
Abstract

G
A 75-year-old farmer presented to our emergency department with a history of painful swelling in the right upper limb following impalement by an animal horn 4 d prior. On examination, the patient had an altered sensorium and was unable to move his right forearm. His edematous right forearm revealed a 4×2 cm ulcer in the posteromedial aspect near the elbow and crepitus on palpation. Neither the radial nor ulnar pulses were palpable and the brachial pulse was feeble. Radiography showed gas in the subcutaneous tissue and in the muscular planes (Fig. 1). The patient underwent an emergency fasciotomy to manage compartment syndrome, and a gram stain revealed gram-positive bacilli with subterminal spores (Fig. 2). The patient was given tetanus immune globulin 250 IU and tetanus toxoid 0.5 intramuscular stat, and started on intravenous (IV) penicillin G and clindamycin mL. The next day, infection had ascended to compartments of the arm. The patient underwent an emergency guillotine above-elbow amputation to control spreading infection. Anaerobic culture showed growth of C. perfringens sensitive to cloxacillin, ceftriaxone, and meropenem. Escherichia coli and Proteus mirabilis were also isolated. Blood culture was sterile. Patient received 5 d of IV antibiotics followed by oral cloxacillin 500 mg for 7 d. Post-operatively, the patient improved and the wound healed (Fig. 4). The patient was discharged after a 14-d hospital stay.
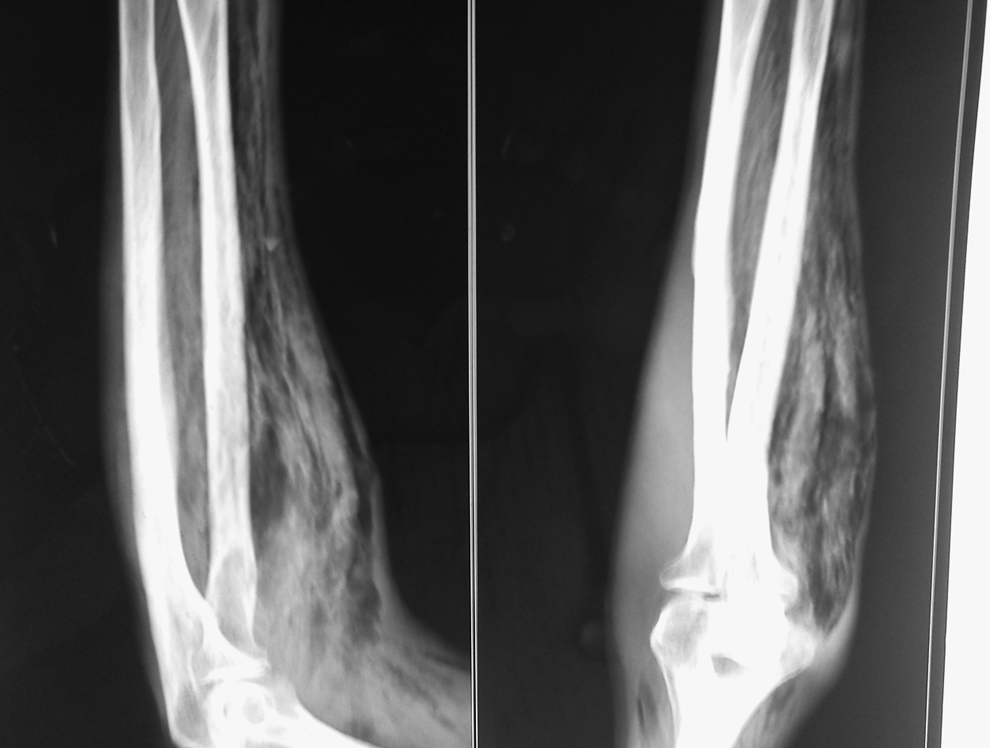
Radiograph of the forearm.
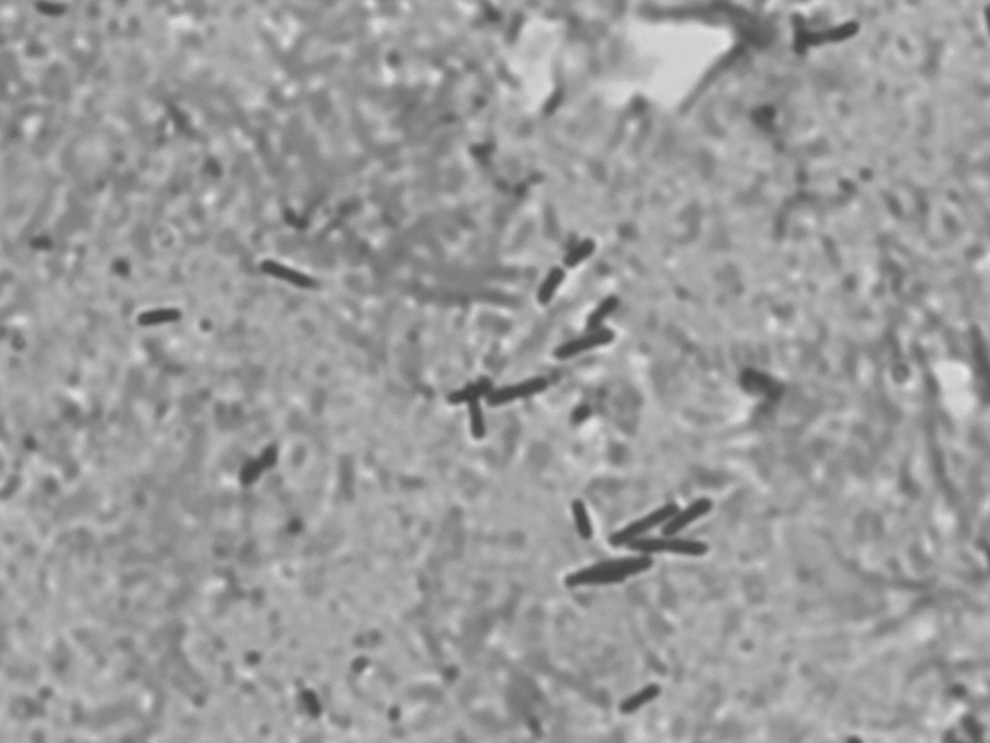
Gram-positive bacilli with subterminal spores.
Gas gangrene of the limbs is rare. Usually, amputation is necessary to control infection and preserve life, whereas functional limb preservation is rare [1]. Incubation time is brief, usually less than 24 h, and the physical finding of crepitus is characteristic but a relatively late finding in the setting of soft tissue infection [4,5]. Plain radiographs identify gas in deep tissues. Bacteremia occurs in approximately 15% of patients and typically develops several hours before skin manifestations [1]. Despite heroic efforts, amputation may be necessary; a salvaged limb may be chronically painful or functionless. The worst case scenario occurs when a limb must be amputated after the patient has endured multiple attempts at salvage or after years of pain following a “successful” salvage. On the other hand, early amputation and prosthetic fitting is associated with decreased morbidity, fewer operations, a shorter hospital course, decreased hospital cost, and shorter duration of rehabilitation in cases of traumatic limb injury [3].
The subjective importance of body image, the possibility of prolonged hospitalization, financial burden, and possible social isolation should be discussed with patients in order to help them make informed decisions [3]. Aggressive management in those presenting late may result in better outcome.