
Abstract
Abstract
Background:
The standard treatment of necrotizing soft tissue infection (NSTI) includes extensive surgical debridement. Care of these debridements is challenging because of the size of the wound and associated pain. A potential solution is to leave the wounds open-to-air in the period after the initial debridement, allowing for regular inspection at bedside while reducing pain associated with frequent dressing changes. We evaluated the feasibility of this approach from a pain control standpoint.
Patients and Methods:
An audit of wound care modalities used on adult patients with NSTI admitted to a regional burn center between January 2009 and May 2014 was performed. Patients with at least one operation were included. Those opting for palliative care were excluded. Wound care was divided into four categories: open-to-air (OTA), negative-pressure wound therapy (NPWT), packing, and ointment. Wound care, pain score, pain medication use, and number of operations were collected for the first seven days after initial debridement. Pain management was assessed by pain scores. Analgesic use was measured and compared using conversion to morphine milligram equivalents (MME).
Results:
Ninety-six patients were included; 67% were men with average age of 50 years, resulting in a total of 672 days of wound care evaluated: 69 days of OTA, 127 days of NPWT, 200 days of packing, and 126 days of ointment (150 days were undocumented). Average daily pain score from all wound care modalities was 2.00. Negative pressure wound therapy had the highest reported daily pain score (2.18, p = 0.034), whereas OTA had the lowest pain score (1.63, p < 0.05). Mortality was lower in the OTA cohort but was not statistically significant; there were no other differences in long-term outcome.
Conclusion:
Leaving wounds OTA is a safe and viable option in the immediate post-debridement period of NSTI to reduce pain, while permitting frequent re-evaluation for quick recognition of disease progression and repeat operative debridement if necessary.
N
Early recognition and treatment are linked to increased survival rates. Once NSTI is diagnosed aggressive surgical debridement of necrotic tissue is the principle treatment option followed by the administration of broad-spectrum antibiotic agents. After resection of the infected tissue has been performed, it is imperative the wound be closely monitored for signs and symptoms of continued infection because it may still progress rapidly despite surgical debridement [3]. Hakkarainen et al. [3] and others [4,5] have suggested routine second-look operations be performed 24 hours after initial debridement to re-evaluate the wound to minimize un-recognized wound infection.
The requirement for frequent re-assessment of the wound may be accomplished in different ways at different centers. Some centers opt for routine operative exploration at pre-determined intervals [6], while others perform dressing changes at the bedside to evaluate the wound [5,7] which has lower cost and resource use but is often painful for the patient.
The senior author (S.D.) developed an alternative practice in which the wound was left completely open to air after initial debridement and assessed visually by physicians and nurses at every clinical assessment in the acute peri-operative period, which usually lasted between one and seven days from initial operation. After the initial infectious episode was determined to be resolved and the wound deemed stable and not infected actively, other options for wound coverage that were more beneficial in promoting healing were used. This article describes a five-year retrospective review of this practice in comparison to other options for wound coverage in this challenging group of patients.
Patients and Methods
The study was performed as a quality improvement initiative and thus the data collection was exempt from formal Institutional Review Board review. We audited the charts of patients admitted to a regional burn center within an academic teaching hospital with diagnosis of NSTI (ICD-9 code 728.86, 608.33, 040.0) between the dates January 1, 2009 and May 16, 2014. Only patients with at least one debridement surgery were included. Patients who opted for palliative care were excluded from this study to eliminate co-existing illness confounding pain scores and pain medication use.
Wound care modality for the first seven days after initial debridement was recorded and divided into four broad categories: open-to-air (OTA), negative-pressure wound therapy (NPWT), packing, and ointment. Pain scores, recorded by visual analog scale (VAS), were gathered for those seven days, averaging the scores to obtain daily means. Pain scores were recorded at least every four hours and in the same manner for all four groups. In cases in which the patient requested more pain medication as needed, an extra set of pain scores were documented. Pain medication was gathered then converted to intravenous morphine milligram equivalents (MME) using the opioid equianalgesia conversion calculator [8]. Cross-tolerance was set to 0%. The MME was then averaged to obtain a daily MME. The daily pain score and daily MME were linked with the wound care modality during that day, effectively eliminating crossover of patients receiving multiple types of wound care. For our mortality and pain analysis, wound care was broken down into two major categories depending on wound care provided in the immediate post-operative period: OTA versus non-OTA. Least square means and type 3 tests of fixed effects were calculated to analyze the data. Mortality, length of stay, and number of debridements were also collected.
Clinical practice and wound care
All wound care modalities were initially performed in the hydrotherapy/debridement room located in the verified regional burn center, with the exception of one intensive care room that contains its own hydrotherapy area. A wound care nurse, primary nurse, and burn care technician performs the procedure. In this area the patient is typically medicated for pain and anxiolysis control, cleansed with a topical antiseptic solution, dried with bath towels, and new dressings applied, if applicable, while connected to continuous monitoring of necessary vital signs.
Choice of wound care modality was determined by attending surgeon preference. No formal protocol was in place during this time, and the choice was based on wound size and location, degree of infection, necrosis and purulence at initial surgery, likelihood for further debridement being necessary, and personal preference.
When a wound is left OTA, the staff washes the patient and wound with a chlorhexidine solution and leaves the wound open to the environment. A heat lamp is placed at a safe distance (six feet minimum) from the wound for several hours per day to promote drying, with an hourly spritz of topical solution by the nurse to prevent excessive drying. The nurses are careful to make sure all muscles and tendons are continuously lubricated in SAF-Gel® (ConvaTec, Bridgewater NJ), an alginate-containing ointment that is usable on infected wounds to prevent overdrying [9]. The patient is educated on the necessity of keeping the wound exposed. Room temperatures are adjusted to patient comfort to assist with removal of bedding covers. Wounds are continuously monitored for disease progression and signs of infection.
When NPWT is ordered the wound care team cleanses the wound and places it in a NPWT dressing either at the bedside or in the hydrotherapy room. There are various types of sponges but the most common that we utilize in our institution is a black sponge. Sponges are cut and pieced together as needed to cover the wound length and depth. An occlusive dressing or drape is then used to cover the wound extending approximately one-half inch around the border of the wound, completely sealing off the wound. A quarter-sized hole is cut into drape over the sponge and a SensaT.R.A.C.™ Pad (KCI, New South Wales, Australia) with tubing is applied in the direction to ensure patient comfort in regards to the tubing. Multiple SensaT.R.A.C. pads are sometimes necessary depending on the size of the wound and amount of exudate. Also, bridging of wounds in close proximity to one another utilizing one NPWT suction setup is often done. Tubing is connected canister tubing and prescribed suction, intermittent or continuous and amount is programmed. The NPWT dressing generally remains in place for 72 hours on continuous suction at approximately 75–150 mm Hg. The primary nurse is responsible for monitoring NPWT output, color, and suction. After 72 hours, the dressing is removed and the physician examines the wound. The wound appearance will determine what the subsequent dressing will entail.
Wound packing involves placing saline or an antimicrobial agent moistened gauze in the wound bed. Gauze bandages are soaked with the prescribed solution to confirm complete coverage then the excess solution is mechanically extracted to leave the gauze dressing applied in the wound damp. Dressings will be periodically moistened to prevent drying or wicked by a dry layer of gauze for a wet-to-dry effect. Red rubber catheters are placed periodically between the moistened gauze and the stabilizing dressing for large anterior wounds to ensure equal distribution of antimicrobial solution and for ease of application. Both forms of wound packing will typically have a supportive outer dressing, usually a tubular netting dressing or ace bandage, for mobile patients. Wound packing is usually performed twice per day by the nursing staff.
Topical ointment placement involves the prescribed ointment to be mixed into a non-adherent dressing such as ADAPTIC™ (Acelity, San Antonio, TX) or Cuticerin® (Smith & Nephew, Fort Worth, TX) and placed on the wound. After placement of the non-adherent dressing the wound is covered by either lap sponges or gauze bandages. A compression dressing is then placed to prevent edema and to help keep the topical ointments from “melting” off. Topical ointments are chosen by the physician based off wound cultures and physical assessment of wound. The wound care staff change topical ointment dressings at least daily.
Results
Of the 96 patients reviewed, 67% were male and the average age was 50. Six hundred seventy-two days of wound care were evaluated: 69 days OTA, 127 days of NPWT, 200 days of packing, and 126 days of ointment (150 days were undocumented; Fig. 1). A total of 55.2% of the patients received NPWT before discharge. Least square mean pain scores and MME averages were 1.63 (standard error of the mean [SEM] = 0.23) and 54.38 [SEM = 5.85] for OTA, 2.18 [SEM = 0.20] and 34.91 [SEM = 3.55] for NPWT, 2.06 [SEM = 0.18] and 35.28 [SEM = 2.69] for packing, and 2.01 [SEM = 0.20] and 35.02 [SEM = 3.75] for ointment (Figs. 2 and 3) Average daily pain score (based on the visual analog scale from 0–10 with 10 being the highest) from all wound care modalities is 2.00 (SEM = 0.07; Fig. 4) Average daily MME for all wound care modalities is 33.22 (SEM = 1.56) MME. The most common drugs used to control pain were morphine, dilaudid, hydrocodone, fentanyl, and ibuprofen.
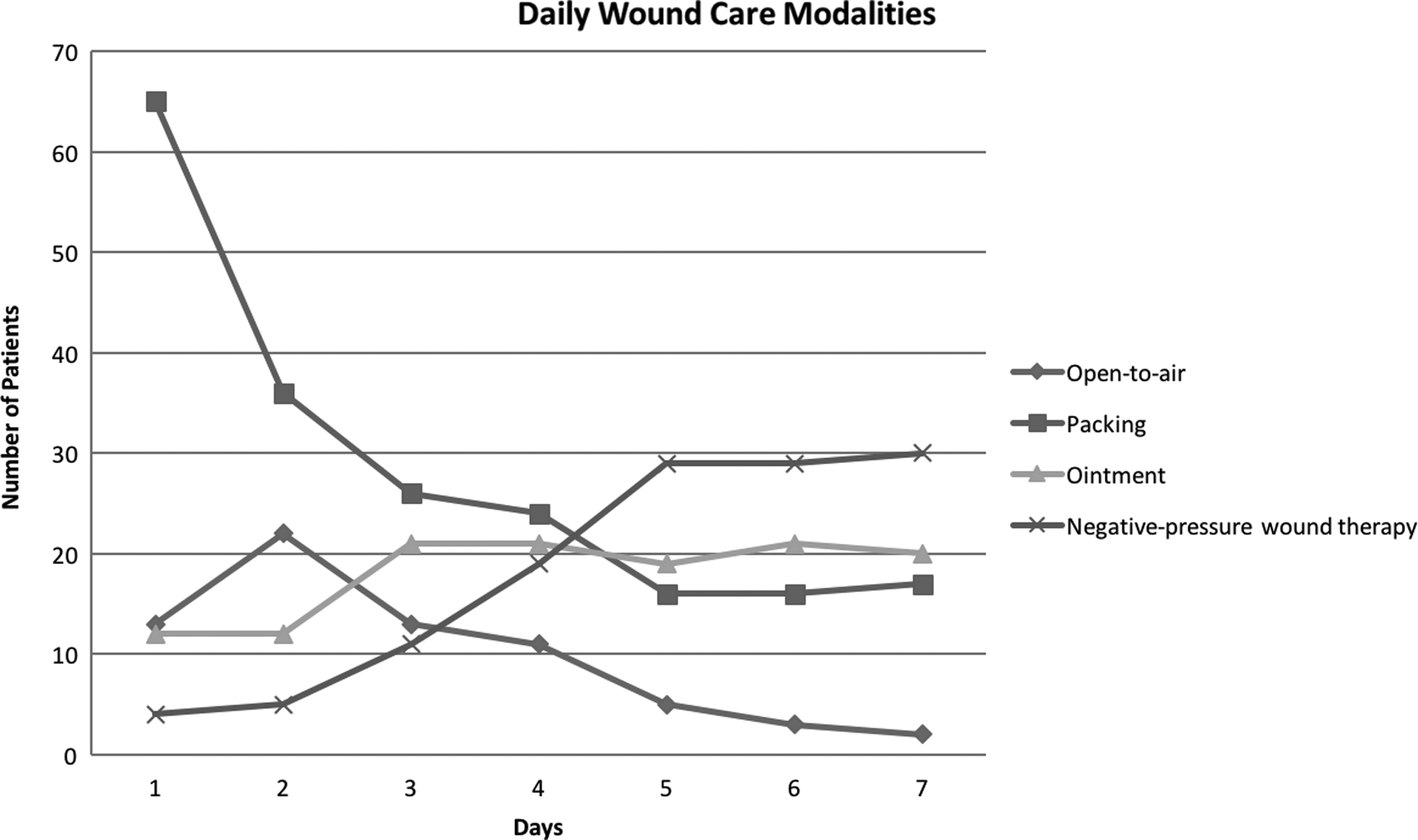
Trend in wound care modalities used during the first 7 days post-debridement. The majority of the patients were packed after initial debridement, and as the week progressed, more patients were switched to negative-pressure wound therapy or ointment dressing.
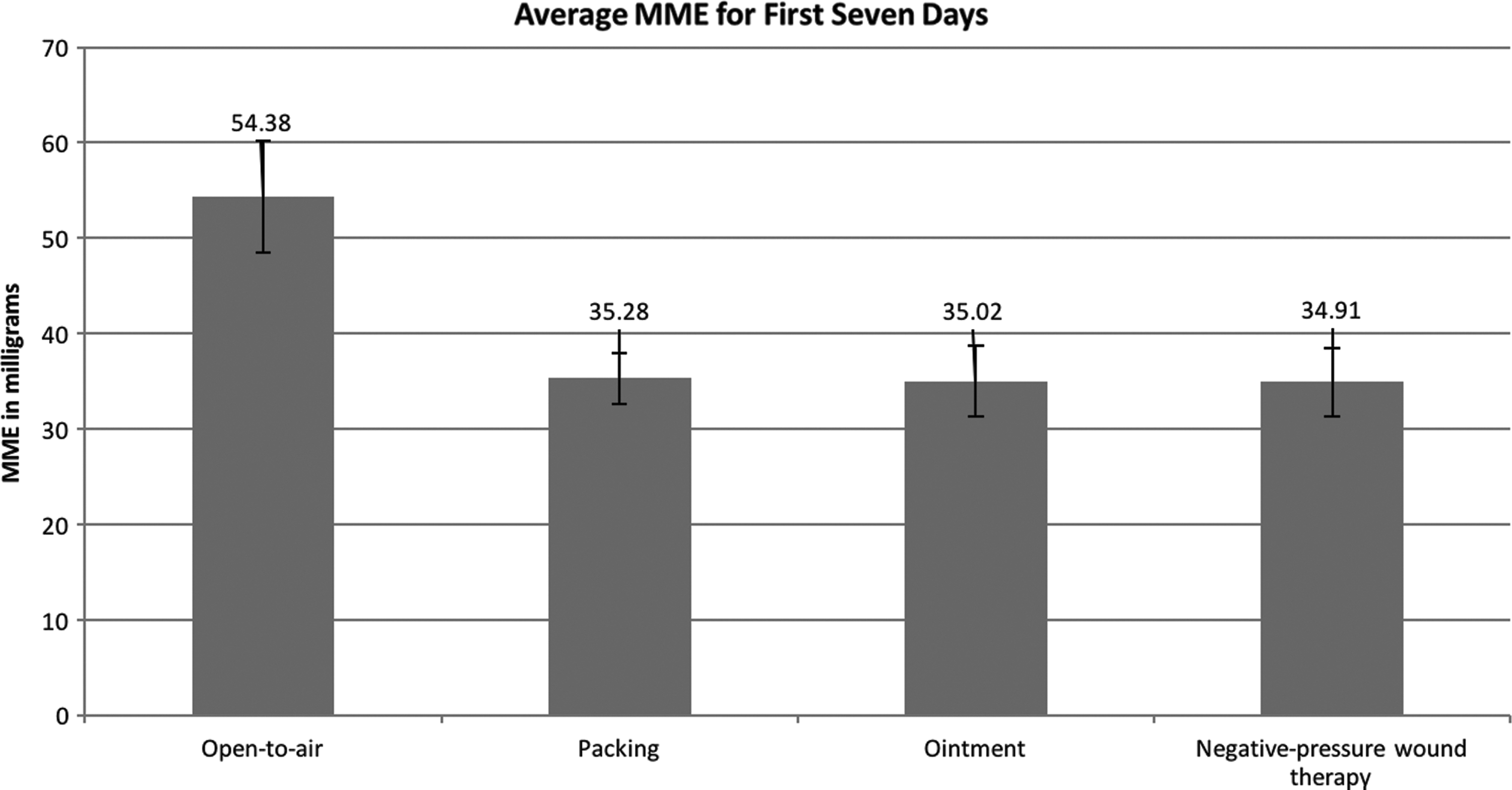
Open-to-air wound care received significantly more pain medication that the other three groups. Error bars are standard error of the mean. MME = morphine milligram equivalent.
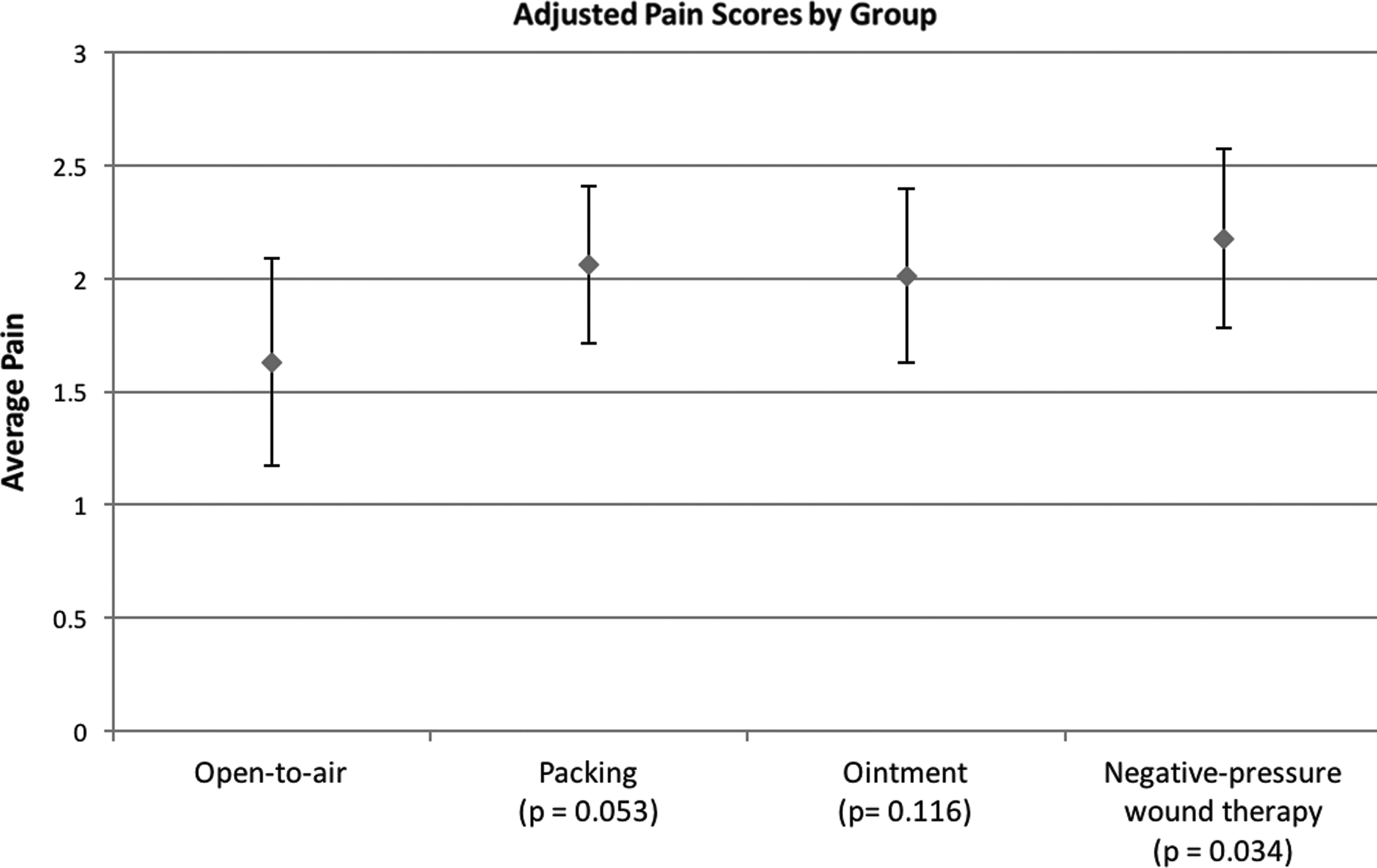
Pain scores adjusted for pain medication received and day of week. Open-to-air still reports the lowest pain score (1.63) whereas negative-pressure wound therapy reported the most pain (2.18). Average pain reported by visual analog scale score (0–10); error bars are standard error of the mean.
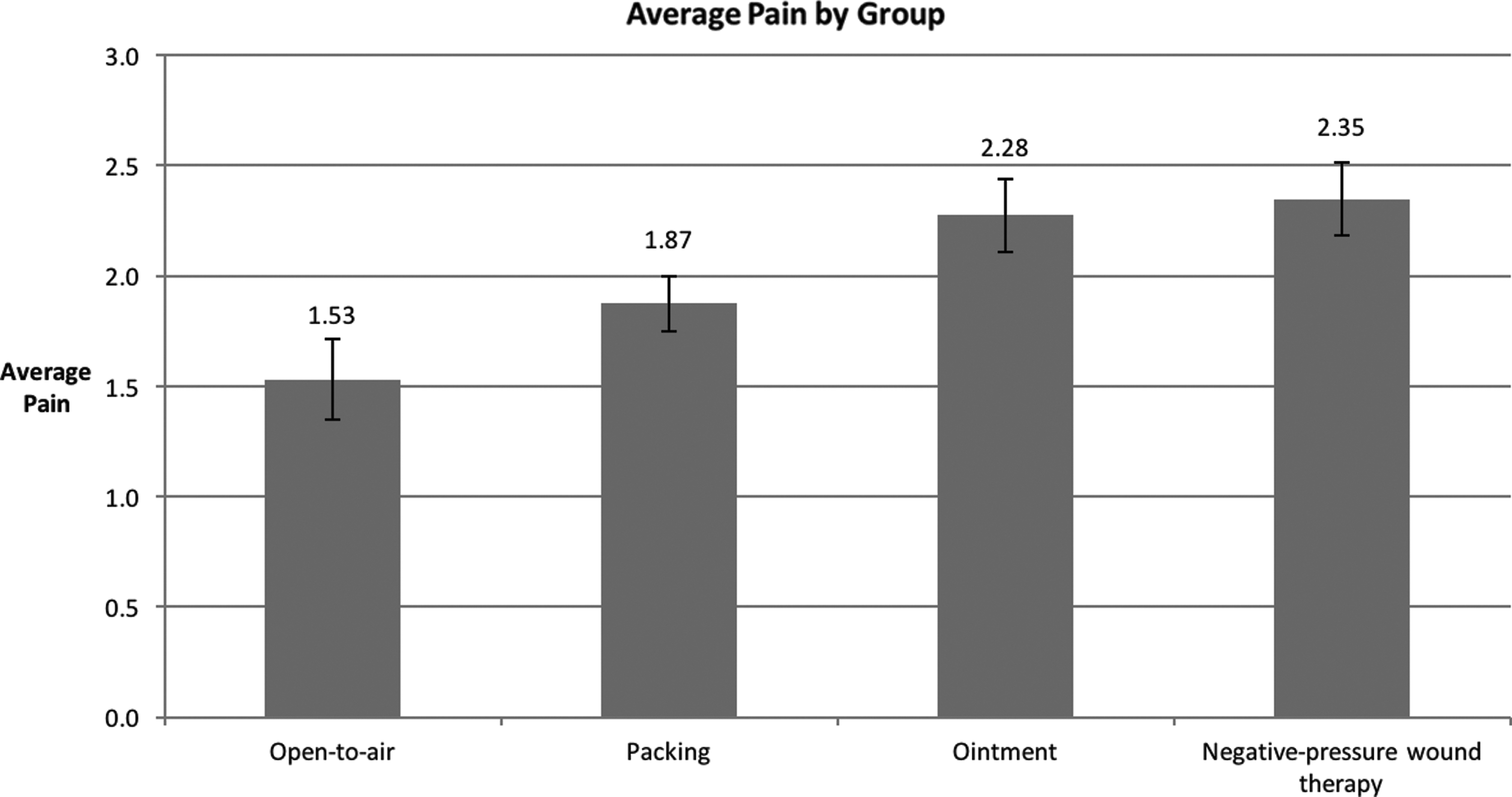
Unadjusted pain scores by group. Open-to-air reported the least pain while negative-pressure wound therapy reported the most. These pain scores do not adjust for day of the week or pain medication received. Average pain reported by visual analog scale score (0–10); Error bars are standard error of the mean.
Because of the apparent difference in pain medication use in the OTA group (54.38 MME), mixed models were used to estimate the difference in average daily pain for open-to-air versus non-open-to-air subjects after adjusting for differences in MME and day of treatment. The day was treated as a repeated measure under the assumption of compound symmetry and differences in subjects were modeled using a random effect. The group effect was not observed to have a statistically significant (p = 0.165) effect upon pain scores, but a pre-planned pairwise comparison of means of each group to the open care group, in which we only compared pain scores of OTA to each of the competing wound treatment regimens, suggested that pain scores in the NPWT group were higher (p = 0.034), even after adjusting for differences in pain medication use and day of treatment (Fig. 3). The mixed models described above also makes it appear that open treatment is much less painful (p < 0.05) than any of the other treatment groups after adjusting for differences in MME and day of treatment (Table 1).
Type 3 tests of fixed effects, adjusting for MME and days of treatment.
MME = morphine milligram equivalent; Num df = numerator for degrees of freedom; Den df = denominator for degrees of freedom.
Patients with OTA wound care averaged 2.08 debridements and returned to the operating room 30 times among 26 patients whereas all other wound care averaged 1.75 debridements and returned to the operating room 53 times among 70 patients. A total of 65% of the OTA group returned to the operating room compared with 54% (p = 0.50) of all other wound care regimens. Average debridements across all wound care were 1.8. There were no documented instances of return to operating room for desiccation of muscle tissue or other potential complications of OTA. All re-operations in the acute period were for re-evaluation of the wound to assess for recurrent or spreading infection, or further debridement.
Open-to-air had a mortality rate of 3.8% (1/26) whereas all other wound care was 7.1% (5/70), which was not statistically significant (p = 0.56); overall mortality was 6.25%. Average length of stay was 17.25 days.
Discussion
Necrotizing soft tissue infections require extensive wound debridement and as a result, extensive wound care. The literature on wound care is lacking and there is no current consensus on best wound care modality, and thus treatment is left up to the clinical judgment of the physician. At our institution, four major wound care methods are used for our patients post-debridement: OTA, NPWT, packing, and ointment.
Leaving a patient's wound OTA after debridement is a novel yet simple approach and is beneficial to the patient and healthcare providers. It allows for continuous wound assessment to identify within minutes the need for further surgical debridement of the rapidly progressive infection without the need for painful, labor-intensive dressing changes. Our hypothesis was that OTA would allow for easier detection of spreading or recurrent infection in the wound by bedside clinicians, thus allowing us to return to the operating room when necessary to improve outcome. Our study revealed that mortality and return to operating room between the two groups were not statistically different, showing that OTA is an equally acceptable wound care method in the immediate post-operative period. Open-to-air had a higher operating room return rate of 65% versus 54%, and a lower mortality rate of 3.8% compared with 7.1% of all other wound care. This suggests that changes in the wound suggestive of spreading infection is easily recognizable with OTA wound care without the pain associated with traditional wound care methods.
It is well known early and complete surgical debridement is necessary to improve survival and is considered the gold standard [3,7]. However, a single surgical debridement often is insufficient, with patients averaging three to four debridements [3]. An exposed wound would allow for early identification of continued infection and the need for further debridement to halt progression and allow for simultaneous critical care interventions before multi organ dysfunction and ensuing death. Although a direct relation between wound care and mortality cannot be made due to many confounding variables, our study suggests the potential that leaving wounds OTA temporarily may actually decrease mortality. It is also important to note that having an exposed wound can have potential psychosocial side effects and it is critical to educate the patient and family on the vital importance of monitoring the wound closely. Topical antimicrobial agents and solutions are noted in literature to be the most traditional wound care modality until definitive source control [7,10]. Deep wounds may be packed with saline or antimicrobial-soaked packing gauze and more superficial wounds may require ointment-soaked gauze. Because thorough and frequent assessments of the wound are necessary, dressing changes may occur two to three times per day, which may be excruciating for patients. Our institution also utilizes a variety of creams, ointments, and aqueous solutions to maintain a moist wound base to promote healing, but require complete removal to accurately inspect the wound. Liquid solutions are less painful to remove, but when used with gauze dressings can cause shivering or lead to hypothermia depending on the frequency of application. Controlling pain and anxiety is essential when performing dressings changes, but could potentially mask a pathologic process or influence cognition.
Many clinicians prefer the use of NPWT dressings for wound management because of the ease of application, decreased dressing changes, and faster healing times [11]. The action of NPWT is to promote tissue granulation and epithelialization by placing the wound bed in sub–atmospheric pressure vacuum. The negative pressure in turn draws exudate away from the wound and promotes angiogenesis [11]. Although NPWT is touted as a non-painful method of wound care, clinicians should use it cautiously because it may cause increased pain and skin trauma, therefore decreasing patient well-being and satisfaction [12,13]. This increased stress and anxiety has been shown to delay wound healing [14–19] In an investigative study interviewing wound care clinicians, it was found that patients experience moderate to severe pain frequently during the application or the removal of NPWT dressing [19]. Our study showed that in patients with NSTIs who require surgical debridement, those with NPWT reported a higher pain score than those receiving other wound care.
An interesting finding in this study was that although pain scores in the OTA group were lower even after adjustment for their higher narcotic use, this group still was given a much greater dose of opioids than the other patients. This may reflect an assumption by nursing staff of increased pain based on the acuity of the immediate post-operative period as well as the visual stimulus of a large open wound that is likely perceived by the observer—consciously or sub-consciously—as more painful than a similar wound that is covered in dressings. During the initial implementation of OTA treatment there were significant concerns by nurses and physicians that this modality would be too painful to tolerate and that patients and families would not accept this treatment. Although anecdotal, this lends some credence to the hypothesis that the higher opioid doses reflect bias on the part of the caregiver rather than the patient.
Limitations to our study include single-center retrospective study, loss of some wound care or pain score documentation, and lack of baseline visual analog scale score. In addition, wound size and depth were not evaluated because of the retrospective nature of the study. The authors did not evaluate specifically patient or family satisfaction with OTA; given the resistance to the initial implementation as described above, this would be an interesting aspect to explore. The idea for this study arose because one surgeon routinely used OTA based on personal success with this technique whereas others did not, thus allowing for a comparison to be performed. However the non-randomized nature of patient allocation to each wound care category, as well as the inability to determine why a particular wound care modality was chosen based on retrospective documentation review alone, leads to the possibility of multiple confounders. The timing of return to the operating room was not evaluated in this study; given the hypothesis that one benefit of OTA was quicker return when needed, this is an area we intend to explore further in a future study. Our single-center analysis suggests use of OTA wound care in patients with NSTI reduces pain and may improve patient outcomes.
Footnotes
Acknowledgments
The authors would like to thank the staff of the Timothy J. Harnar Burn Center, Lubbock, Texas, for their excellent patient care and cooperation with this review of our wound care practices.
Author Disclosure Statement
There are no conflicts of interest and no funding received for the work done.