
Abstract
Abstract
Background:
Central venous catheter (CVC)-related infections are a substantial problem in the intensive care unit (ICU). Our infection control team initiated the routine use of antiseptic-coated (chlorhexidine–silver sulfadiazine; Chx-SS) CVCs in our adult ICUs to reduce catheter-associated (CA) and catheter-related (CR) blood stream infection (BSI) as we implemented other educational and best practice standardization strategies. Prior randomized studies documented that the use of Chx-SS catheters reduces microbial colonization of the catheter compared with an uncoated standard (Std) CVC but does not reduce CR-BSI. We therefore implemented the routine use of uncoated Std CVCs in our surgical ICU (SICU) and examined the impact of this change.
Hypothesis:
The use of uncoated Std CVCs does not increase CR-BSI rate in an SICU.
Methods:
Prospective evaluation of universal use of uncoated Std CVCs, implemented November 2007 in the SICU. The incidences of CA-BSI and CR-BSI were compared during November 2006–October 2007 (universal use of Chx-SS CVCs) and November 2007–October 2008 (universal use of Std CVCs) by
Results:
Annual use of CVCs increased significantly in the last six years, from 3,543 (2001) to 5,799 (2006) total days. The APACHE III scores on day 1 increased from a mean of 54.4 in 2004 to 55.6 in 2008 (p = 0.0010; 95% confidence interval [CI] 1.29-5.13). The mean age of the patients was unchanged over this period, ranging from 58.2 to 59.6 years. The Chx-SS catheters were implemented in the SICU in 2002. Data regarding the specific incidence of CR-BSI were collected beginning at the end of 2005, with mandatory catheter tip cultures when CVCs were removed. Little difference was identified in the incidence of BSI between the interval with universal Chx-SS use and that with Std CVC use. (Total BSI 0.7 vs. 0.8 per 1,000 catheter days; CA-BSI 0.5 vs. 0.8 per 1,000 catheter days; CR-BSI 0.2 vs. 0 per 1,000 catheter days.) No difference was seen in the causative pathogens of CA-BSI or CR-BSI.
Conclusion:
Eliminating the universal use of Chx-SS-coated CVCs in an SICU with a low background incidence of CR-BSIs did not result in an increase in the rate of CR-BSIs. This study documents the greater importance of adherence to standardization of the processes of care related to CVC placement than of coated CVC use in the reduction of CR-BSI.
The CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections recommend preventive strategies with strong supportive evidence, including: (1) Education and training of healthcare providers; (2) use of full barrier precautions during CVC insertion; (3) use of a 2% chlorhexidine preparation for skin antisepsis; (4) no routine replacement of CVCs; and (5) use of an antiseptic/antibiotic-impregnated CVC in adults whose catheter is expected to remain in place longer than five days if, after implementing a comprehensive strategy to reduce the rate of CR-BSI, the infection rate remains above the goal set by the individual institution on the basis of benchmark rates and local factors. All of these preventive strategies are employed by critical care practitioners in an attempt to achieve zero CR-BSIs in intensive care units (ICUs) [2,10].
Antimicrobial-impregnated (minocycline/rifampin) and antiseptic-coated (chlorhexidine–silver sulfadiazine; Chx-SS) CVCs have been studied extensively. Two meta-analyses of randomized trials have established that antimicrobial/antiseptic-coated CVCs reduce the incidence of microbial colonization and CR-BSI, but the methodologic quality of the studies generally was poor, putting the conclusions in doubt [11]. The minocycline/rifampin CVCs were associated with CR-BSI reduction, but Chx-SS CVCs were not. Furthermore, these studies were not done in settings where infection-prevention bundles of care were established as routine practice. The investigators concluded that coated CVCs may be useful if the incidence of CR-BSI is above institutional goals despite full implementation of infection prevention interventions [12].
However, few studies address the efficacy of antiseptic-coated CVCs in ICUs with low CR-BSI rates. Schuerer et al. evaluated whether the use of Chx-SS CVCs would decrease the CR-BSI rate in a surgical ICU (SICU) with an already low rate. They found no statistically significant decrease in CR-BSI rates from before implementation of the Chx-SS CVCs (3.3 per 1,000 catheter days) to after implementation (2.1 per 1,000 catheter days; p = 0.16)[13].
The routine use of Chx-SS CVCs was initiated in our SICU as we implemented other educational and standardization strategies to reduce CR-BSI. Once we achieved a low CR-BSI rate, we began using uncoated Std CVCs instead of Chx-SS CVCs and examined the impact of this unit-wide practice change.
Patients and Methods
Setting
The University of Michigan 20-bed SICU admits all non-cardiothoracic critically ill surgical patients. The SICU operates as a collaborative model in which a dedicated unit team works closely with the admitting surgical team to facilitate communication and coordinate all aspects of care. To minimize duplication and optimize efficiency, only the SICU team enters orders. Physician staffing includes an attending surgical or anesthesiology intensivist and an in-house resident team that consists of a surgical or anesthesiology critical care fellow and resident staff assigned exclusively to the SICU.
Patients
All patients admitted to the SICU were evaluated for BSIs. Only patients identified as having a BSI who underwent placement of a CVC by the SICU team in the internal jugular, subclavian, or femoral position were included in the analysis.
Design
We used an interrupted time-series (quasi-experimental) design to examine the outcomes of interest. In 2000, our infection control team initiated the routine use of antiseptic-coated triple-lumen CVCs (Chx-SS, first generation with external coating [ARROWguard Blue®], transitioned to second-generation coated internally and externally [ARROWguard Blue PLUS ®; Arrow International, Inc, Reading PA]) in our adult ICUs as we implemented other educational and standardization strategies aimed at CR-BSI reduction (hand hygiene and antisepsis, dedicated catheter cart use, standardized placement, chlorhexidine skin preparation, maximum sterile barriers) (Fig. 1). Placement, use, and care for CVCs were standardized by hospital policy (see below). Empowerment of any member of the patient care team to stop line placement in the event of contamination or failure of protocol adherence was enforced. Education and twice-daily evaluation of CVC removal was performed during SICU team rounds starting in 2005.
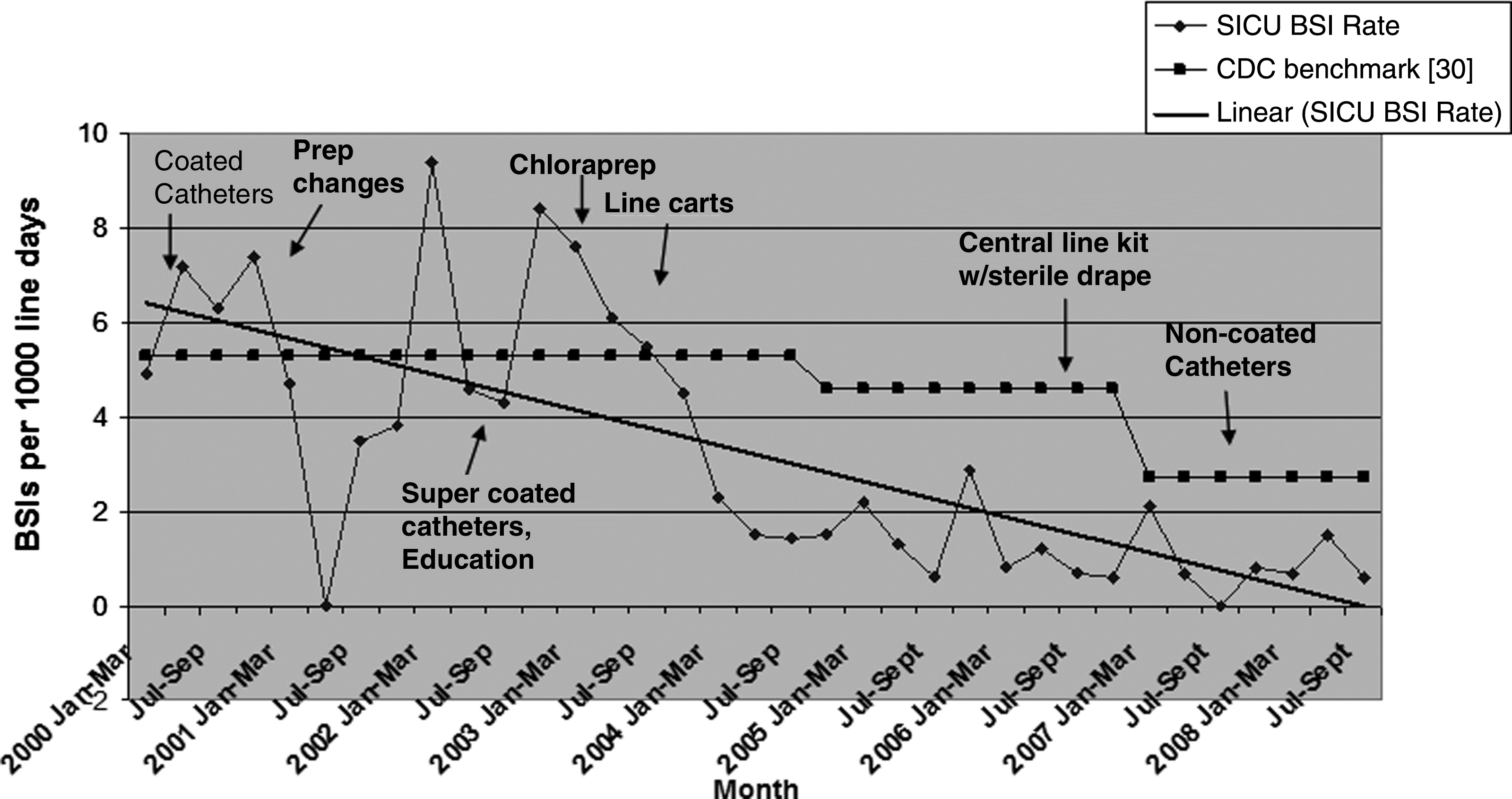
Surgical intensive care unit blood-stream infection rate, 2000–2008.
The rate of catheter-associated (CA)-BSI decreased steadily until 2006, during which our rate was 0.9 per 1,000 CVC days and the rate of CR-BSI was 0 per 1,000 CVC days. In November 2007, the SICU team implemented use of standard non-coated triple-lumen CVCs (same manufacturer) and tracked our CA-BSI and CR-BSI rates over the following year. All preventive efforts previously implemented regarding CA-BSI prevention were continued. Although we did not track compliance with hospital infection control policies, staff education and routine monitoring of hand washing were continued throughout the study period.
Standardization of CVC placement and care
Placement and maintenance of CVCs is standardized by the University Hospitals and Health Centers Infection Control Committee Policy: VI-58 Central Lines: Temporary Central and Arterial Vascular Access Catheters, Long-Term Central Catheters: Tunneled and Ports, and Peripherally Placed Central Catheters (PICC) [14]. The hospital policy for Use and Maintenance of CVC Catheters was followed, which includes washing hands before and after replacing, accessing, or repairing the catheter, and before and after palpating or dressing the catheter site; and use of clean gloves to remove old dressings and either clean or sterile gloves when placing a fresh, sterile dressing; or using an aseptic “no-touch” technique to apply a sterile dressing to the catheter site. The insertion site is evaluated every 24 h, with every dressing change, and when the patient complains of discomfort at the site. The catheter site was cleansed during dressing changes with a 2% chlorhexidine–70% isopropyl alcohol-based preparation (70% isopropyl alcohol or iodophor solution if there was a patient allergy). Catheter sites were kept clean with a sterile, dry, gauze dressing taped in a manner to resist moisture; alternatively, a highly permeable transparent dressing was employed.
Dressing changes also are regulated by hospital policy. Gauze dressings or any dressing constructed with gauze or other opaque materials were changed at least every three days or whenever they become wet, loose, or soiled or when inspection of the site was necessary. Highly permeable transparent dressings were changed at least every seven days and as necessary.
Catheter manipulations were kept to a minimum; when necessary, they were performed using strict aseptic technique. A needleless access system with a pierced injection port and blunt cannula or locking blunt cannula was used to maintain a closed system. Access ports were changed every seven days. A Luer-lok-type attachment was used for extension tubing. All stopcocks were fitted with a pierced injection needleless port at the time of set-up. Access points were disinfected with alcohol just before entry. Blood draws through the CVCs were kept to a minimum; when required, blood specimens were obtained using aseptic technique and clean gloves and the tubing, stopcock, IV port, and the access port attached to the stopcock was flushed clean of any remaining blood after the specimen was removed. The use of stopcocks was kept to a minimum, and a fresh, sterile cap was used after each entry. Stopcocks were flushed clean after blood drawing.
The SICU also adheres to University policies for changing the intravenous tubing and attached components (secondary tubing, extension tubing, stopcocks, locking blunt cannulae, pierced injection ports/caps used on stopcocks, T-connectors). These were changed according to the following guidelines: Tubing for fluids, medications, hemodynamic pressure monitoring, and parenteral nutrition without lipids was changed every 96 h; tubing for lipids and continuous blood products was changed at least every 24 h; and tubing and components used for propofol administration were changed at least every 12 h.
The SICU policy is not to remove or replace CVCs inserted outside the unit routinely if they were placed with aseptic technique. If CVCs are placed in an emergency situation or under non-sterile conditions, they are removed immediately. It is our policy never to replace CVCs over a guidewire unless it is impossible to place a new CVC elsewhere. The internal jugular site is preferred for CVC placement in the SICU, with real-time ultrasound guidance to avoid technical complications and to avoid subclavian vein stenosis in patients with advanced renal disease.
Data collection
Differentiation between CA-BSI and CR-BSI was first made in 2005, mandating catheter tip cultures and peripheral blood cultures in all SICU patients when CVCs were removed. A CA-BSI was defined as a positive blood culture in a patient with a CVC in place and no other apparent source of infection; i.e., the CVC is assumed to be the cause of the BSI. A CR-BSI was defined as a positive blood culture in a patient with a CVC in place, isolation of the same organism from a semi-quantitative or quantitative culture of a catheter segment and from the blood of a patient with symptoms of BSI, and no other apparent source of infection; i.e., the catheter is confirmed to be the cause of the BSI. Cultures from CVCs were performed by the central microbiology laboratory using the roll plate method, in which the cut end of the CVC catheter is rolled across an agar plate and the numbers of colony-forming units are counted after an incubation period [15]. Blood stream infections were monitored by the University infection control team, and the data were evaluated monthly by the faculty, staff, and administration at the SICU quality assurance meeting.
Statistics
We used an unpaired t-test to compare the Acute Physiology and Chronic Health Evaluation (APACHE) III score, Acute Physiology Score (APS), and age differences in the SCIU from the year before intervention with those of the post-intervention period. A 2 × 2 contingency table was analyzed using the χ2 test with Yates correction to compare total BSI, CA-BSI, and CR-BSI rates from the pre-intervention period with those of the post-intervention period.
Results
Patients
The number of SICU admissions annually ranged from 1,340 to 1,491. The services admitting patients to the SICU included Transplant, Non-Trauma Emergency, Trauma, General Surgery, Surgical Oncology, Urology, Obstetrics/Gynecology, Orthopedics, Otolaryngology, Vascular Surgery, Interventional Radiology, Thoracic Surgery, and Surgical Critical Care. Disease acuity, assessed by the admission APACHE III score [16], increased from 52.5 in the pre-intervention period (historical 58.2 in 2004) to 55.6 in the post-intervention period (p = 0.0010; 95% confidence interval [CI] 1.29-5.13). Similarly, the mean APS [16] increased from 42.3 to 45.3 (p = 0.0009; 95% CI 1.22-4.74) during the same time. The mean patient age remained the same at 57 years. There were no differences in any other demographics or critical care characteristics of the SICU patients during the time periods examined (Table 1).
APACHE = Acute Physiology and Chronic Health Evaluation score; ICU = intensive care unit.
Catheter-associated and catheter-related blood stream infections
The total number of CVC days during the pre-intervention period (November 2006–October 2007) when Chx-SS-coated triple-lumen CVCs were used exclusively was 5,580. The mean number of catheter-days per patient was 5.79 in the pre-intervention period and 5.87 in the post-intervention period. The total number of CA-BSIs was three, a rate of 0.5 per 1,000 catheter-days. The total number of CR-BSIs during the pre-intervention period was one, a CR-BSI rate of 0.2 per 1,000 catheter-days (Table 2).
BSI = blood stream infection; CA = catheter-associated; CR = catheter-related; Chx-SS = chlorhexidine–silver sulfadiazine central venous catheter; N/A = not available; Std = standard catheter.
Rate = central venous catheter infections per 1,000 catheter-days.
The total number of CVC days during the post-intervention period (November 2007–October 2008) when Std non-coated triple-lumen CVCs were in use was 5,244. The total number of CA-BSIs was four, a rate of 0.8 per 1,000 catheter-days. The total number of CR-BSIs during the time period was zero (Tables 2 and 3).
CA = catheter-associated; CR = catheter- related; BSI = blood stream infection; CVC = central venous line; VSE = vancomycin-sensitive Enterococcus; VRE = vancomycin-resistant Enterococcus.
Causative pathogens
No difference in the causative microbial pathogens for CA-BSI or CR-BSI was noted between the pre-intervention and post-intervention periods (Table 3). Note that most of these CA-BSIs were not confirmed as CR-BSIs, and the microbial pathogens identified probably were not the causative pathogens in the CR infections.
Relation of catheter location to infection
Catheter-associated BSIs were commonly identified in CVCs positioned in the internal jugular or femoral vein (Table 3). Subclavian CVC placement is not often performed in our SICU because the use of real-time ultrasound guidance is employed regularly for safety concerns.
Discussion
It has been estimated that CVCs account for approximately 90% of all blood stream infections [17,18], and more than five million CVCs are inserted per year in the U.S. [19,20]. Antimicrobial/antiseptic-coated and -impregnated catheters have been designed in an attempt to reduce CR-BSI. Multiple meta-analyses have concluded that coated CVCs are associated with reduction in the rates of BSI, but these studies were performed in the era when CR-BSI rates were high [20–24].
A number of studies have documented that implementation of an education program and standardization of CVC placement in addition to full application of the CDC guidelines for prevention of CA-BSI is associated with a significant reduction in CA-BSI, without the use of antimicrobial/antiseptic-coated CVCs [25–27]. An important single-institution study documented that the “recipe” for zero CR-BSI included: (1) Standardized education of staff; (2) standardized placement of CVC; (3) having a CVC cart with all necessary supplies; (4) daily inquiry regarding discontinuation of CVC; (5) catheter-insertion checklist for assurance of aseptic technique; and (6) empowering the team to halt the procedure if aseptic technique rules are violated [28]. A similar intervention was implemented state-wide in Michigan (108 ICUs; 375,757 catheter days) without the use of antimicrobial/antiseptic-coated CVCs, and a significant reduction in mean CA-BSI, from 7.7 to 1.4/1,000 catheter-days, was documented, representing an overall 66% reduction [29].
After years of an aggressive education program, implementation of the CDC guidelines, and use of Chx-SS-coated CVCs, we reduced the incidence of CA-BSI in the SICU to very low rates. We next examined whether Chx-SS CVCs were an essential component of our CR-BSI infection prevention efforts. By replacing the Chx-SS CVCs with non-coated Std CVCs, we introduced a single change in our CR-BSI infection prevention efforts that did not result in an increase in either CA-BSI or CR-BSI. Our findings are similar to those of Schuerer et al., who demonstrated that use of Chx-SS-coated catheters in a SICU with an already low CA-BSI rate failed to reduce the rate further [13].
We continue to use uncoated Std CVCs exclusively in the SICU. Importantly, neither the CA-BSI nor the CR-BSI rate in the SICU changed substantially over the following five months (CA-BSI total one [0.5 per 1,000 catheter-days]; CR-BSI total zero.)
Catheter-associated BSI has been proposed to be and is accepted as a “never” event; however, this is difficult to achieve. Despite maximum multidisciplinary efforts to reduce CA-BSI in a single ICU as a controlled environment, a persistent zero rate of CA-BSI was not achievable.
The interrupted time-series (quasi-experimental) design used to examine the impact of this intervention (use of uncoated Std CVCs) in the SICU does have several limitations. Most notably, it was conducted in a single SICU in a single tertiary-care institution with all the inherent biases, and is potentially subject to influence by changes in patient populations, ICU practices and policies, and other unrecognized temporal biases. We did not collect data on the CVCs that were not associated with BSI and therefore cannot make any comments on the location, indwelling time, or specific patient characteristics associated with CVCs not linked to BSI. Additionally, in the SICU, CVCs are likely to be placed in a specific subset of critically ill patients. The types of patients and the reason for CVC placement were not tracked during this study.
Despite these limitations, the findings of this analysis support the conclusion that aggressive education programs and adherence to best-practice guidelines are powerful tools in the prevention of CA-BSI and CR-BSI. In ICUs where exceptionally low CA-BSI rates already have been achieved, the universal use of Chx-SS-coated catheters does not yield any additional reduction. Given the cost of $50.00 to $100.00 more for a Chx-SS than an Std catheter, use of Std CVCs in ICUs with a low CR-BSI rate carries potential cost savings.
Conclusion
Elimination of the universal use of Chx-SS-coated CVCs in an SICU with a low number of CR-BSIs did not increase the rate of such infections. This study documents the greater importance of adherence to standardization of the processes of care related to CVC placement and care than of catheter design in reducing CR-BSI.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.