
Abstract
Abstract
Background:
Peritoneal cavity lavage is used widely in the treatment of peritonitis. Nonetheless, some studies question its rationale and prove it to be deleterious to the mesothelium. The present study aims to determine whether 0.9% and 3.0% saline lavage of the peritoneal cavity have an effect on the early systemic inflammatory response, namely, in the lung injury and splenic cellularity of gerbils with induced peritonitis.
Methods:
Thirty-four male gerbils were divided into four groups: Control (n=9), submitted to laparotomy at time zero, re-laparotomy after 2 h, and sacrificed after a total of 6 h from start; untreated (n=8), submitted to peritonitis induction through cecal ligation and puncture (CLP) at time zero, re-laparotomy intended for drying of abdominal cavity and resection of the ischemic cecum after 2 h, and sacrifice after a total of 6 h from start; saline (n=8), submitted to peritonitis induction through CLP at time zero, re-laparotomy intended for warm 0.9% saline lavage of the abdominal cavity and resection of the ischemic cecum after 2 h, and sacrificed after a total of 6 h from start; and hypertonic (n=9), submitted to peritonitis induction through CLP at time zero, re-laparotomy intended for warm hypertonic saline (3.0%) lavage of the abdominal cavity and resection of the ischemic cecum after 2 h, and sacrificed after a total of 6 h from start. After sacrifice, we collected the left lung and the spleen for morphometric analysis.
Results:
In the both the saline and hypertonic groups, there was significant decrease in the mean nuclei count in the lungs, compared with the untreated group (p<0.01). There was no difference in terms of nuclei count in the spleen among groups (p>0.05).
Conclusions:
The present study demonstrated that the peritoneal lavage with large volumes of warm 0.9% and 3.0% saline has a beneficial effect on the early systemic inflammatory response in infected animals, modulating and reducing the lung injury but having no effect on splenic cell count.
P
Although used commonly, lavage of the peritoneal cavity has no consensus among surgeons. Many variables of the technique are still empirical (such as the methods of performing the lavage, type of fluid and volume used, among the others), and evidence is still scant on the subject, being dependent on the experience of each surgeon.
A questionnaire conducted in England revealed that 97% of surgeons adhere to the practice of washing the peritoneal cavity. It also showed that most of the surgeons perform the lavage until the aspirated fluid is clear, with no signs of contaminates, which usually occurs with 500–1,000 mL [4].
There are many lines of research on this subject, with conflicting results. Some studies propose that the lavage interferes with defense mechanisms, promoting the spread of pathogens in the abdominal cavity, with little or no interference in the prognosis of patients [5]. Others suggest that it modulates the inflammatory response and reduces end-organ damage, improving survival [6].
The intravenous (IV) use of hypertonic saline has been proved beneficial as a part of the treatment of multiple organ dysfunction syndrome due to peritonitis [7]. Shih et al. [7] demonstrated that animals treated with IV hypertonic saline had reduced concentrations of nitric oxide and interleukin-1β in plasma and oxygen free radicals in organs, and it also prevented circulatory collapse, reduced mortality, and organ dysfunction.
The present study aims to determine whether hypertonic saline lavage of the peritoneal cavity has an effect on the early systemic inflammatory response, namely, in the lung injury and splenic cellularity of gerbils with induced peritonitis.
Materials and Methods
This work was approved by the Ethics Committee of Animal Research of the Universidade Federal de Minas Gerais, according to protocol 186/2011.
Subjects and experimental groups
Thirty-four male gerbils, 12 weeks old and weighing 75–90 g, were used in the experiments. The animals were obtained from the Instituto de Ciências Biológicas da Universidade Federal de Minas Gerais and were maintained in collective cages, and provided rodent chow (Labina®, Purina, St. Louis, MO) and water ad libitum prior to the experiments.
The animals were divided into the following four experimental groups:
Control (n=9), subjected to laparotomy at time zero, re-laparotomy after 2 h, and sacrifice after a total of 6 h from start.
Untreated (n=8), subjected to peritonitis induction through cecal ligation and puncture (CLP) at time zero, re-laparotomy intended for drying of abdominal cavity and resection of the ischemic cecum after 2 h, and sacrifice after a total of 6 h from start.
Saline (n=8), subjected to peritonitis induction through CLP at time zero, re-laparotomy intended for warm 0.9% saline lavage of the abdominal cavity and resection of the ischemic cecum after 2 h, and sacrifice after a total of 6 h from start.
Hypertonic (n=9), subjected to peritonitis induction through CLP at time zero, re-laparotomy intended for warm hypertonic saline (3%) lavage of the abdominal cavity and resection of the ischemic cecum after 2 h, and sacrifice after a total of 6 h from start.
Induction of peritonitis
Gerbils were anesthetized with intraperitoneal injection of a solution of xylazine (8 mg/kg) and ketamine (60 mg/kg). The abdominal wall was disinfected with 0.05% chlorhexidine, and a 2-cm midline laparotomy was performed. Peritonitis was induced by CLP, which consisted of the ligation of the antimesenteric surface of the cecum with 5-0 silk and puncture of the excluded cecum with scissors (2 mm extension). The abdominal wall was closed using a 4-0 nylon continuous suture. In the control group, a laparotomy was performed and only the viscera were manipulated, followed by closure of the abdominal wall. Animals had access to water ad libitum right after the procedure.
Peritoneal lavage
After a 2-h observation period, the animals were submitted to re-laparotomy under anesthesia, the ischemic cecum was excised, and the peritoneal cavity was treated according to each group. In the untreated group, the cavity was dried with sterile gauze and closed. In the saline group, the lavage was performed with 10 mL of warm (38°C) 0.9% NaCl solution for three times (5 min for each of the three lavages), followed by drying of the cavity and closure of the abdominal wall. In the hypertonic group, the lavage was carried out with 10 mL of warm (38°C) 3% NaCl solution for three times (5 min for each of the three lavages), followed by drying of the cavity and closure of the abdominal wall. In the control group, the animals were submitted to re-laparotomy, with viscera manipulation and closure of the abdominal wall. All animals received one dose of intramuscular ceftriaxone (30 mg/kg) after this second operation.
Necropsy
At the end of a total of 6-h observation period, the animals were submitted to euthanasia by anesthetic overdose (intraperitoneal 200 mg/kg ketamine +25 mg/kg xylazine), the spleen was obtained through laparotomy, and the left lung was obtained through sternotomy, and both were fixed in 10% buffered formalin.
Morphometric analysis
The spleen and left lung were embedded in paraffin and sections of 4 microns were prepared in slides and stained with hematoxylin and eosin. The morphometric analysis of the pulmonary inflammatory infiltrate was conducted to produce 10 randomly-captured images on each plane (upper, middle, and lower) of the left lung, which was visualized using a 40× objective and digitized using a microcamera (JVC TK-1270/RGB Victor Company of Japan, Ltd., Yokohama, Japan), measuring a total of approximately 1.6×106 square micrometers of the analyzed tissue. On the other hand, the morphometric analysis of splenic cellularity was determined by producing 30 randomly-captured images of the red pulp, following the same mechanism described for the lung.
All cells in each image were quantified using the KS300 software program from the Carl Zeiss Image Analyzer (Jena, Germany). The nucleus of leukocytes and other cell types usually present in lung and splenic tissue were counted through nuclear pixel selection from the real image, and subsequently transformed into a binary image for later analysis. For the final analysis, the images captured on the different planes were grouped to determine the cellular count in each animal's lung. The pathological changes were assessed by a pathologist blinded to the animal groups. The results of total nuclei count were expressed as number of cells ×103.
Statistical analysis
The results were expressed as mean±standard deviation. Statistical analysis was performed using the Mann-Whitney U test, with p<0.05 accepted as statistically significant.
Results
Lung
In the control group, the mean nuclei count in 30 random fields was 8.3±1.6. In the untreated group, the mean nuclei count was 11.7±1.7, with a significant difference when compared with the control group (p<0.001). The saline group had a mean nuclei count of 9.2±1.6, with a significant difference when compared with the untreated group (p<0.005), and no significant difference when compared with the control group (p>0.05).
The hypertonic group had a mean nuclei count of 9.2±1.3, with a significant difference when compared with the untreated group (p<0.003), and no significant difference when compared with the control group (p>0.05; Fig. 1). The hypertonic group, when compared with the saline group, had no significant difference in terms of nuclei count (p>0.05; Fig. 2).
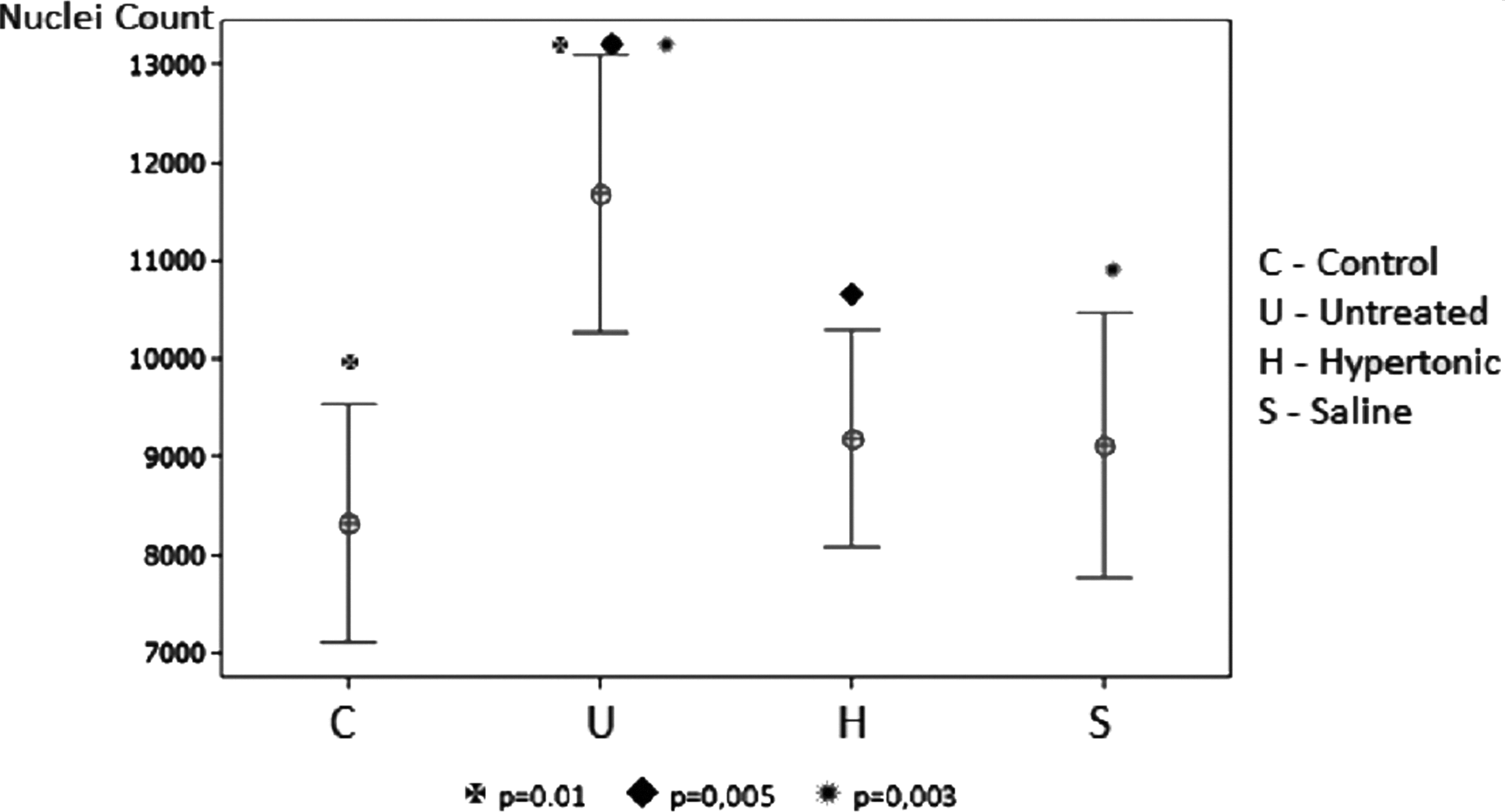
Lung nuclei count expressed as mean±standard deviation.
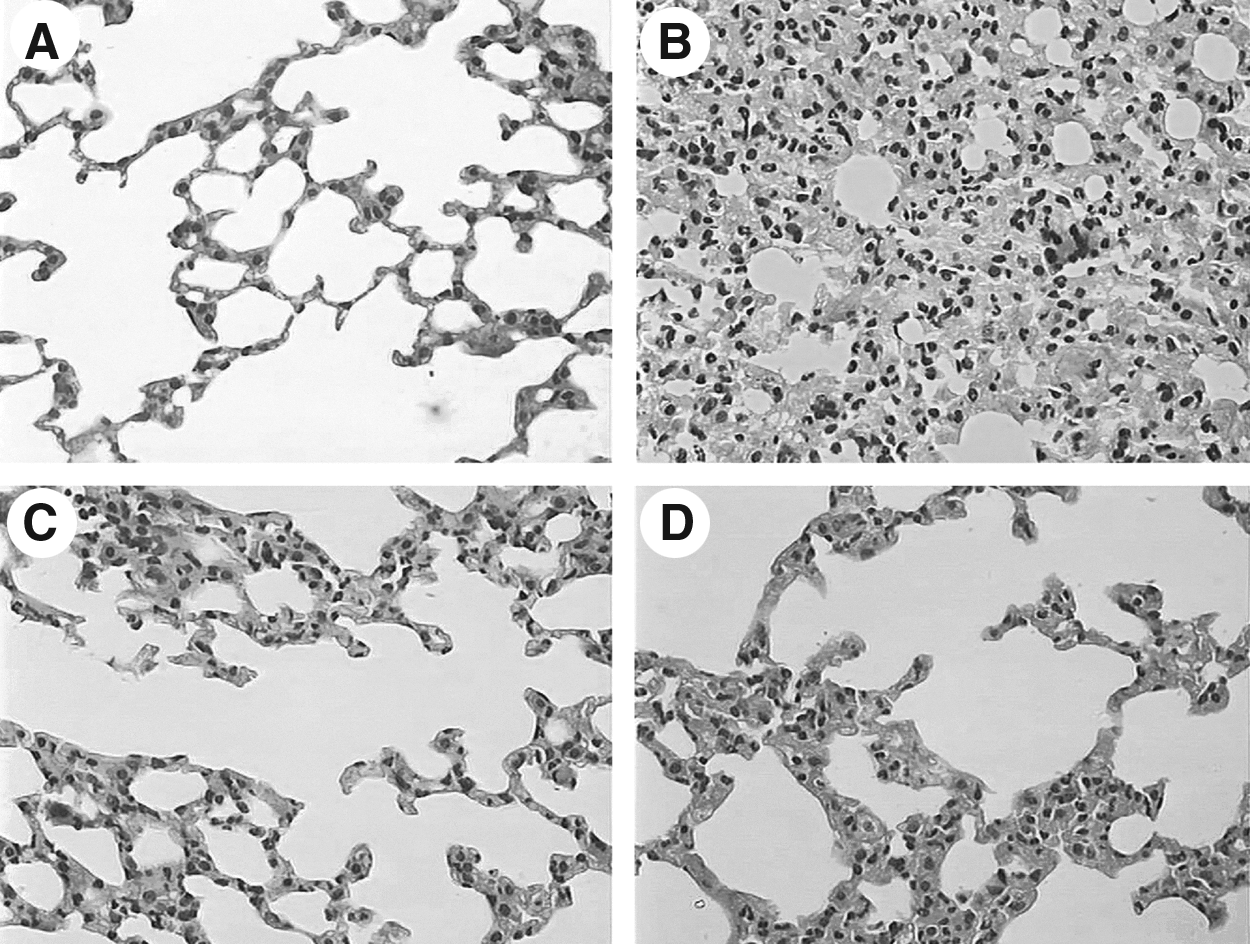
Digitized image of the left lung (40× objective lens).
Spleen
In the control group, the mean nuclei count in 30 random fields was 18±3.7. In the untreated group, the mean nuclei count was 16.6±3.7, with no significant difference when compared with the control group (p>0.05).
The saline group had a mean nuclei count of 17.2±5.1, with no significant difference when compared with the untreated group (p>0.05) and control group (p>0.05).
The hypertonic group had a mean nuclei count of 14.9±3.7, with no significant difference when compared with the untreated group (p>0.05) and control group (p>0.05; Fig. 3).
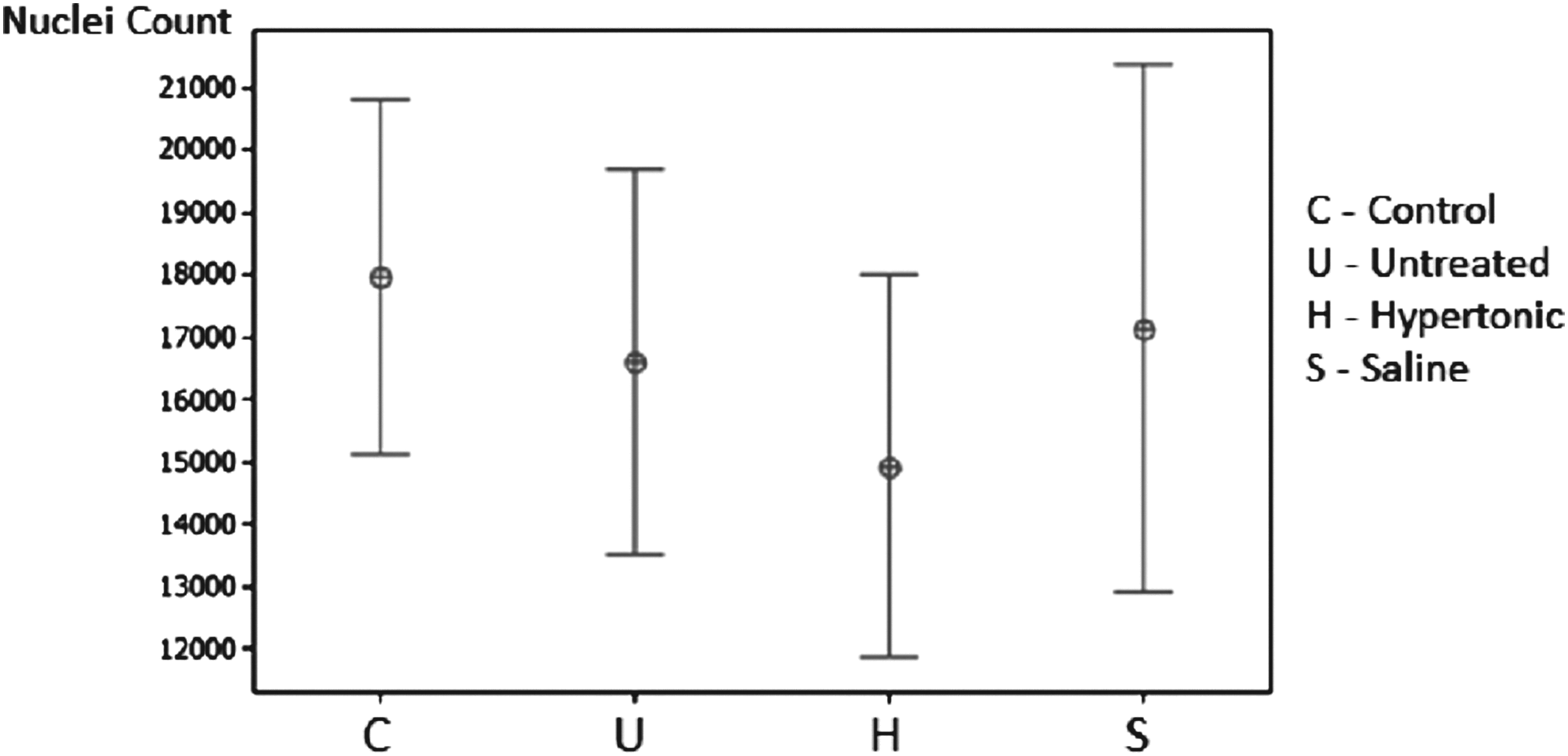
Spleen nuclei count expressed as mean±standard deviation.
Discussion
Secondary bacterial peritonitis and its complications, such as septic shock and multiple organ dysfunction syndrome, are still important causes of death in surgical practice [8]. Its physiopathology not only involves local injury but also end-organ injury (such as the lung), which are associated with greater mortality in abdominal infection. The lungs have been considered as the remote organ most commonly affected (74% of the cases [9]), and is usually the first organ to fail and one of the main causes of death in patients with peritonitis [10]. Inflammatory conditions can cause increased oxidative activity of the lung, resulting in peroxidation of the membrane and secretion of cytokines by activated macrophages, causing a persistent inflow of neutrophils to the lung [11,12].
It has also been proven that pulmonary neutrophil count increases and reaches a plateau at 5 h after inducing peritonitis [10]. Therefore, although such an early intervention during abdominal infection is rarely seen in clinical practice, our observational period suffices to evaluate the early pulmonary inflammatory response.
The precise immunologic role of the spleen in sepsis is still debated. It has been established that splenectomized patients are at higher risk of developing lethal septic shock [13]. Nonetheless, some recent studies have concluded that splenectomy does not worsen survival during polymicrobial abdominal sepsis, but actually reduces liver damage and decreases lethality [13,14]. The mechanism involved in this protection involves the reduction of systemic high mobility group box 1 and maintenance of Th1-dependent serum cytokine response, reducing sepsis-induced liver injury [14]. Santos et al. [15] demonstrated that splenic exudation occurs 48 h after peritonitis induction, due to which we could not detect any change in splenic cellularity in the present study.
Over the past decades, the adjunctive use of peritoneal lavage by surgeons has been widely debated, and clinical studies have not come to a consensus. The first surgical approach to peritonitis was proposed by Mikulicz in 1889 [16]. His concept was that an early operation, with elimination of the focus and lavage of the cavity, could interrupt the vicious circle of inflammation and improve survival. Such concepts are still the basis of the treatment, and Seiler et al. demonstrated that among 258 patients diagnosed with diffuse peritonitis, 88% were treated successfully according to Mikulicz's concepts [17].
It is already clear that washing the peritoneal cavity also has its adverse aspects in the peritoneal defense mechanisms. Haagen et al. [18] and Edmiston et al. [19] found that bacteria adhere to mesothelial cells and the lavage results in only transient reductions of the bacterial populations. Moreover, lavage can remove important inflammatory mediators (i.e., complement proteins, proteases, opsonic proteins, and immunoglobulins), impairing peritoneal defense mechanisms [20]. Washing the cavity can also retard the healing process of the compromised mesothelial cells and cause even more injury to the mesothelial cell membranes [3,21].
Nonetheless, most studies have proved that lavage of the peritoneal cavity can reduce bacterial load, inhibit bacterial proliferation, and is better than no treatment [2,20,22]. Our study confirmed that washing the peritoneal cavity with 0.9% or 3.0% NaCl solutions is better than systemic antibiotics alone in the treatment of peritonitis.
So far, there is neither a consensus on the best technique of peritoneal lavage nor on the best solution to be employed. A recent meta-analysis favored the use of antibiotic in the lavage solution [2]. Other studies found no appreciable advantage in using them as long as systemic antibiotics are being used [23]. Solutions with antiseptics (such as povidone-iodine or chlorhexidine) and altered pH demonstrated controversial effects among different studies [1,3]. Local anesthetics (i.e., lidocaine) seem to improve the survival when used in the lavage solution [24]. It has been suggested that large volumes of solution are more efficacious [25], a principle that was assured in this study.
The use of IV 7.5% hypertonic saline has already been studied in the treatment of systemic inflammatory response syndrome (SIRS) and adult respiratory distress syndrome (ARDS) due to various causes (pancreatitis, ischemia-reperfusion, hemorrhagic shock, fat embolism, peritonitis) [7,26–29]. Its use is safe and apparently helps to modulate the systemic inflammatory response by restoring the circulating volume and exerting favorable effect on cardiac contractility, blood pressure, and peripheral tissue perfusion [26]. In our experiment, we hypothesized if local treatment with hypertonic (3.0%) saline could have an immunomodulatory effect in the peritoneum, therefore decreasing the systemic inflammatory response and end-organ damage caused by peritonitis. We were not able to prove any additional benefits from the intraperitoneal use of 3.0% NaCl in contrast to the 0.9% NaCl, which probably indicates that the local effect of the hypertonic solution is merely of mechanical removal of contaminants and endotoxin clearance. We opted for a 3.0% concentration instead of 7.5% described in the literature because the latter is used systemically and we used the former locally. Considering the fact that the solution was used exclusively in the abdominal cavity and that the greater omentum presents a high permeability, the use of a high osmolarity solution would be responsible for a great amount of liquid extravasation into the peritoneal cavity, enhancing the hypovolemia, fact that explains the early death of all the animals in which a 7.5% solution was used in the pilot experiment.
This study has some limitations. Animals did not receive intravenous fluid for resuscitation of abdominal sepsis, and we did not obtain data regarding whether the animals were in septic shock or a hypoperfused state, (i.e., no lactate or base deficit was obtained). Nonetheless, it is important to notice that we aimed to analyze the early effects of peritonitis, therefore, we did not expect relevant hemodynamic and metabolic disturbances in these animals, reason why we opted not to resuscitate in order to annul the effects of volemic resuscitation. It has been proved that fluid is not absorbed from the abdominal cavity with an inflamed peritoneum [30]. Hence, in the experimental groups that had their cavity washed there was no fluid resuscitation consequent to the lavage itself. The lungs and spleen were examined, but other organs (i.e., liver and the kidneys) that are also prone to end-organ damage in sepsis and septic shock states were not examined in this study. Also, no data regarding peritoneal bacteriology were obtained. These data would provide important information regarding the local effect of the peri-operative peritoneal lavage strategies. Also important to notice is that in clinical practice, it is rare to treat patients in such an early phase of sepsis. The short duration of the study is a substantial study limitation and additional studies will be required to investigate the late inflammatory response in this experimental abdominal sepsis model.
Conclusions
The present study demonstrated that the peritoneal lavage with large volumes of warm 0.9% NaCl has a beneficial effect on the early systemic inflammatory response in animals with peritonitis, modulating and reducing the lung injury, which is in accordance with the medical literature [6]. Moreover, it revealed that washing the cavity with large volumes of warm hypertonic (3%) saline is also beneficial and reduces the early pulmonary inflammatory response. Both saline and hypertonic groups presented no difference in terms of lung leukocyte infiltration, when compared with the control group, indicating that lavage was not only able to block progression of the inflammatory response, but also to reverse the process. We could not prove any difference between the 3% and 0.9% NaCl groups.
Footnotes
Author Disclosure Statement
No competing financial interests exist.