
Abstract
Abstract
Background:
Soft-tissue infections traditionally have been viewed as carrying a lower risk of death than other types of infection such as pneumonia, blood stream, and intra-abdominal. The influence of secondary bacteremia on the outcomes of patients with soft-tissue infections is not well described.
Objectives:
To describe the risk factors for bacteremia among patients admitted to an urban medical center with soft-tissue infections and the influence of bacteremia on outcomes.
Methods:
A retrospective cohort study of 717 patients with culture-positive non-necrotizing soft-tissue infections admitted between April 1, 2005, and December 31, 2007.
Results:
Bacteremia was present in 52% of the patients. Increasing age, previous hospitalization, decubitus or lower-extremity ulcers, device-related soft-tissue infection, and polymicrobial infection were independent predictors of bacteremia. Intensive care unit admission (adjusted odds ratio [AOR] 3.57; 95% confidence interval [CI] 2.17, 5.86), lower-extremity ulcer (AOR 3.43; 95% CI 2.07, 5.70), and bacteremia (AOR 6.37; 95% CI 3.34, 12.12) were independent predictors of in-hospital death. When patients with device-related soft-tissue infections were excluded, the rate of secondary bacteremia was 37.6% (201/535), and it remained an independent predictor of in-hospital death.
Conclusions:
The occurrence of bacteremia in soft-tissue infections is associated with a greater risk of death. Health care providers should be aware of the risk factors for bacteremia in patients with soft-tissue infections in order to provide more appropriate initial antimicrobial therapy and to ascertain its presence as a prognostic indicator.
Patients and Methods
Study design
A retrospective cohort analysis was performed of all culture-positive patients admitted to Barnes-Jewish Hospital (a 1,200-bed urban teaching hospital) between April 1, 2005, and December 31, 2007, with a diagnosis of soft-tissue infection.
Data source
Two investigators (VP, JAD) identified all study patients by the presence of either a primary or a secondary ICD-9-CM code indicative of soft-tissue infection and a concomitant positive culture from the site of infection or a positive blood culture (see Appendix). The study database was constructed (by APH) by merging patient-specific data from the automated hospital records and microbiology and pharmacy databases of Barnes-Jewish Hospital.
Definitions
For the purposes of this investigation, soft-tissue infections were limited to non-necrotizing infections and included cutaneous abscesses, furuncles and carbuncles, cellulitis and erysipelas, ulcers, surgical site infections, and device-related infections (including arterial grafts, arteriovenous fistulas or shunts, insulin infusion pumps, peripheral dialysis catheters, and internal orthopedic implants and excluding central venous, Hickman, and peripherally inserted catheters and Port-a-caths) as defined in the recent Infectious Diseases Society of America guidelines [1] (see Appendix Table 1). Device-related infections were included only if there was clinical evidence of soft-tissue infection (e.g., cellulitis, abscess) superficial to the device. Necrotizing infections, including necrotizing fasciitis, clostridial myonecrosis, and pyomyositis, were excluded, as these infections require immediate surgical intervention (see Appendix Table 2).
Health care-associated soft-tissue infection was said to be present in patients admitted to the hospital with a diagnosis of soft-tissue infection who met the following criteria: (1) Admission from a nursing home, rehabilitation hospital, or other long-term nursing care facility; (2) hospitalization within the immediately preceding 12 months; (3) receiving outpatient hemodialysis, peritoneal dialysis, or infusion therapy necessitating regular visits to a hospital-based clinic; and (4) being in an immunocompromised state.
The diagnosis of soft-tissue infection was verified by one of the investigators (STM) from the medical database and required documentation of the site of infection plus at least one of the following: (1) White blood cell count > 10,000 × 103/mL; (2) temperature ≥ 38.3°C; or (3) purulent discharge from the infection site. Acceptable positive culture specimens included abscess drainage, aspirate from the leading edge of a cellulitis lesion or involved soft tissue, surgical biopsy, non-abscess purulent drainage, deep tissue, and purulent discharge from an ulcer or wound. Blood cultures were accepted if the same organism was identified in a soft-tissue culture or no other source for the positive blood culture could be identified. For patients with a device-related infection, confirmation of the presence of overlying soft-tissue infection was confirmed using the electronic medical record.
Data analysis
All comparisons were unpaired, and all tests of significance were two-tailed. Continuous variables were compared using the Student t-test for normally distributed variables and the Mann-Whitney U test for non-normally distributed variables. The chi-square or Fisher exact test was used to compare categorical variables. We performed multiple logistic regression analysis using SPSS Version 11.0 for Windows (SPSS, Inc., Chicago, IL). Multivariable analysis was performed using models judged a priori to be clinically sound. This was determined prospectively to be necessary to avoid producing spuriously significant results with multiple comparisons. All potential risk factors significant at the 0.2 level in univariable analyses were entered in the model.
Results
Patient characteristics
A total of 717 culture-positive patients with soft-tissue infection were admitted to Barnes-Jewish Hospital during the study period. One hundred nine patients (15.2%) had more than one soft-tissue infection identified during the same hospitalization. The mean age of the population was 51.5 ± 17.4 years (range 14–99 years). The study included 374 (52.2%) male and 343 (47.8%) female patients. There were 372 patients (51.9%) with secondary bacteremia, and 527 patients (73.5%) were classified as having a health care-associated infection. The characteristics of the patients with soft-tissue infection segregated by the presence or absence of bacteremia and in-hospital death are provided in Table 1. Hospitalization during the previous 12 months was the most common criterion for classification as a health care-associated infection. Among patients with a device-related infection, 176 (96.7%) had cellulitis and an abscess overlying the device (Table 2).
Includes arterial grafts, arteriovenous fistulas or shunts, insulin infusion pumps, peripheral dialysis catheters, and internal orthopedic implants.
N/A = not available.
Risk factors for bacteremia
Patients with secondary bacteremia were statistically more likely to have a health care-associated infection than were the non-bacteremic patients (Table 1). The health care-associated risk factors that significantly differentiated patients with bacteremia from those without were prior hospitalization, admission from a nursing home or extended care facility, and chronic hemodialysis. Bacteremic patients were significantly more likely to have end-stage renal disease, neutropenia, insulin-requiring diabetes mellitus, underlying malignant disease, cirrhosis, or peripheral vascular disease than were non-bacteremic patients. Bacteremic patients also were significantly more likely to have an infection characterized by a decubitus ulcer, lower-extremity ulcer, device-related infection, gram-negative bacteria, Candida, or polymicrobial infection and less likely to have an abscess with cellulitis, postoperative incisional infection, or gram-positive bacterial infection (Tables 1 and 2).
Patients with bacteremia were significantly more likely to have infection with Enterobacter spp., Escherichia coli, Klebsiella spp., Stenotrophomonas maltophilia, Enterococcus faecalis, Ent. faecium, vancomycin-resistant enterococci, or coagulase-negative staphylococci and less likely to have infection with methicillin-resistant Staphylococcus aureus, the community-associated phenotype of methicillin-resistant S. aureus, or non-group A and B streptococci. Patients with soft-tissue infections associated with bacteremia were significantly less likely to have their culture source be an abscess, tissue aspirate, purulent drainage, tissue, or drainage from an ulcer than were non-bacteremic patients.
Excluding patients with a device-related infection resulted in similar findings. Among the 535 such patients, there were 201 (37.6%) with secondary bacteremia. Patients with device-related soft-tissue infections had a significantly greater incidence of secondary bacteremia than did patients without device-related infections (94.0% vs. 37.6%; p < 0.001). Among patients with a decubitus ulcer, 46 of 87 infections were polymicrobial (52.9%), including 5 (5.7%) associated with polymicrobial bacteremia.
Logistic regression analysis of the entire study cohort identified increasing age, previous hospitalization, decubitus or lower-extremity ulcers, device-related soft-tissue infection, and polymicrobial infection as independent predictors of bacteremia (Table 3). When patients with device-related soft-tissue infections were excluded, being a nursing home resident was an independent predictor of bacteremia, whereas abscess and cellulitis formation and surgical site infection were associated independently with the absence of secondary bacteremia (Table 3).
Other covariates not in the table had a p value > 0.05, including nursing home resident, chronic hemodialysis, insulin-requiring diabetes mellitus, neutropenia, underlying malignant disease, cirrhosis, peripheral vascular disease, abscess and cellulitis on digit, abscess and cellulitis other location, postoperative surgical site infection, gram-negative bacteria, gram-positive bacteria, and Candida spp. (p = 0.419; Hosmer-Lemeshow goodness-of-fit test).
Includes arterial grafts, arteriovenous fistulas or shunts, insulin infusion pumps, peripheral dialysis catheters, and internal orthopedic implants.
Other covariates not in the table had a p value > 0.05, including chronic hemodialysis, insulin-requiring diabetes mellitus, neutropenia, underlying malignant disease, cirrhosis, abscess and cellulitis on digit, and gram-positive bacteria (p = 0.282; Hosmer-Lemeshow goodness-of-fit test).
Risk factors for in-hospital death
Compared with survivors, non-survivors were significantly older, more likely to be nursing home residents, require intensive care unit admission, or have health care-associated infection; underlying malignant disease; a solid organ allograft; a decubitus or lower-extremity ulcer; Candida infection; infection with Ent. faecalis, Ent. faecium, or vancomycin-resistant enterococci; or bacteremia and less likely to have abscess and cellulitis on a location other than a digit, gram-positive bacteria, methicillin-resistant S. aureus, other non-group A and B streptococci, or a causative organism isolated from an abscess (Tables 1 and 2). Logistic regression analysis demonstrated that intensive care unit admission, lower-extremity ulcer, and bacteremia were independently associated with in-hospital death (Table 4). Excluding patients with a device-related infection resulted in the same variables plus underlying malignant disease being identified as independent risk factors for in-hospital death. Kaplan-Meier curves comparing patients with soft-tissue infections with or without bacteremia demonstrated a greater risk of in-hospital death for bacteremic patients (p = 0.007; log-rank test) (Fig. 1). A similar statistically significant difference in the hospital mortality rates of bacteremic and non-bacteremic patients was identified when individuals with device-related soft-tissue infections were excluded (p < 0.001; log-rank test).
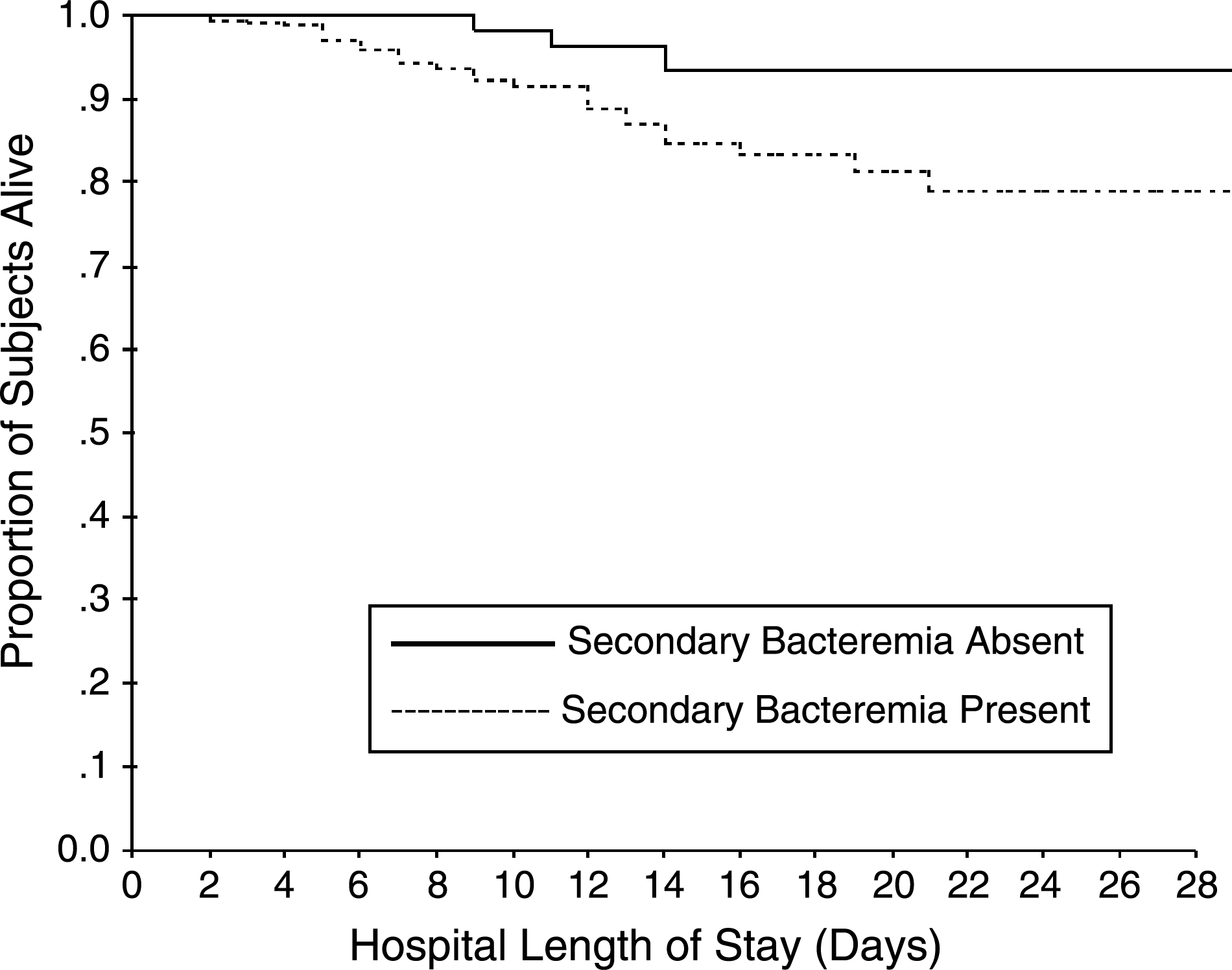
Impact of bacteremia on mortality rate.
Other covariates not in the table had a p value > 0.05, including age, race, health care-associated infection, previous hospitalization (0–3 months), nursing home resident, insulin-requiring diabetes mellitus, underlying malignant disease, solid-organ transplant, abscess and cellulitis other location, decubitus ulcer, gram-negative bacterial infection, gram-positive bacterial infection, and Candida spp. infection (p = 0.787; Hosmer-Lemeshow goodness-of-fit test).
Outcomes analysis
Patients with bacteremia had a greater risk admission to an intensive care unit and of in-hospital death (Table 5). Hospital length of stay was statistically longer for bacteremic patients, and they were less likely to be discharged to home and more likely to be discharged to a nursing home or other acute care facility. Similar results were observed when patients with device-related infections were excluded (Table 5).
Discussion
We showed that bacteremia complicating soft-tissue infections was common among patients admitted to an urban medical center and was associated with excess in-hospital deaths. Logistic regression analysis demonstrated that the occurrence of bacteremia was independently associated with death. We also found that certain risk factors may be associated with bacteremia in patients with soft-tissue infections: Increasing age, previous hospitalization, a decubitus or lower-extremity ulcer, device-related infection, and polymicrobial infection. Additionally, more than half of the soft-tissue infections in our study were classified as health care-associated. Our study addresses a different population from that in other reports of soft-tissue infections [1]. We did this purposefully to evaluate a more inclusive population pertinent to clinicians working in the hospital setting. Patients with bacteremia were statistically more likely to require intensive care unit admission, have longer hospital stays, be discharged to a nursing home or other acute care facility, or die during their hospitalization than were patients without bacteremia.
Clinical assessment of the severity of soft-tissue infections is crucial to ensure that timely and appropriate treatment is administered [1]. Most assessment schemes attempt to differentiate necrotizing from non-necrotizing infections because of the urgent need for surgical intervention in the former [6]. Bacteremia complicating cellulitis has been described previously but has not been shown to be associated with a greater risk of morbidity and death [2–4]. Bacteremia complicating cellulitis caused by non-group A streptococci superimposed on lymphedema occurs in 30% of patients [7]. This high prevalence of bacteremia has been attributed to the lymphedema and the virulence of the infecting bacterial species [8]. Other types of cellulitis involving the buccal or periorbital area, in patients in whom a salt-water or fresh-water source of infection is likely, and in patients with evidence of a systemic inflammatory response, are more likely to be associated with bacteremia [8].
Peralta et al. reviewed the records of patients with limb cellulitis in a teaching hospital to identify predictors of bacteremia [9]. Among 308 patients (among 2,678 patients presenting to the hospital with cellulitis) having blood culture, 57 (18.5%) had bacteremia. Risk factors for bacteremia included absence of previous antimicrobial treatment, presence of two or more co-morbid conditions, length of illness less than two days, and proximal limb involvement. In an accompanying editorial, Eron and Lipsky suggested that clinicians should employ such risk factors to assist in determining when blood cultures should be obtained for patients with cellulitis [10]. Unfortunately, similar studies identifying risk factors for bacteremia in other types of soft-tissue infections are lacking. Jahamy et al. recently demonstrated that bacteremia accompanying S. aureus soft-tissue infections was similar for Panton-Valentine leukocidin (PVL)-positive and -negative isolates [11]. Predictors of bacteremia in their study included age 65 years or greater, necrotizing infection, and head/neck location of the infection.
Our study examined a consecutive group of patients admitted to a large referral hospital with a variety of soft-tissue infections. Other experiences examining soft-tissue infections differ from our study in that they examined specific types of bacteria, geographic locations, or infection types. Sebeny et al. described soft-tissue infections caused by multi-drug resistant Acinetobacter baumannii among soldiers with war wounds [12]. This illustrates the importance of recognizing specific risk factors for infection with highly virulent or resistant pathogens in order to administer appropriate antimicrobial therapy in a timely manner. Similarly, Chang et al. demonstrated that community-onset skin and soft-tissue infections in Taiwan caused by Klebsiella pneumoniae were more likely to be associated with bacteremia and shock than those attributable to other bacteria [13]. Those investigators recommended that in their geographic area, clinicians be aware of this finding in order to initiate broader antimicrobial therapy in patients having skin and soft-tissue infections complicated by shock. Other authors have highlighted the need to recognize that soft-tissue infections associated with foreign bodies can be difficult to treat and often necessitate removal of the foreign body or more protracted antibiotic therapy for success [14,15].
Several important limitations of our investigation should be noted. First, we evaluated only culture-positive infections. Therefore, we may have missed patients with soft-tissue infections who had negative cultures because of either early antibiotic administration or inadequate specimens submitted for microbiologic evaluation. Second, our study was performed at a single hospital with demonstrated high rates of health care-associated infections among patients admitted with culture-positive infections [16]. As a result, our findings may not be applicable to hospitals with a lower proportion of patients having health care-associated risk factors at admission. Third, we included patients with device-related soft-tissue infections. This appeared to be an important risk factor for bacteremia and may represent a distinct type of soft-tissue infection similar to catheter-associated bacteremia. The lack of a separate classification for device-related soft-tissue infections is a limitation that needs to be addressed, especially because this type of infection accounted for more than 25% of our population. Fourth, we did not employ a severity of illness score. It is possible that patients dying with bacteremia may have been sicker than non-bacteremic patients. The results of our multivariable analysis refute this idea, however, in showing that a marker of greater disease severity (requirement for intensive care unit admission) was independently associated with death along with bacteremia complicating soft-tissue infections. Lastly, because of the retrospective nature of our study, we may have missed identifying other important factors associated with bacteremia and in-hospital death.
In summary, we found that bacteremia complicating soft-tissue infections is common and associated with a greater risk of death. Clinicians should consider obtaining blood cultures in patients with soft-tissue infections who have risk factors predisposing to this complication. The identification of pathogens in blood cultures offers prognostic information and may help in directing antimicrobial therapy for patients with soft-tissue infections.
Footnotes
Acknowledgment
Dr. Kollef's efforts were supported by the Barnes-Jewish Hospital Foundation.
Author Disclosure Statement
The authors have no conflicts of interest to report for this manuscript.
Appendix
| Diagnosis code | Description |
|---|---|
| 728.86 | Necrotizing fasciitis |
| 785.4 | Gangrene |
| 686.09 | Ecthyma gangrenosum |
| 730.00-730.2 | Osteomyelitis |
| 630-677 | Complications of pregnancy, childbirth, and puerperium |
| 288.0 | Neutropenia |
| 684 | Impetigo |
| Procedure code | |
| 39.95 | Plasmapheresis |
| 99.71 | Hemoperfusion |