
Abstract
Abstract
Background:
With high morbidity and potentially devastating consequences, surgical site infections (SSIs) after cardiac surgery add substantially to the healthcare burden. Inhibiting migration of skin microbes is likely to reduce contamination of the surgical incision by endogenous potential pathogens. We studied the effect of treatment with a cyanoacrylate-based antimicrobial skin sealant (INTEGUSEAL®) on the SSI rate in cardiac surgery patients.
Methods:
In a consecutive series of 910 prospective patients undergoing routine cardiac surgery, standard pre-operative preparation was performed on 721 patients of whom 189 also received antimicrobial skin sealant. A further 189 consecutive patients who received only standard pre-operative care were studied retrospectively. The primary study endpoint was occurrence of superficial or deep SSI according to the definitions of the U.S. Centers for Disease Control and Prevention.
Results:
The mean (standard deviation) SSI risk score based on combined pre-operative and intra-operative factors according to the Society of Thoracic Surgeons risk scoring system was significantly higher for the skin sealant group (9.1±1.0) than for the prospective (7.1±3.2; p<0.001) and retrospective (8.7±0.8; p<0.001) control groups. Surgical site infections occurred in two patients (1.1%) in the sealant group, 33 patients (4.6%) in the prospective control group (p<0.025), and nine patients (4.8%) in the retrospective control group (p<0.032).
Conclusions:
When added to existing pre-operative measures to reduce bacterial contamination of surgical incisions that are employed routinely at this cardiovascular surgery unit, use of antimicrobial skin sealant decreased the incidence of SSI in cardiac surgery patients.
Tactics to limit the rate of SSI in cardiac surgery have addressed modifiable risk factors and incorporated preventive procedures, including minimizing bacterial contamination of the surgical site, administering adequate antibiotic prophylaxis, minimizing local injury during surgery, and optimizing host defenses [11]. However, no evidence-based standard of care has been recognized. Effective patient skin preparation before surgery is essential, and scrubbing of the operative site with a chlorhexidine or iodophor alcohol-based solution is standard procedure. Although this action reduces the skin flora bacterial counts by approximately 80%, some organisms persist after scrubbing, buried deep in hair follicles and sweat glands [12]. Thus, even with optimal skin preparation, complete disinfection of the skin is not possible [13].
Antimicrobial skin sealant is an emerging technology that, when incorporated into pre-operative preparative procedures, has the potential to reduce the rates of SSI. The sealant polymerizes on application to the skin to form a continuous but breathable barrier that prevents migration of skin flora into the incision. Importantly, and in contrast to conventional skin disinfection, the polymerized compound seals micro-abrasions on the skin, thus preventing recolonization of such spaces with potential pathogens. This paper reports the effect of treatment with a cyanoacrylate-based antimicrobial skin sealant (INTEGUSEAL Microbial Sealant, Kimberly-Clark Corporation, Dallas, TX) on the incidence of SSI in patients undergoing routine cardiac surgery.
Patients and Methods
This study included consecutive patients undergoing routine cardiac surgery at the Department of Cardiovascular Surgery, Charité Hospital, Berlin, Germany, between March and November 2007. During this period, 910 patients were studied prospectively. Standard institutional pre-operative preparation was performed in 721 patients by one of five academic staff surgeons. In addition, 189 patients undergoing surgery by a single academic staff surgeon (P.M.D.) received antimicrobial skin sealant. A further 189 patients who received standard care before surgery by P.M.D. between March 2006 and February 2007 are included for separate retrospective comparison.
Standard Pre-Operative Preparation
For patients scheduled for elective or urgent surgery, hair removal was performed by a clipper or depilatory cream on the afternoon of the day before surgery. Depilatory creams were used in patients who were completely stable and a clipper for patients assessed as unstable. Patients then washed by shower using only soap and showered again on the morning of surgery. For patients undergoing emergency surgery, hair was removed by clipper immediately prior to surgery, and patients did not shower. After hair removal, the skin was disinfected using povidone–iodine alcohol-based solution or, in patients intolerant of povidone–iodine, chlorhexidine alcohol-based solution. The disinfecting solutions were allowed to dry completely before iodine-impregnated drapes were applied (except for those with iodine intolerance), and, for patients in the study group, antimicrobial skin sealant was administered (see below).
Antimicrobial Skin Sealant Application
The antimicrobial sealant was applied to the skin after completion of pre-operative preparation and 5–10 min before surgery commenced. The INTEGUSEAL IS100 applicator was used to apply a single even layer of sealant over an area of approximately 50×25 cm around the sternal incision mark and was allowed to dry completely before any drapes were positioned. Skin sealant was applied only to the sternal site.
Intra-Operative Care
All patients underwent normothermic cardiopulmonary bypass, and care was taken to maintain optimal temperature during surgery. Blood glucose concentrations were monitored regularly, and all patients, with or without diabetes mellitus by history, who became hyperglycemic during or after surgery received insulin intravenously as a single dose, intermittent doses, or by continuous infusion until blood glucose concentrations had been normalized. Patients with type 2 diabetes mellitus with blood glucose ≥6.7 mmol/L (120.6 mg/dL) received insulin intermittently, but if the blood glucose concentration had not normalized by the next measurement, these patients were given insulin by continuous infusion. Arterial pO2 was maintained at 120–150 mm Hg with supplemental oxygenation throughout the operative period. Antibiotic prophylaxis was given 60 min before skin incision, with a second dose 4 h later and a third dose 6 h after the second dose.
Microbiological Methods
All patients were screened on admission for methicillin-resistant S. aureus (MRSA) with swabs taken from nose, throat, and groin. For MRSA-positive patients with stable angina, surgery was delayed while patients received intranasal mupirocin therapy, daily showers with chlorhexidine solution 4%, and, for those with MRSA-positive throat swabs, topical application of chlorhexidine 0.2% for three days. For patients with SSI, microbiological samples were taken from the incision and cultured. In cases with clinical suspicion of deep incisional SSI, blood cultures were obtained also. Bacterial isolates from wound samples were cultured and identified using standard microbiological procedures.
Study Endpoint and Analyses
The primary study endpoint was the occurrence of superficial or deep incisional SSI within 30 days of followup or within one year if an implant was left during the procedure [14]. The 30-day followup was performed by the medical staff of the rehabilitation clinic. A report on all patients was sent to our hospital. Furthermore, because of our quality management protocol, all our patients were contacted after 30 postoperative days. For the one-year followup, patients having artificial valves were receiving echocardiographic followup and were seen again. All other eventual events were documented by the general medical staff and communicated to us.
Deep incisional SSI was defined as infection of the surgical site that was treated with vacuum-assisted closure (VAC) before discharge or readmission for deep infection within 30 days of surgery (or within one year if the patient received an implant). Superficial incisional SSI was defined as superficial infection treated with or without VAC therapy with a closed sternum before discharge or readmission within 30 days of surgery (or within one year if the patient received an implant) for superficial site infection. The infection control program at Charité Hospital includes a prospective active epidemiologic surveillance system that participates in the German Nosocomial Infection Surveillance System (Krankenhaus Infektions Surveillance System; KISS). All nosocomial infections are registered, and all complications during followup are recorded. Infection was documented by at least one of the following: (1) Surgical opening of the sternal wound with excision of tissue (incision and drainage) and application of VAC therapy; (2) positive bacterial culture(s); or (3) treatment with antibiotics.
Treatment groups were compared after evaluating pre-operative and combined pre-operative–intra-operative risk scores according to the Society of Thoracic Surgeons system [15]. A higher risk score predicts a greater likelihood of SSI. Preoperative risk factors were age, gender, obesity, diabetes mellitus, arterial hypertension, hyperlipidemia, chronic obstructive pulmonary disease, chronic kidney disease, peripheral vessel disease, carotid artery disease, cerebrovascular accident, poor left ventricular ejection fraction (LVEF), congestive heart failure, acute myocardial infarct within one month pre-operatively, previous bypass surgery, and previous valve surgery. The intra-operative risk factors were the number of anastomoses, use of internal mammary arteries, use of bilateral internal mammary arteries, duration of perfusion, surgical priority (emergency, urgent, or elective), concomitant procedures, and insertion of an intra-aortic balloon pump. Surgery was defined as urgent if carried out within 24 h of admission and emergency if undertaken within 6 h of admission.
Data were analyzed using SPSS software (version 13.0; SPSS, Inc., Chicago, IL). Categorical variables were analyzed using chi-square testing. Continuous variables were analyzed with Student's t-test. A p value<0.05 on two-tailed testing was considered significant.
Results
The characteristics of the patients receiving antimicrobial skin sealant (n=189), prospective controls (n=721), and retrospective controls (n=189) are shown in Table 1. The three groups had similar majorities of male patients, but the prospective control group was, on average, older than the skin sealant group. Many patients were hypertensive, and there was a high prevalence of hyperlipidemia. Diabetes mellitus, coronary and peripheral arterial disease, and other co-morbidities were typical of this overall surgical population. Approximately 60% of the patients were undergoing coronary artery bypass graft (CABG) surgery. The mean LVEF values were approximately 50%, 23–54% of patients had had a myocardial infarction, and 10–24% of patients had congestive heart failure (Table 2)
Data are n (%) unless otherwise indicated.
CABG=coronary artery bypass graft; LVEF=left ventricular ejection fraction; SD=standard deviation.
Data are n (%) unless otherwise indicated.
CABG=coronary artery bypass graft; SD=standard deviation.
Sealant vs. prospective controls
In both groups, the majority of patients—70% of the sealant group and 79% of the control group—underwent elective surgery. Other procedures were emergencies (26% vs. 17%; p=0.006) or urgent (5% vs. 4%). Overall, the characteristics of the two patient groups were similar, although there was a significantly lower proportion of patients with hyperlipidemia or hypertension in the control group. The presence of coronary artery disease, a previous cerebrovascular accident, congestive heart failure, myocardial infarction, previous CABG, and previous cardiac valve replacement were significantly more common in the skin sealant group than in the prospective control group (see Table 1).
Preoperative risk scores for SSI were 10.0±1.5 for the skin sealant group and 8.0±3.8 (p<0.001) for the control group. Risk scores for SSI according to combined pre-operative–intra-operative factors were 9.1±1.0 and 7.1±3.2 (p<0.001) for the group having the antimicrobial skin sealant and the control group, respectively. The rates of SSI predicted by these risk scores were 3.1% (pre-operative) and 2.8% (combined) with skin sealant and 2.4% (pre-operative) and 2.1% (combined) for controls. At the clinical endpoint, SSI was recorded in two patients in the sealant group compared with 33 patients in the control group (p<0.025) (Fig. 1), a 76.1% relative risk reduction in the sealant group compared with the control subjects (1.1% vs. 4.6%). Followup for both patient groups was 100%. In one patient in the skin sealant group, MRSA was isolated from the sternal wound three weeks after surgery and also from blood samples. Vancomycin-resistant enterococci and extended-spectrum β-lactamase-producing Enterobacteriaceae also were isolated from this patient, who recovered after treatment with an appropriate antibiotic regimen and supportive measures. Methicillin-sensitive S. aureus (MSSA) was isolated from the other patient in the skin sealant group who developed SSI. The predominant organisms isolated from patients with SSI in the control group were S. aureus (MRSA and MSSA), methicillin-sensitive S. epidermidis, and enterococci (Table 3). Seven patients with SSI in the prospective control group died. There were no deaths in the skin sealant group.
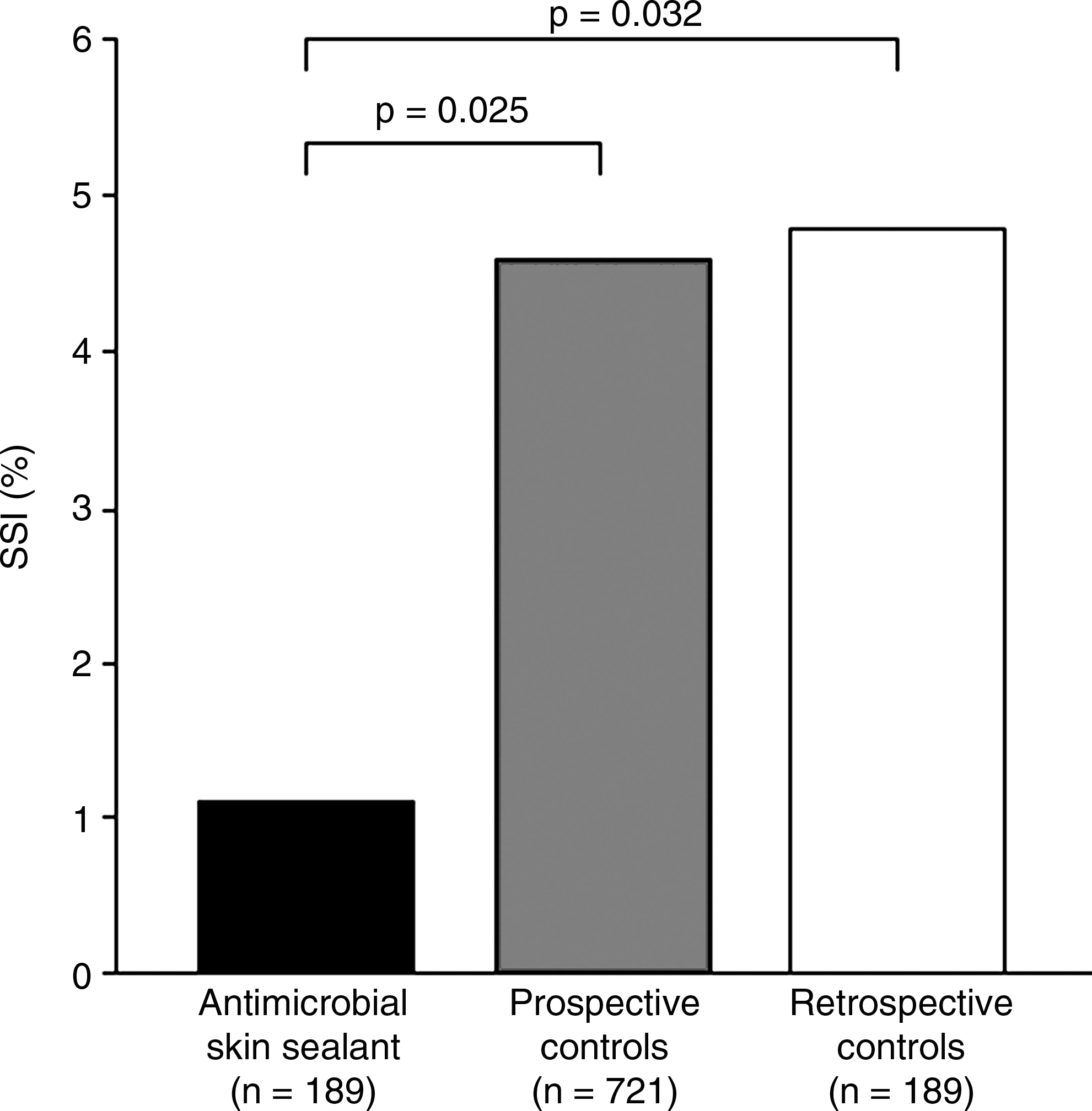
Incidence of surgical site infection (SSI) in patients treated with microbial skin sealant, untreated patients in the same consecutive case series (prospective controls), and untreated patients undergoing surgery by the same surgeon prior to the introduction of sealant to pre-operative preparation (retrospective controls).
MRSA=methicillin-resistant Staphylococcus aureus; MSSA=methicillin-sensitive S. aureus.
Single-surgeon comparison
A retrospective comparison was conducted of SSI in the patients who received antimicrobial skin sealant before surgery (n=189) with 189 preceding consecutive cases who underwent surgery without sealant by the same surgeon (P.M.D.). The rates of coronary artery disease (p<0.015), previous valve replacement (p<0.001)(see Table 1), and bilateral internal mammary artery use (p<0.002) were significantly higher in the skin sealant group.
The pre-operative risk of SSI was 10.0±1.5 and 10.3±1.7 (p=0.070) for the skin sealant group and the retrospective control group, respectively. The combined pre-operative and intra-operative SSI risk score was significantly higher in the skin sealant group than in the control group (9.1±1.0 vs. 8.7±0.8; p<0.001). Predicted rates of SSI based on these risk scores were 3.1% (pre-operative) and 2.8% (combined) with skin sealant and 3.1% (pre-operative) and 2.6% (combined) in the control group. With followup of all cases, the clinical endpoint showed a significant decrease in the rate of SSI in the skin sealant group (n=2) compared with the control group (n=9; p<0.032) (Fig. 1), with a relative risk reduction for the development of SSI of 77.1% associated with the use of skin sealant vs. control subjects (1.1% vs. 4.8%). The predominant organisms isolated from patients with SSI in the retrospective control group were MSSA and methicillin-sensitive S. epidermidis (Table 3). Four patients with SSI in the retrospective control group died.
Discussion
In cardiac surgery patients, infection of the sternal incision site is an infrequent yet potentially disastrous event, leading to prolonged hospitalization, repeated surgical procedures, high associated morbidity and mortality rates, and increased healthcare cost. A substantial number of patient- and procedure-related characteristics have been identified as risk factors for SSI [5,9,15,16]. Risk factor assessment and the implementation of specific surveillance of SSI have increased patient safety. Risk factor models can identify patients who are at high risk for major infection who may then be targeted for peri-operative intervention strategies to reduce their risk [15]. Efficient antibiotic pre-operative coverage, rigorous asepsis, refinements of surgical technique such as the introduction of minimally invasive techniques for vein harvesting, better pre-operative preparation of the patient, and optimum post-operative wound care have contributed to the reduction in SSI rates [17]. Despite improvements in many aspects of peri-operative care, however, SSI after cardiothoracic surgery remains an important if mainly preventable complication.
The results of this study show that the use of an antimicrobial skin sealant prior to surgery significantly reduced the rate of SSI among cardiac surgery patients. The incidence of SSI in patients treated with the skin sealant was lower than that in similar patients undergoing surgery in the same surgical unit and that in similar patients operated on by the same surgeon before the use of skin sealant was introduced into the pre-operative procedures. Notably, the beneficial effect of antimicrobial skin sealant on SSI rates was seen in elderly patients who had a variety of chronic disorders such as hypertension, hyperlipidemia, diabetes mellitus, and vascular disease. These patients had significantly higher mean risk scores for pre-operative and intra-operative characteristics and thus a higher predicted incidence of SSI. The observed rates of SSI in prospective (4.6%) and retrospective (4.8%) controls, although higher than that predicted by risk factor scoring, were similar to those reported by some recent studies [9,18,19] and lower than in other, generally older, studies [2].
Intravenous antibiotic prophylaxis as standard practice has undoubtedly decreased the risk of SSI in cardiac surgical patients, but there is now good evidence that emerging antibiotic resistance is linked directly to the duration of prophylactic antibiotic administration [20]. The clinical consequences of infection with antibiotic-resistant bacteria are serious; patients experience a higher mortality rate, prolonged hospitalization, and increased healthcare costs compared with those infected with nonresistant organisms [20, 21]. The use of broad-spectrum antibiotics for surgical prophylaxis adds to the selective pressure driving the development of resistant pathogens and thus is a clinical dilemma [22]. The continuing problem of SSI dictates that the development and application of novel treatments to extend the multimodal approach to reducing SSI is a consequence of antibiotic stewardship.
Staphylococcus aureus is a major cause of complications of cardiothoracic surgery procedures, accounting for 12%–36.4% of incisional infections overall [4] and is associated with high morbidity and mortality rates and a worse prognosis than infections of other etiologies [23]. In this study, S. aureus was isolated from 20 of the 35 sternal SSIs (57%). The endogenous pathway of infection has been demonstrated for some cases of post-cardiac surgery SSI by an identical pattern of S. aureus from the patient's nose and sternum [4]. Pre-operative eradication of nasal S. aureus may protect against SSI [24], an approach that is supported by cohort studies in cardiac surgery patients that have shown a significant reduction in sternotomy site infections after intranasal mupirocin treatment [25]. In contrast, prophylactic intranasal mupirocin administered to S. aureus carriers did not reduce the rates of SSI overall by S. aureus after cardiac surgery compared with placebo in a randomized clinical trial [26].
In elderly patients with multiple risk factors, the need for urgent or emergency cardiac surgery is common. This limits the opportunity for prophylactic treatments such as intranasal decolonization. Until S. aureus carriers can be identified and decolonized more rapidly, patients who are carriers still need to be treated with intranasal mupirocin for several days to achieve decolonization before surgery. In addition, prolonged or widespread use and repeated courses of mupirocin are associated with the development of mupirocin resistance in S. aureus [27, 28], which compromises its use in other clinical areas. Given the predominant role of skin flora, particularly Staphylococcus spp., in SSI, immobilizing skin-borne microorganisms in situ—a mechanism of action that does not promote bacterial resistance—is a rational approach to the prevention of surgical site contamination by migration of endogenous potential pathogens.
After successful preclinical evaluation [29], early clinical support for the efficacy of microbial skin sealant came from a study of patients undergoing open, clean inguinal hernia repair. Patients having antimicrobial skin sealant after 10% povidone-iodine followed by iodine skin preparation had a significantly lower rate of surgical site contamination than patients treated with povidone–iodine alone (53.0% vs. 68.7%; p=0.04) [30]. Elsewhere, we have reported results from a separate case-control study that showed a significant beneficial effect of antimicrobial skin sealant on the incidence of SSI in patients undergoing CABG surgery [31,32], and a randomized, multicenter clinical trial in CABG patients is underway. Our clinical experience to date indicates that the antimicrobial skin sealant is easy to apply and can be used with a variety of skin preparation solutions and with most site-closure techniques. The treatment has a good safety profile and is now used routinely in our surgical center. Microbial skin sealant may therefore form a valuable part of the multimodal approach to reducing bacterial contamination of surgical incisions, thereby decreasing the risk of SSI.
Reduction of SSI risk also has an important economic impact. Fry [33] reported that the costs of SSI are in general 0.5% of the annual hospital budget. These direct hospital costs of SSI, as reported by Urban [34], are a result of prolonged hospitalization, additional surgical therapy, long-term antibiotic therapy, and additional medical equipment use. The main increase in the cost is a result of the lengthening of the hospital stay, which depends on the severity of the underlying SSI. Coskun et al. [35] showed that superficial incisional SSI costs an average of US$3,740.58, whereas deep incisional SSI costs an average of US$6,850.93. Again, these costs depend on the length of hospitalization, which can be decreased by using aggressive antibiotic therapy. Although the costs of antibiotic therapy will increase as a result, the total costs can be reduced [36,37].
The other side of the economic impact is the indirect costs attributable to loss of productivity if the patient is of working age. Alfonso et al. [38] calculated that for patients younger than 40 years, an SSI-related permanent work incapacity, resulting in years of productivity loss, carried a cost of US$309,636/patient. This study showed for the first time the real cost of SSI in which the healthcare cost together with other costs were only approximately 20% of the total cost, of which the main part was secondary to the years of productive life lost. Therefore, additional prevention of SSI not only has an important impact on surgical morbidity and mortality rates, but also an economic impact for society.
Footnotes
Acknowledgments and Author Disclosure Statement
No financial support was received for this study. Neil McKendrick, Ph.D., provided assistance in preparing and editing the manuscript with financial support from Kimberly-Clark Europe.
P.M.D. has been a member of the speaker faculty for and has received lecture fees from Kimberly-Clark Healthcare. He also has received a research grant from the company for a separate study. D.G., T.G., W.K., J.L., and A.W. have no conflicts.