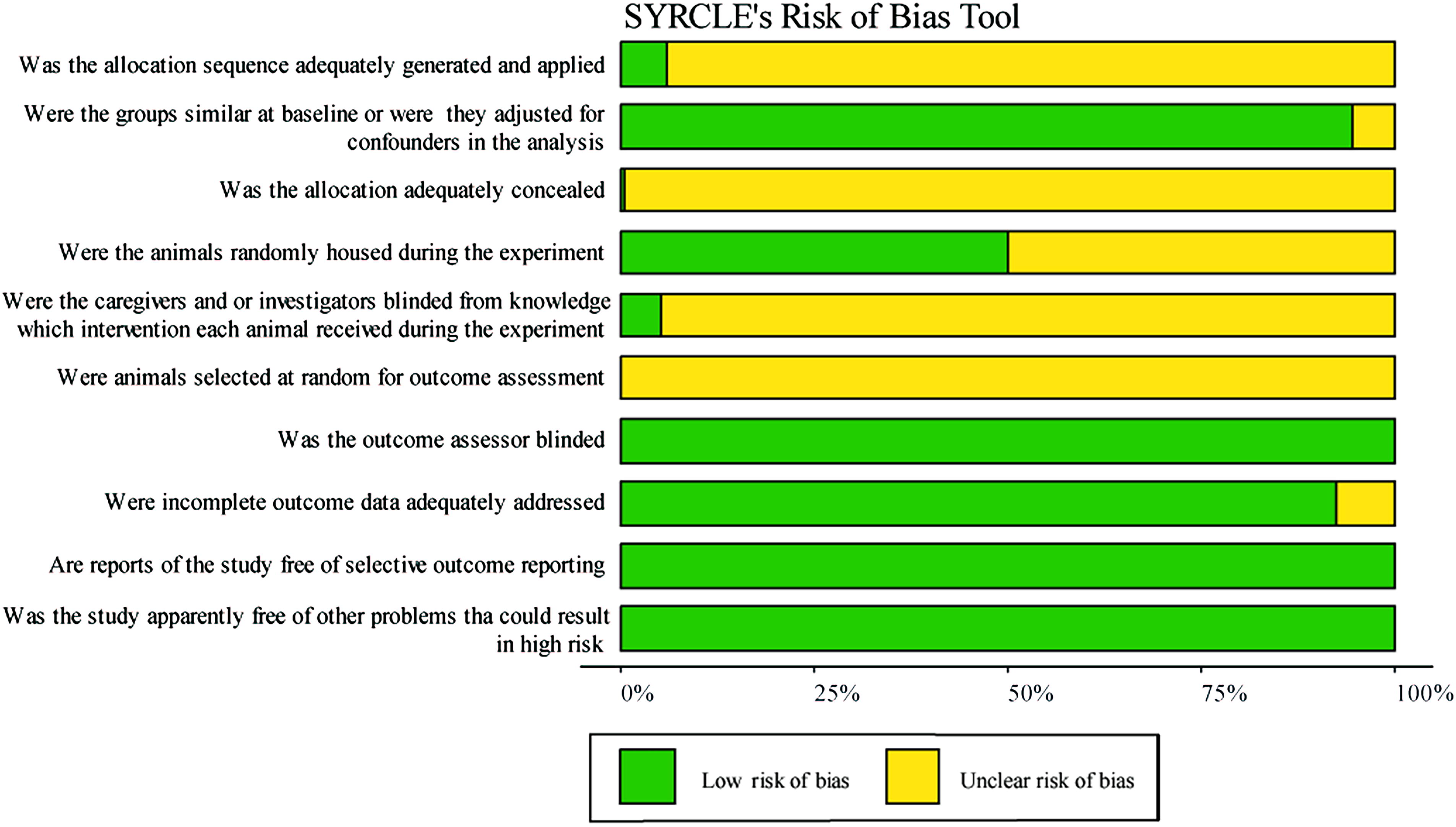
Risk-of-bias assessment results.
Traditional meta-analysis results of 21 different types of stem cells
Second week after stem cell therapy
In the 148 studies included, 77 reported the results of the rotation test in rats at 2 weeks after stem cell therapy, involving 12 types of stem cells as follows: ADSC, ADSC-NF, BMSC, BMSC-NF, DPSC, ESC, ESC-NF, HAc, NSC, NSC-NF, UMSC, and UMSC-NF. The results of the meta-analysis based on a random-effects model indicated that, except for DPSC and UMSC-NF, the rotation counts of the other stem cells were significantly lower than that of the negative control group, with statistically significant differences. Comparing the WMD of different stem cells, the results suggested that NSC-NF appeared to have the best therapeutic effect, which was further verified in the subsequent NMA. See Supplementary Table S4 in the Supplementary Data.
Fourth week after stem cell therapy
In the 148 studies included, 86 reported the results of the rotation test in rats at 4 weeks after stem cell therapy, involving 12 types of stem cells as follows: ADSC, ADSC-NF, BMSC, BMSC-NF, DPSC, ESC, ESC-NF, HAc, NSC, NSC-NF, UMSC, and UMSC-NF. The results of the meta-analysis based on a random-effects model indicated that, except for ADSC and ADSC-NF, the rotation counts of the other stem cells were significantly lower than that of the negative control group, with statistically significant differences. Comparing the WMD of different stem cells, the results suggested that NSC-NF appeared to have the best therapeutic effect, which was further verified in the subsequent NMA. See Supplementary Table S5 in the Supplementary Data.
Sixth week after stem cell therapy
In the 148 studies included, 59 reported the results of the rotation test in rats at 6 weeks after stem cell therapy, involving 12 types of stem cells as follows: ADSC, ADSC-NF, BMSC, BMSC-NF, DPSC, ESC, ESC-NF, HAc, NSC, NSC-NF, UMSC, and UMSC-NF. The results of the meta-analysis based on a random-effects model indicated that, except for ADSC, the rotation counts of the other stem cells were significantly lower than that of the negative control group, with statistically significant differences. Comparing the WMD of different stem cells, the results suggested that NSC-NF appeared to have the best therapeutic effect, which was further verified in the subsequent NMA. See Supplementary Table S6 in the Supplementary Data.
Eighth week after stem cell therapy
In the 148 studies included, 69 reported the results of the rotation test in rats at 8 weeks after stem cell therapy, involving 10 types of stem cells as follows: BMSC, BMSC-NF, DPSC, ESC, ESC-NF, HAc, NSC, NSC-NF, UMSC, and UMSC-NF. The results of the meta-analysis based on a random-effects model indicated that the rotation counts of all stem cells were significantly lower than that of the negative control group, with statistically significant differences. Comparing the WMD of different stem cells, the results suggested that NSC-NF appeared to have the best therapeutic effect, which was further verified in the subsequent NMA. See Supplementary Table S7 in the Supplementary Data.
NMA results
Second week after stem cell therapy
A total of 77 studies were included in the NMA of the rotation test. The evidence network showed that direct comparisons existed between BMSC and BMSC-NF, NSC and NSC-NF, ADSC and ADSC-NF, as well as ESC and ESC-NF, while no direct comparisons were found among other stem cell types. NSC was the most studied stem cell type, as shown in Fig. 4A. The results of the NMA indicated that, compared with the negative control, the SUCRA for NSC-NF was approached 1, as shown in Supplementary Fig. S2 in the Supplementary Data. The ranking results also suggested that NSC-NF might be the most effective stem cell therapy for PD, consistent with the findings of the traditional meta-analysis, as presented in Supplementary Table S8 in the Supplementary Data. The corrected funnel plot was generally symmetrical, indicating a low likelihood of publication bias and small-sample effects, as shown in Fig. 5A.
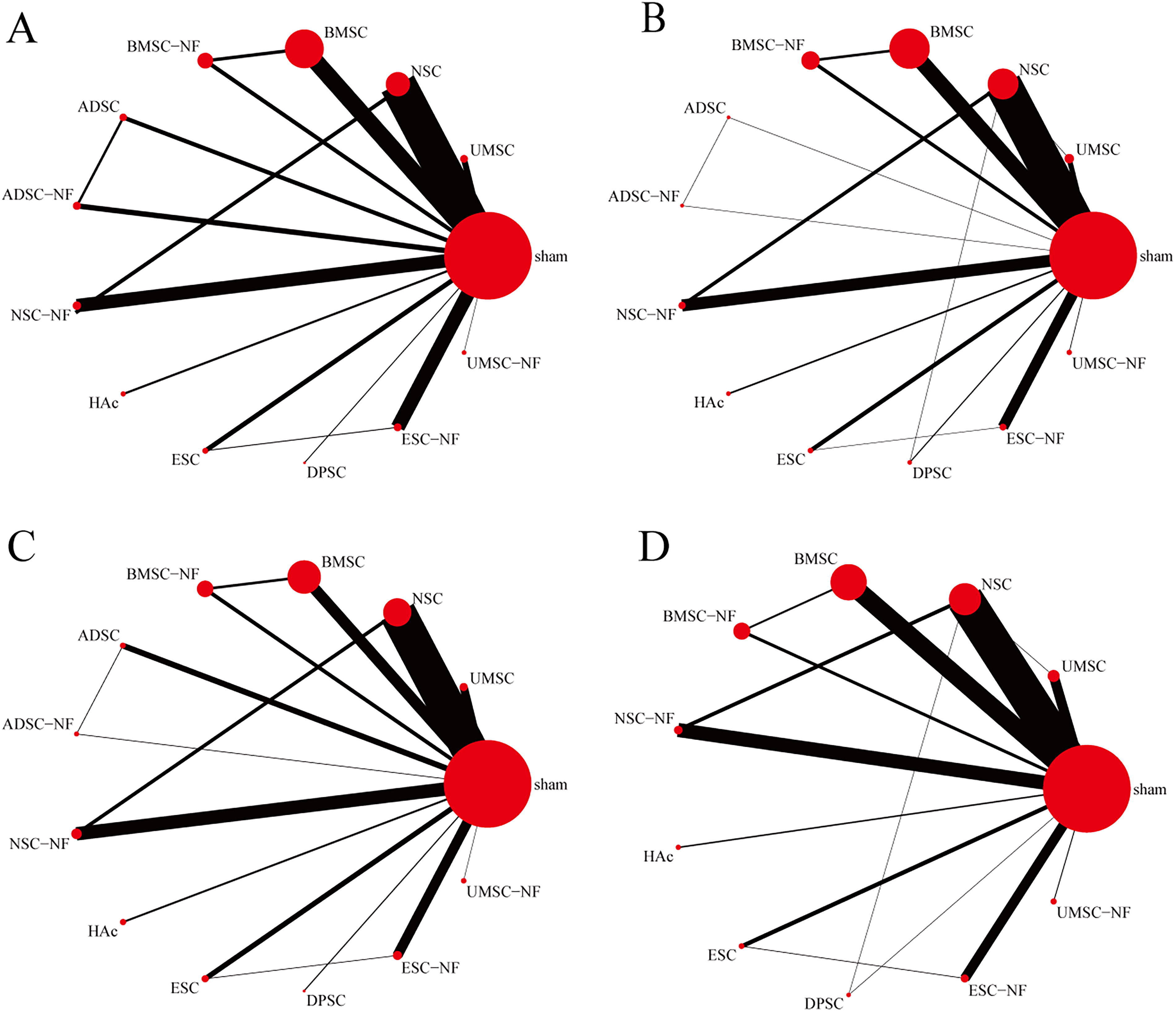
Evidence network diagram [
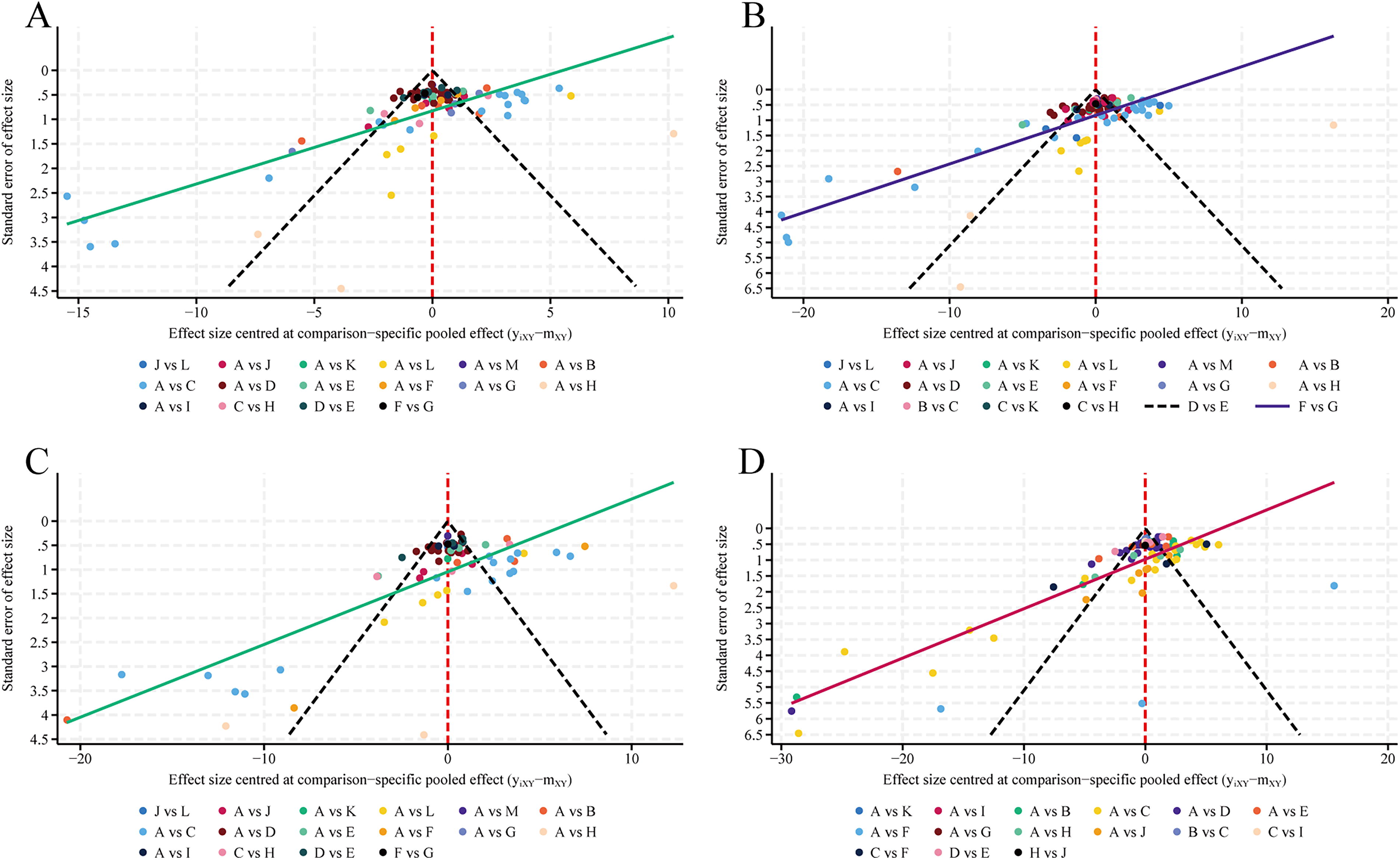
Comparison-adjusted funnel plot [
Fourth week after stem cell therapy
A total of 86 studies were included in the NMA of the rotation test. The evidence network showed that direct comparisons existed between BMSC and BMSC-NF, NSC and NSC-NF, ADSC and ADSC-NF, ESC and ESC-NF, as well as DPSC and NSC, while no direct comparisons were found among other stem cell types. NSC was the most studied stem cell type, as shown in Fig. 4B. The results of the NMA indicated that, compared with the negative control, the SUCRA for NSC-NF was approached 1, as shown in Supplementary Fig. S3 in the Supplementary Data. The ranking results also suggested that NSC-NF might be the most effective stem cell therapy for PD, consistent with the findings of the traditional meta-analysis, as presented in Supplementary Table S9 in the Supplementary Data. The corrected funnel plot was generally symmetrical, indicating a low likelihood of publication bias and small-sample effects, as shown in Fig. 5B.
Sixth week after stem cell therapy
A total of 59 studies were included in the NMA of the rotation test. The evidence network showed that direct comparisons existed between BMSC and BMSC-NF, NSC and NSC-NF, ADSC and ADSC-NF, as well as ESC and ESC-NF, while no direct comparisons were found among other stem cell types. NSC was the most studied stem cell type, as shown in Fig. 4C. The results of the NMA indicated that, compared with the negative control, the SUCRA for NSC-NF was approached 1, as shown in Supplementary Fig. S4 in the Supplementary Data. The ranking results also suggested that NSC-NF might be the most effective stem cell therapy for PD, consistent with the findings of the traditional meta-analysis, as presented in Supplementary Table S10 in the Supplementary Data. The corrected funnel plot was generally symmetrical, indicating a low likelihood of publication bias and small-sample effects, as shown in Fig. 5C.
Eighth week after stem cell therapy
A total of 69 studies were included in the NMA of the rotation test. The evidence network showed that direct comparisons existed between BMSC and BMSC-NF, NSC and NSC-NF, ESC and ESC-NF, NSC and DPSC, as well as NSC and UMSC, while no direct comparisons were found among other stem cell types. NSC was the most studied stem cell type, as shown in Fig. 4D. The results of the NMA indicated that, compared with the negative control, the SUCRA for NSC-NF was approached 1, as shown in Supplementary Fig. S5 in the Supplementary Data. The ranking results also suggested that NSC-NF might be the most effective stem cell therapy for PD, consistent with the findings of the traditional meta-analysis, as presented in Supplementary Table S11 in the Supplementary Data. The corrected funnel plot was generally symmetrical, indicating a low likelihood of publication bias and small-sample effects, as shown in Fig. 5D.
Optimal stem cell therapy strategy for PD
Through traditional meta-analysis and NMA, we found that NSC-NF might be the most effective stem cell type for treating PD at the 2, 4, 6, and 8 weeks after transplantation. To investigate the effects of different transplantation routes and dosages, we conducted two additional NMAs, which indicated the following.
NMA of stem cell dosage
We found that at the 2, 4, and 6 weeks, a dosage of 105 stem cells might be the most effective, whereas at 8 weeks, a dosage of 103 stem cells might be the most effective, with a dosage of 105 stem cells ranked second. Moreover, across all four time points, the group receiving the highest doses (dosage of 107 or 106 stem cells) consistently showed only slightly better efficacy than the placebo, as shown in Supplementary Table S12 and Supplementary Fig. S1 in the Supplementary Data. Therefore, we speculate that as the stem cell dosage increases by orders of magnitude, the therapeutic effect may initially improve but then decline. The optimal dosage might be a dosage of 105 stem cells, which requires further experimental validation.
NMA of stem cell administration routes
We found that at the 2, 4, 6, and 8 weeks, the most effective administration routes were MFB, STR, STR, and MFB, respectively. In addition, IN and IV administration showed less efficacy, as shown in Supplementary Table S13 and Supplementary Fig. S1 in the Supplementary Data. Similarly, further experiments are needed to confirm the specific efficacy differences among these administration routes.
Discussion
Summary of main results
Results of the meta-analysis
The traditional meta-analysis demonstrated improved rotational behavior in PD mouse models across most stem cell therapies compared with sham controls, with therapeutic inefficacy observed in DPSC and UMSC-NF groups at week 2, ADSC and ADSC-NF groups at week 4, and ADSC group at week 6. NSC-NF exhibited superior therapeutic effects across all temporal evaluation points compared with other interventions. These findings align with studies by Li, K et al. 34 and Liu, J et al., 35 which highlight the therapeutic potential of NSC-based strategies in PD.
Although various stem cell therapies show preclinical efficacy in alleviating behavioral deficits in PD mouse models, significant methodological heterogeneity remains in terms of stem cell types and delivery parameters (dose, route). Existing meta-analyses have focused primarily on comparisons with sham controls, without evaluating differences between stem cell therapies or delivery parameters. This limitation prevents a comprehensive comparison of therapeutic efficacy across approaches, underscoring the need for an NMA.
Results of NMA
In this study, we evaluated the therapeutic effects of sham, UMSC, NSC, BMSC, BMSC-NF, ADSC, ADSC-NF, NSC-NF, HAc, ESC, DPSC, ESC-NF, and UMSC-NF on PD mouse models using the rotation test. Studies containing experimental groups with fewer than five animals per group were excluded to mitigate potential small-sample bias. In addition, we investigated the optimal dosage and administration routes.
The NMA revealed that NSC-NF consistently ranked the highest in therapeutic efficacy at 2, 4, 6, and 8 weeks. This is consistent with studies by Yifeng Zheng et al., 36 which suggest that NSCs enhance the therapeutic potential for PD compared with mesenchymal lineages, owing to their multipotent differentiation capacity into midbrain-specific DA phenotypes. 37 Furthermore, NSC-NF exhibited enhanced therapeutic efficacy compared with native NSC, potentially mediated by targeted delivery of NFs (e.g., GDNF, BDNF, and NGF) to the affected brain regions, which promote neuronal survival and functional recovery in parkinsonian pathology. 38 Notably, a meta-analysis by Park et al. 39 also revealed that MSC-NFs exhibit superior motor recovery and DA neuron preservation compared with native MSCs in PD models, mirroring the enhanced efficacy of NSC-NF observed in our current study.
NMA of cell dose optimization identified temporal-specific efficacy thresholds across intervention phases as follows: 105 cells demonstrated peak efficacy at 2, 4, and 6 weeks, while 103 cells achieved optimal therapeutic outcomes at 8 weeks. Dose–response modeling revealed a potential critical threshold at 105 cells during early-to-mid intervention phases (2–6 weeks), warranting further validation in standardized preclinical models.
NMA of administration routes identified distinct efficacy rankings across time points as follows: MFB administration was most effective at 2 and 8 weeks, while STR delivery showed optimal outcomes at 4 and 6 weeks. IV administration ranked lower in efficacy, likely due to biological barriers, including liver sequestration and blood–brain barrier (BBB) restrictions. IN delivery exhibited inconsistent dosing precision across studies, as demonstrated in the study of Andrzejewska et al. 13
Optimal strategy for stem cell therapy
The clinical application of stem cell therapy remains preliminary, 40 despite over 40 registered clinical trials investigating various stem cell types (ClinicalTrials.gov). Direct comparisons of therapeutic parameters (cell types, dosage, and administration routes) have been challenging in clinical trials, highlighting the need for systematic preclinical optimization. For instance, Venkataramana et al. 41 administered autologous BM-derived MSCs via stereotactic surgery to seven PD patients at 106 MSCs/kg. In a subsequent 2012 pilot trial, the same team reported that 16 Parkinson’s patients received the same dosage of allogeneic BM-derived MSCs. 42 These studies highlight the feasibility of stem cell therapy for PD but emphasize that large-scale clinical trials are challenging.
To address this issue, we included studies examining stem cell therapy in PD mouse models in this study, encompassing various stem cell types such as MSCs, NSCs, ESCs, and iPSCs. These studies explored multiple administration routes, including IV injection, IN delivery, and intracranial transplantation at different brain regions. In addition, stem cell dosages ranged from 103 to 107 cells, providing a comprehensive basis for evaluating therapeutic efficacy.
The results of this study suggest that NSC-NF delivered via MFB or STR administration as a superior therapeutic strategy in PD rats. In addition, doses below 103 cells proved insufficient, while doses higher than 106 cells provided no additional benefits. In contrast, dosages between 104 and 105 appeared optimal, aligning with the findings of Rajesh et al. 43 These findings provide a preclinical framework for advancing stem cell therapy toward clinical translation, requiring validation of this optimized strategy in human trials.
Advantages of NSC therapy
NSC transplantation has indicated its ability to promote repair and functional recovery of damaged neural tissue in PD. Traditional drug and surgical treatments primarily slow disease progression without halting or reversing it. As PD progresses, the therapeutic effects of these treatments tend to diminish. In contrast, NSC therapy offers restorative potential. NSCs self-renew and differentiate into various neural cells, including neurons, astrocytes, and oligodendrocytes, which may replace lost neurons and restore motor function. 44 This makes NSC therapy a promising approach for therapeutic intervention, offering the possibility of long-term recovery rather than just symptom management.
Studies by Zhang et al. 45 and Watanabe et al. 46 have demonstrated that NSC transplantation can slow PD progression, restore brain function, and improve neurological outcomes without significant complications. In addition, research by Ryu et al. 47 revealed that NSCs can migrate to damaged areas, promoting endogenous neurogenesis and angiogenesis in the ischemic rat brain. Furthermore, NSCs exhibit immunomodulatory effects, including the secretion of cytokines, chemokines, and chemokine receptors, as well as inhibition of T cell proliferation. 48
Furthermore, preliminary clinical safety studies by Jiang, S. 49 and Garitaonandia, I. 50 suggest that NSC transplantation carries a low risk of tumor formation due to restricted differentiation along the neural lineage and minimal immune rejection, with no serious adverse effects reported. These findings provide strong evidence for the potential of NSCs in treating neurodegenerative diseases. However, further clinical trials are necessary to comprehensively assess their long-term effects and efficacy.
There have also been preliminary clinical trials investigating other types of stem cell therapy for PD, primarily focusing on MSC treatment. 51,38 Although MSC therapy has shown potential, it faces challenges such as low differentiation into DA neurons. 32 In contrast, NSCs differentiate more efficiently into DA neurons and possess stronger neurorepair capabilities. As a result, NSCs have emerged as one of the most promising stem cell types for PD treatment.
GDNF augments the efficacy of NSC therapy
In 1993, Lin et al. 52 discovered that certain factors could significantly enhance the survival and differentiation of DA cells, offering new hope for treating neurodegenerative diseases such as PD. Grondin et al. 53 built on this by showing that long-term infusion of GDNF into the LV or STR can restore the nigrostriatal DA system and significantly improve motor function in parkinsonian monkeys. This laid a solid theoretical foundation for GDNF’s potential in PD treatment.
Moreover, GDNF has been shown to protect DA neurons in the SN from degeneration and to improve motor function. In a study by Tereshchenko et al., 54 GDNF effectively alleviated motor deficits in rats with 6-OHDA-induced neurotoxin damage, further proving its potential in treating PD and other neurodegenerative diseases. GDNF promotes the survival and morphological differentiation of DA neurons, 47 shields DA neurons from certain neurotoxic damage, 55 and demonstrates its significant therapeutic potential for promoting stem cell survival and enhancing treatment outcomes.
In addition, Liu et al. 56 transplanted GDNF-overexpressing c17.2 NSCs into the STR of a PD rat model and found that the group with GDNF expression showed better motor improvements and higher neurotransmitter levels than the control group. Similarly, Sun et al. 57 transplanted HAMSC-GDNF into the STR of a PD rat model, yielding similar promising results. These findings further emphasize GDNF’s potential in PD therapy, particularly when combined with stem cell therapies to facilitate neural repair and restore function.
Challenges and future perspectives in NSC-based therapy
The BBB, a specialized cerebral vascular interface regulating CNS homeostasis through selective permeability, critically impedes therapeutic delivery. 58 In this study, intracranial injection showed significantly better therapeutic effects compared with IV injection, attributable to cell size restrictions impeding trans-BBB transport. Direct intracranial injection ensures more effective delivery to target areas. While intracranial injections are invasive and more complex, requiring careful consideration of patient tolerance, IN administration is a noninvasive method that bypasses the BBB. Although its therapeutic effect is lower than intracranial injection, IN delivery offers ease of administration and higher patient acceptance, making it a promising long-term treatment option, especially for patients unable to tolerate invasive procedures. Thus, IN delivery could serve as an adjunctive treatment.
In clinical applications of NSCs, although initial studies show low tumorigenicity, the pluripotency of stem cells still poses a risk for tumor formation. Stem cells can differentiate into various cell types, including neurons and glial cells, but uncontrolled differentiation could lead to tumor development. Therefore, strict control over stem cell dosage is critical to avoid tumor formation. Our study suggests that the optimal treatment dose for NSCs is between 105 and 106 cells. Higher doses may lead to reduced therapeutic efficacy, potentially due to immune responses or disrupted differentiation patterns. While no significant tumorigenic side effects were reported in the studies included, this could be due to short treatment durations or insufficiently high doses. Further research is needed to determine the optimal dosage, balance efficacy, and minimize risks of tumorigenicity, as well as to identify the ideal treatment window and safe dosages.
Current research explores diverse NSC sources, including MSCs, ESCs, peripheral blood cells, CSF, 59,60 and amniotic fluid. 61,62 Fetal-derived NSCs remain the predominant clinical source, 44 demonstrating multipotent differentiation into neurons, astrocytes, and oligodendrocytes to promoting tissue repair and angiogenesis, 63,64 while secreting NFs that enhance neurogenesis and mitigate inflammation. 65,59 However, the use of human fetal-derived NSCs raises ethical concerns, prompting research on alternatives such as NSCs derived from ESCs, MSCs, and iPSCs. In addition, fibroblasts from adult tissues can be reprogrammed into NSCs, which can differentiate into various neural cell types, including neurons. 66,67 Endogenous NSCs exist in specific regions of the brain, such as the STR, hippocampus, and olfactory bulb, providing additional potential sources for regenerative therapies. These alternative sources avoid ethical concerns and hold significant promise for CNS repair.
Given the variety of potential NSC sources and their promising applications, it is essential to further investigate the most effective treatment strategies for neurodegenerative diseases such as PD. This study, therefore, presents optimal treatment strategies for PD in mouse models, including stem cell types, administration routes, and dosages. However, since animal studies were involved, the treatment window and patient selection remain undefined and warrant further investigation.
This NMA has several limitations. First, the risk of performance bias may exist due to unclear blinding in most of the studies. Second, only the rotation test data were available for evaluating motor function. Although this test provides objective results, it does not offer a comprehensive assessment of treatment efficacy. Third, according to the guidelines by Salanti et al., 24 using the SUCRA ranking graph to rank treatment effects has inherent limitations, and the results should be interpreted with caution. In addition, although the use of NFs has improved the efficacy of stem cell therapy, the exact in vivo mechanisms remain unclear. Despite these limitations, they have been carefully considered in our analysis. First, performance bias risk exists due to unclear blinding in most studies, although peer-reviewed standards mitigate this. Second, as the primary measure of motor function recovery, the rotation test remains valid due to its strong presence in the literature and consistency with DA neuron recovery. Third, while SUCRA has inherent limitations in ranking treatment effects, the consistency of results across different time points in the NMA and the subgroup analyses in the traditional meta-analysis reinforces the reliability of our conclusions. Considering these factors, we categorize the overall risk of bias as “some concerns,” suggesting that these biases were unlikely to influence the results. Therefore, we believe they were unlikely to substantially lower confidence in the study’s conclusions.
Conclusion
Traditional meta-analysis of 21 stem cell types and NMA of 13 stem cell types revealed that NSC-NF may represent the most optimal stem cell type for the treatment of PD. Further analysis showed that an appropriate dosage (ranging from 104 to 105 cells) ranked the highest in efficacy. In addition, the MFB/STR route of administration demonstrated the highest efficacy, significantly outperforming the IN and IV routes. Despite “some concerns” regarding bias, the results are deemed reliable and the conclusions robust. This study aims to investigate the optimal treatment strategy through animal experiments to promote clinical translation, enhance the quality of preclinical research, and reduce the risks associated with clinical drug use.
Footnotes
Acknowledgments
The authors thank Zhengmian Zhang and Zhongquan Qi (corresponding authors) for their guidance and support, and Yingkai Wang (second author) for her contributions.
Informed Consent Statement
The article does not contain clinical studies or patient data.
Author Disclosure Statement
The authors have no competing interests to declare that are relevant to the content of this article.
Funding Information
The research leading to these results received funding from the Joint Funds for the Innovation of Science and Technology, Fujian Province, under Grant Agreement No. 2021Y9189.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.