
Abstract
Abstract
Background:
Ascariasis continues to be one of the most important parasitic diseases in terms of its burden and complications in children in the developing world.
Methods:
Case report and literature review (Medline, SCI, and LILACS).
Results:
We report herein a case in which a Paraguayan infant presented with one of these complications: An intestinal obstruction due to Ascaris lumbricoides being diagnosed during surgery. The patient was managed with a conservative protocol for the extraction of the parasites using liquid petrolatum administered through a nasogastric tube followed with extensive water irrigation through the tube, in conjunction with the administration of piperazine as antiparasitic treatment.
Conclusions:
This case, as with others reported previously, shows that this complication can be managed successfully without major intestinal surgery. Early recognition of this condition, based on local prevalence, can prevent serious surgical complications, morbidity, and mortality associated with intestinal obstruction due to A. lumbricoides.
Case Report
A 13-month-old male infant born in Paraguarí (rural Paraguay) presented with complaints of 11-day evolution of fever (39°C), acute abdominal pain, non-bloody, non-mucoid diarrhea; and vomiting. On admission, he was found to have signs of mild dehydration, diffuse abdominal pain without peritoneal irritation, anemia (hemoglobin, 8.5 g/dL), and leukocytosis (12.0 × 103 cells/mm3, 60% lymphocytes). His anthropometric evaluation revealed short stature (−2 SD) and weight (−1 SD) for his age according to the national growth charts. Abdominal sonogram revealed an intestinal invagination at the ileal region. Abdominal radiography also showed signs of intestinal obstruction (Fig. 1). Surgical exploration via open right transverse infraumbilical laparotomy found a parasite bolus (suggestive of A. lumbricoides) located 1.5 m from the ileocecal valve. The surgical diagnosis was intestinal obstruction due to A. lumbricoides. During abdominal surgery, the parasite bolus was manually displaced to the large intestine (ascending colon). Liquid petrolatum (20 mL) was administered through a nasogastric tube followed with extensive water irrigation in conjunction with the nasogastric administration of piperazine (50 mg/kg per day divided into three doses) as antiparasitic treatment. Adult forms of A. lumbricoides began extensive expulsion through the anus (up to 50 adult parasites in each evacuation) (Fig. 2). Ampicillin–sulbactam was used as antimicrobial prophylaxis for the surgical procedure. Patient evolution was successful, presenting one day later with a systemic allergic reaction (nasal pruritus, cough, cutaneous rash, and pruritus) treated with chlorphenhydramine (0.3 mg/kg per day by mouth). One day later, the patient was discharged.
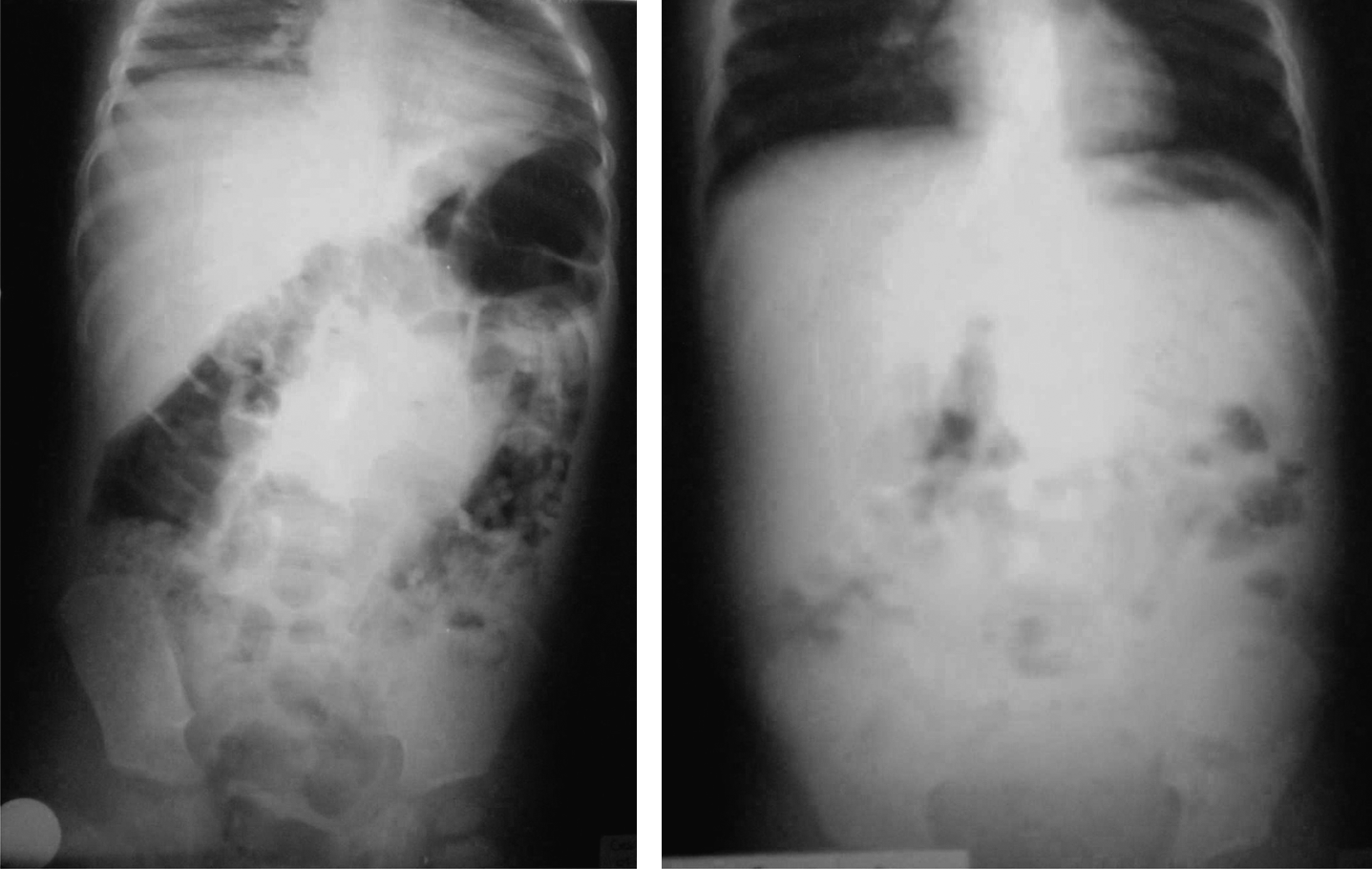
Abdominal radiography images showing signs of intestinal obstruction (left) and after surgical and medical treatment (right).

Moment of one feces evacuation after the protocol using piperazine in which the parasites (adult forms of A. lumbricoides) began to be expelled extensively through the anus (up to 50 adult parasites in each evacuation).
Discussion
Ascariasis is one of the most cosmopolitan intestinal parasite infections but with higher burdens in developing countries in tropical and subtropical areas, sometimes carrying major and even fatal complications such as intestinal obstruction [5]. With variable incidence, intestinal obstruction has been managed effectively conservatively using intravenous fluid, antibiotics, piperazine salt through nasogastric tube, and glycerin plus liquid paraffin emulsion enemas, among other measures, especially in patients who do not have peritonitis [5,6]. More studies in settings with a higher prevalence of ascariasis should be done, considering there are no randomized clinical trials for the management of intestinal obstruction due to A. lumbricoides infection [5,6]. This complication could be managed successfully without major intestinal surgery, especially if early recognition of this condition is achieved. Appropriate epidemiologic evaluation of these cases and conservative management can prevent serious surgical complications, morbidity, and mortality [7].
Footnotes
Acknowledgments
Thanks to Diane Edrington (Long Beach, MS) and Elizabeth Lavoie (Ontario, ON, Canada) for their review of the manuscript.
Author Disclosure Statement
No competing financial interests exist.