
Abstract
Abstract
Extensive studies on foot traffic in the operating room (OR) have shown little correlation between surgical site infections (SSIs) and traffic of OR personnel in and out of the OR. While evidence supports the relation between foot traffic in the OR, airborne bacteria, and subsequent SSIs in orthopedic surgical procedures, the studies were conducted over four years and in more than 8,000 patients. The direct relation this finding has to general surgery patients has yet to be proven; however, protocols to reduce foot traffic may have a beneficial effect for the OR team.
A
In this study, evidence to support the hypothesis that airborne bacteria pervaded the OR environment was based on data using “drop plates” or petri dishes containing bacterial culture medium, placed on surfaces in the OR. The bacteria that landed on the drop plates at the time of operation had lower bacterial counts when the room had UV light than when there was no UV radiation. No significant reduction of SSI was found with the UV light, and this prevention management is no longer used in the OR.
The study did elucidate the importance of wound classification related to SSIs. The classification was adopted by Cruse [2] who initiated a wound surveillance program as part of post-operative management and carefully documented observations for more than a decade. These data help provide a firm basis for identifying the source of infections, as well as other extrinsic factors such as the importance of skin preparation, pre-operative hospital stay, the surgeons' scrub time, and duration of operation. This exhaustive work by Cruse [2] provided a standard for infection prevention.
That the duration of operation can affect the SSI rate raises the question of what, if any, external forces can result in a higher SSI. Is it simply that the longer operation is because of many minor surgical misadventures or that a slow surgeon exposes his patients to more bacterial-laden air that eventually lands in the patients' wound and overwhelms the patients' local immune resistance?
In our current healthcare environment, “bundling” prevention measures to manage a single patient has a proven impact in reducing infection. Order sets appear to have a greater influence than single/isolated ones [3]. This approach has been used to reduce foot traffic among other activities in cardiothoracic surgery [4]. Perhaps this approach should be a standard for all clean wounds. The argument to institute such a demanding approach is based on Cruse's data, which show that while contaminated and dirty wounds have a higher infection rate, overall the frequency of the high risk procedures are far less than clean operative procedures. While the rate of SSI in a clean wound is small, there are many more of them [2]. Cruse [2] found that 25% of all SSIs come from clean wounds. In the recent past, ORs were fashioned with windows of grand views, some with windows that could be opened on a hot day to allow “fresh” air. The current standard for OR design has carefully regulated airflow and filtration.
OR Traffic, SSI, and Airborne Particles
Air sampling in the 1960s and 1970s was performed with drop plates—culture plates placed on the surfaces in the OR theater followed by incubation and colony counting [5]. This technique was only partially quantifiable because the number of colonies present on the drop plates could be counted, but the size of the air sample represented could not. The drop plate approach has been replaced by self-contained instruments, which suck air onto a filter at a fixed rate (Fig. 1). The filter size is small enough to capture bacteria (three microns) and is used in most current air studies [6,7]. The filters are then placed on culture media, incubated, then colony counts performed on the plates. The number of bacterial colonies is a function of the volume of air aspirated by the sampling instrument.

An air sampling device made by Sartorius Mechatronics [6].
Similarly, Stauning et al. [7] used air particle counts and performed an analysis by continued assessment of OR staff behaviors using a motion tracking system. The impact on the SSI risk was determined during surgical procedures, measuring microbiologic air counts and wound sampling counts as a surrogate for SSI risk. They concluded that door openings affect air contamination that could jeopardize OR room sterility and believed that behavioral aspects are critical for the control of the exogenous risk of SSI.
Once again, airborne bacteria were related to traffic flow but not to the SSI. In fact, the weakness of these data is the loose correlation between high bacterial counts on the air filters and the actual rate of SSI. Specific culture of airborne bacteria as related to a specific surgical infection is lacking. One classic article published in 1976 [8] assessed the SSIs in surgical patients before and after a renovation of the surgical suite. In an analysis of the SSIs immediately before the renovation, one patient had an infection attributed to an “environmental” cause. The patient had a post-hysterectomy wound infection, and the organisms recovered were Enterococcus and Proteus mirabilis, both flora from the intestinal tract. While it is possible that these organisms could have contaminated the wound from the air, it is more likely that they inoculated the wound by direct contact. After the renovation, the colony counts in agar gels placed in the OR were nearly half of the levels than before the renovation, and no SSIs were identified that could have been from the environment.
This best current evidence that personnel movement in and out of the OR causes an increase in the infection rate is based on the assumption that the more people come and go from an OR, the more bacteria become airborne. A significant negative impact on the OR environment was demonstrated by the air quality, expressed as colony-forming units per cubic meter (CFU/m3) during orthopedic trauma surgery in a displacement-ventilated OR. The study demonstrated how traffic flow and the number of personnel present in the OR affects the air contamination rate near surgical wounds. Their data showed a strongly positive correlation between the total CFU/m3 per operation and total traffic flow per operation, after controlling for duration of surgery [6]. Unfortunately, there is no specific correlation with the rate of airborne bacteria and subsequent SSI.
The most convincing evidence that airborne bacteria have direct impact on subsequent SSI is from a series of studies from the UK evaluating an “ultraclean air” air handling system and joint replacement. Cases were followed for one to four years [9–11]. During the operative procedures, wound irrigation to detect bacterial contamination was correlated with air quality sampling to determine the impact on subsequent prosthetic infections. The impact of ultraclean air reduced infections from 1.5% to 0.6%, a significant infection reduction. An important component of these data—that patients were followed for years not weeks and had large prosthetic devices placed in their deep wounds. How this relates to non-implant surgical procedures is speculative [12].
OR Traffic and Staff Behavior
While compelling evidence for increased infections in other operations is difficult to identify, there are a number of studies that document excessive turnover of all members of the OR staff during surgical procedures [13–21]. With the exception of the surgeon, OR techs, nurses, certified registered nurse anesthetists, and anesthesiologists come and go from the OR on a regular basis. The behavioral aspect of OR foot traffic has elucidated enough curiosity to result in numerous studies, mostly in the orthopedic, cardiac and neurosurgery fields, which are often longer cases than in general surgery.
The volume of OR traffic appears to correlate with the duration of the surgical procedure [16] (Fig. 2). These studies have analyzed the number of door-openings per hour, the duration of the door openings, the reasons for door opening, as well as the number of OR personnel moving in and out of the OR. A mean rate of 40 door openings per hour for orthopedic total joint operation has been reported [12], with some studies reporting more than 50 per hour [16] and others reporting a rate of 12.9/h in trauma orthopedic ORs [6] and a mean rate of 19.2/h for cardiac surgery [22]. Most studies concluded that the reasons for door openings could not be explained [6,16,18].
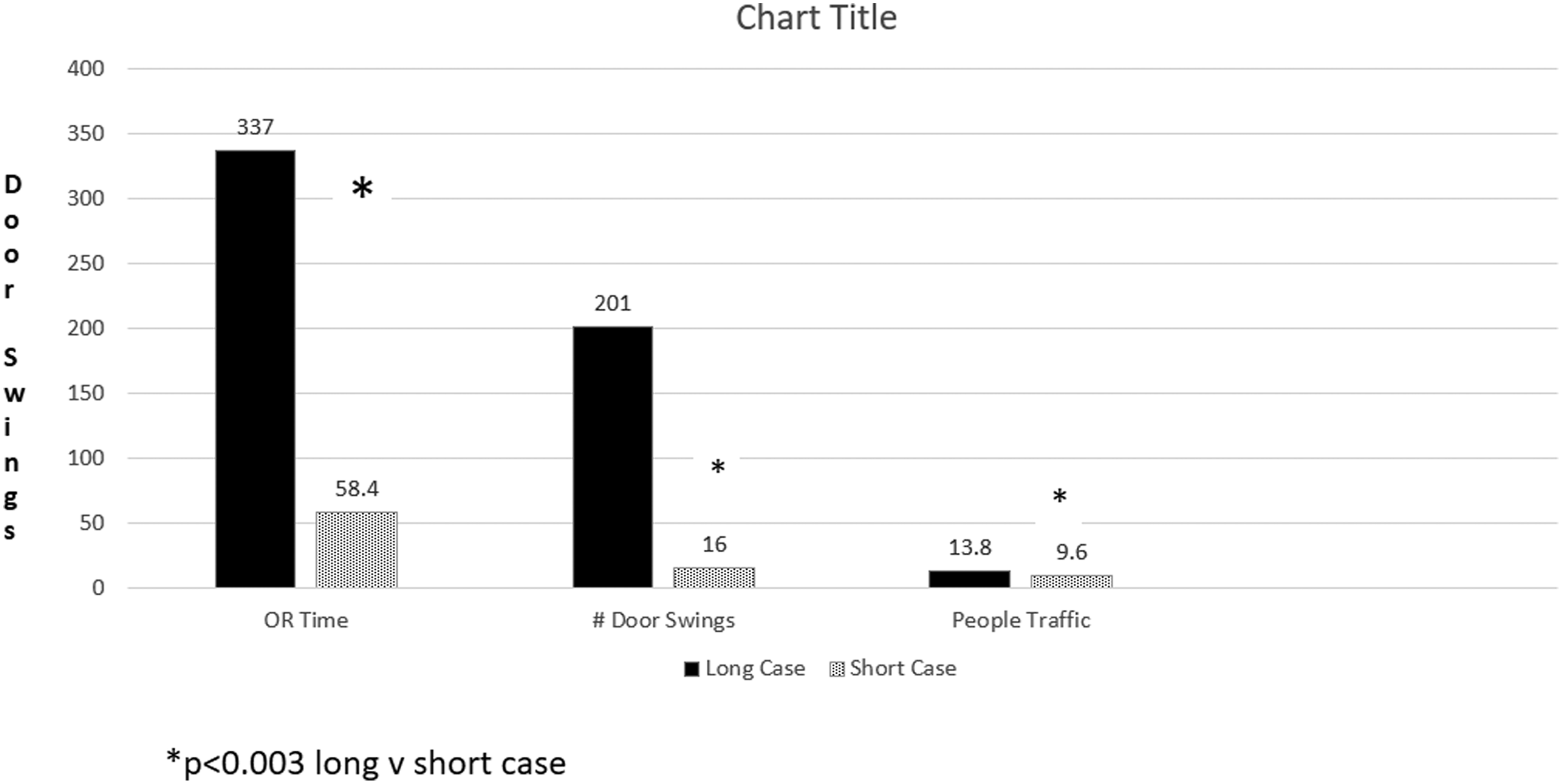
Relation of duration of surgery, the number of door swings, and the movement of operating personnel [16].
Parikh et al. [16] performed a prospective observational study basically evaluating the role of monitoring and the possible Hawthorne effect. They compared THE number of OR door openings, duration of the OR door openings, and number of OR personnel while being monitored. They concluded there was no role of surveillance of OR traffic demonstrated by no difference in number and duration of door openings between control and surveillance group. Thus, Parikh et al. [16] suggest that to achieve any change in OR traffic pattern, monitoring alone may not be sufficient.
In a second study, however, there was a process to minimize the foot traffic by all OR staff by better organizing the staff and making them aware of their activities [18]. This resulted in a significant reduction in the number of door openings by nurses, technicians, and surgeons, but no effect on infection rates was noted (Fig. 3).
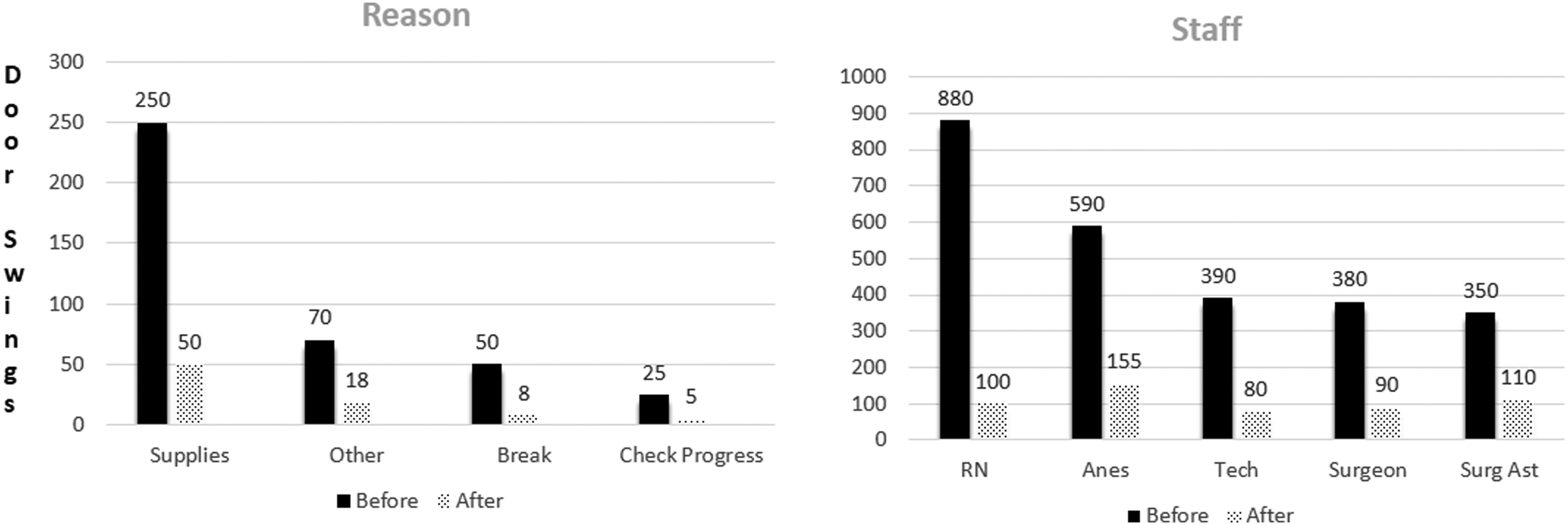
Control of operating room (OR) traffic: May be achieved by developing protocols as to when to enter the OR during a surgical procedure [18].
The duration of operation and the OR traffic during operation intuitively seem to be related and consequently impact on the rate of the SSI; but while evidence supports the principle that the duration of operation can contribute to the SSI rate [23,24], OR foot traffic does not appear to be an independent risk for SSI [23]. The patient population was restricted to clean, elective operative surgical procedures, and the follow-up was 30 days, a short interval compared with the orthopedic studies that were followed for four years [9,19]. It is difficult to develop a cohesive hypothesis as to why foot traffic is not an independent risk factor for infection.
A study from 1963 provides some insight to this relation between foot traffic, wound contamination, and subsequent wound infection [25]. Wounds from a series of 50 patients who had thoracic or abdominal operations were surveyed for Staphylococcus contamination and phage typed (Fig. 4). These strains of bacteria were compared with the patients' own flora as well as that of the surgical team and air samples. Twenty-four wounds had Staphylococcus contamination and, on average, there were six different strains in each of the wounds.
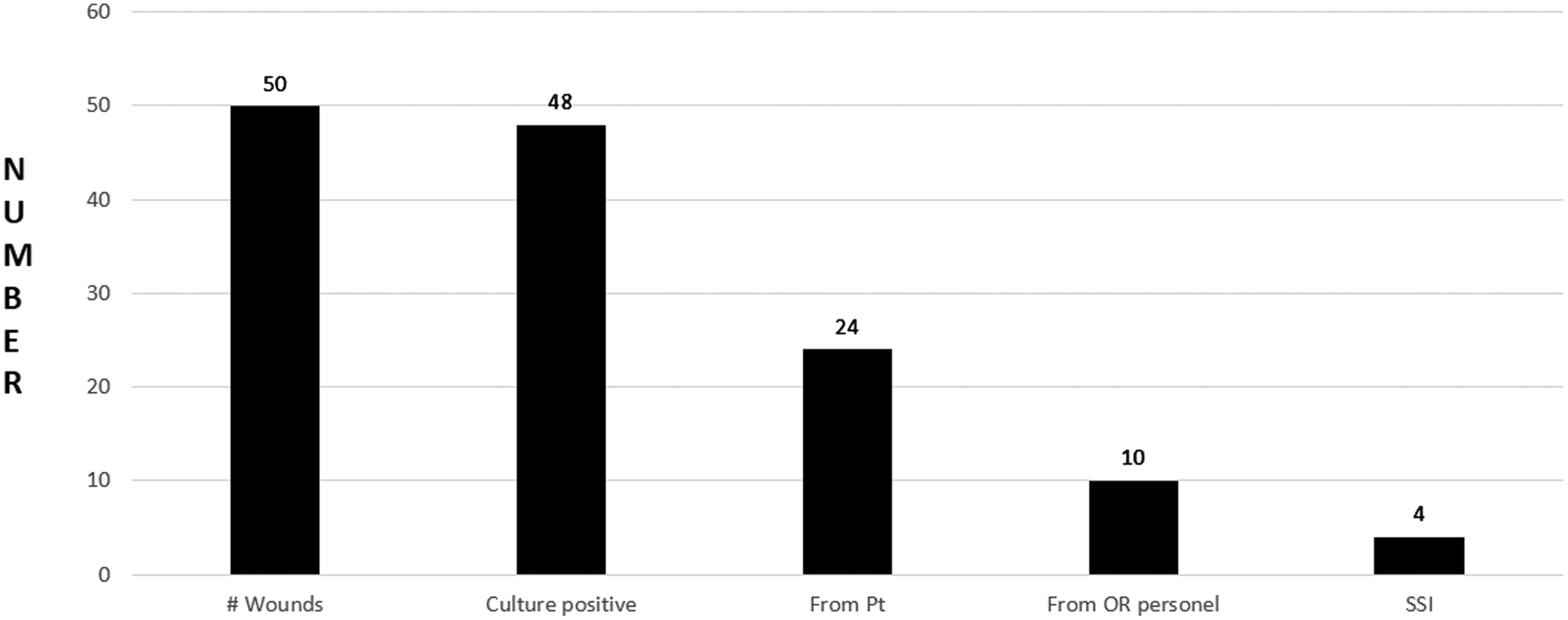
Bacterial contamination during surgical procedures [25].
The most common source of contamination was from the air; however, an SSI developed in four of the wounds. While the wound infection rate of 8% is high by our current standards, only 16.7% of contaminated wounds resulted in an infection. While airborne contamination is common, this event infrequently results in a bacterial inoculum that overwhelms the local immune resistance [26]. This statement is supported by the 1964 study [1] by the American College of Surgeons where operations in ORs equipped with UV light were compared with surgical procedures performed in the absence of UV light. The trial resulted in no difference in the post-operative infection rate.
Conclusion
Understanding the bacterial sources of SSIs and controlling them has been a long process that began in the late 1950s and early 1960s. Clearly SSI is complex and multi-factorial. Risk factors that increase the incidence of SSI have been well described, including patient co-morbidities, wound contamination class, operative time/duration, intra-operative parameters, among others. Despite very well established preventive measures, SSIs still occur and are a measure of our competence and quality as surgeons. In addition, SSIs have a large economic impact on the patient, provider and healthcare system. The CDC guidelines from 1999 recommend to limit the number of OR door openings to a minimum and to limit the number of people in the OR.
This review sought to determine whether there are any data to support these recommendations based on “expert advice” [27]. It appears that direct cause and effect for most surgical procedures is lacking. Data available do not determine causality and appear limited to specialties like orthopedic and cardiothoracic surgical procedures, which involve implantation of hardware or involve longer cases. It is intuitive, however, that reducing OR traffic improves the level of team discipline, concentration, and reduce at least one external variable for SSI. Distractions are rampant in our day-to-day activity, and this has invariably seeped into our ORs. It seems appropriate to reassess our conduct in the OR with an attempt at a reduction of operative time. There are only limited data that a bundled order set including a reduction in OR traffic flow can effectively reduce SSI [4].
The relation between operative time and traffic flow is clearly related [6,16–18,21]. Does this explain why prolonged surgical procedures result in a higher infection rate(24)? Because we, in the healthcare system, are expected increasingly to reach a perfect outcome, especially in elective surgical procedures, it may be time to control all of those factors that can be controlled to improve results, which includes minimizing OR foot traffic.
Footnotes
Author Disclosure Statement
No competing financial interests exist.