
Abstract
Background:
Bacterial infections are a common complication after liver transplantation. Usually, abdominal drains are placed at the end of the surgical procedure. The usefulness of routine drain tip culture has not been investigated.
Patients and Methods:
This retrospective study included 200 liver transplants between 2010 and 2015. We excluded patients without drain tip culture and those with abdominal or systemic complications before removal of drains. Demographic, clinical (pre-transplant, peri-operative and post-transplant) and microbiologic information were collected up to 30 days after operation. Three-month survival and re-transplantation were recorded.
Results:
There were 94 patients included. Drain tip culture was positive in 78 (83%) patients. The most common isolates were coagulase-negative staphylococci (30.9%), mixed gram-positive cocci (13.8%), and polymicrobial (21.3%). In 26 patients, 35 post-operative infections developed, with no differences between recipients with and without positive drain tip culture (22.8% vs. 25%; p > 0.99). In two patients, Staphylococcus aureus was isolated in drain tip cultures and in cultures confirming the post-operative infection (one catheter-related bacteremia and one drain-related peritonitis). In two other recipients, the positive drain tip culture had an impact on clinical management. All patients survived.
Conclusions:
Routine drain tip culture in asymptomatic liver recipients seems unhelpful. It may be more reasonable to perform it only in patients with suspicion of complications.
Liver transplantation is indicated in patients with decompensated cirrhosis, acute liver failure, and certain hepatocellular carcinomas [1,2]. The procedure is associated with significant morbidity and death, however. Most deaths occur in the early post-transplant period. Infections and intra- and peri-operative complications are responsible for approximately 60% of deaths and graft losses during the first post-operative year [1,2].
An infection will develop in approximately two-thirds of recipients after liver transplantation [2]. Bacterial infections are predominant during the first two months after the procedure [3], and three-fourths of bacterial infectious episodes occur in the first month after operation [4]. Thus, in addition to the immunosuppressive treatment and the epidemiologic exposure, the risk of infection varies according to the time point after transplantation [1,3,5].
Surgical site infections are infections of the incision, organ, or organ-space [6] and are the most frequent bacterial infections in the immediate post-transplant period. They can be classified into superficial, deep, and organ-space. This last group is significantly associated with graft loss and patient death. These infections occur within 30 days after liver transplantation [3,7].
Traditionally, and as part of standard practice, at least one abdominal drain is placed toward the end of a liver transplant procedure to prevent fluid collection (subphrenic or subhepatic), to identify post-operative bleeding or bile leak, and to drain ascitic fluid [8].
The primary objective of this study was to investigate the relationship between micro-organisms isolated on routine culture of abdominal drain tips and the infections occurring during the first month after liver transplantation. As a secondary objective, we studied the impact of culture findings on the recipient's clinical management, three-month survival, and re-transplantation.
Patients and Methods
Data collection: Settings, study population, and microbiologic results
On the basis of a prospectively registered cohort, we conducted a retrospective study, including all consecutive adult (>18 years) liver transplant recipients, performed at Hospital Universitari Vall d'Hebron (Barcelona, Spain) between January 2010 and December 2015. The study was approved by the hospital Ethics Committee for Clinical Research.
For the purposes of the study, we included only patients whose drain tips were sent for culture and excluded patients with complications in the early post-operative period, because drain tip culture would have been indicated in these cases. Thus, we established the following criteria for exclusion: (1) Abdominal complications, including re-intervention, hemorrhagic shock or hemoperitoneum, peri-hepatic hematoma or collection, and prolonged paralytic ileus; (2) systemic complications, including re-transplantation, patients who remained critically ill, and patients who died before removal of abdominal drains; and (3) infections (diagnosed or suspected) before removal of the abdominal drains.
In our hospital, abdominal drains (Jackson-Pratt®) are placed at completion of liver transplantation, usually one in a subhepatic and another in a suprahepatic position. Additional drains may be needed depending on the type of surgical procedure. Drains usually are removed around the fifth post-operative day, and abdominal drains tips are sent routinely to the hospital microbiology department for culture. As part of the standard clinical management in liver transplantation, abdominal ultrasonography is performed routinely during the first days after transplantation.
Our standard antibiotic prophylaxis is amoxicillin-clavulanate 2 g every 8 h for 48 h.
The recipient's demographic, clinical, and microbiologic data were collected by clinical chart review. The clinical data included pre-transplantation, peri-operative, and post-transplantation information up to 30 days after transplantation. We also registered three-month survival and re-transplantation. Data referring to post-operative infection included the infection site, microbiologic information, antibiotic treatment, and clinical complications from infection, including death. In patients with a negative drain tip culture, we collected only the site of infection and microbiologic information. The microbiologic data included information from drain tip culture and cultures related to post-operative infections during the first month after the procedure.
Peri-hepatic hematoma can be a potentially serious complication [9], but it can also be an incidental finding in the immediate post-operative course that gradually resolves with no consequences for the recipient [10]. In our study, all patients with a diagnosis of peri-hepatic hematomas were completely asymptomatic. Therefore, we performed a subanalysis in this group.
Definitions
Infections were defined according to Centers for Disease Control and Prevention criteria [7]. Post-operative infection was established as an infection that developed within the first month after the procedure. Micro-organisms isolated in a patient with no clinical signs of infection and febrile episodes in which no micro-organism was isolated were not considered true infections, as described elsewhere [11]. Poly-microbial infection was established when gram-positive and gram-negative micro-organisms were both isolated in culture.
Microbiologic processing
Drain tips were vortexed with a small amount of saline or thioglycolate broth, and the resulting samples were cultured in enriched solid media incubated under aerobic and anaerobic conditions. Bacterial growth was evaluated semi-quantitatively. Microbial identification was performed using the Vitek MS (MALDI-TOF) and Vitek 2 systems (BioMerieux, France). If appropriate, antibiotic susceptibility tests were performed using Vitek 2 or the disc diffusion method (Rosco Diagnostica, Denmark). The recommendations of the European Committee on Antimicrobial Susceptibility Testing and guidelines of the Clinical and Laboratory Standards Institute were followed.
Statistical analysis
The frequencies and percentages were calculated for categoric variables and the medians and ranges for continuous variables. Bivariable analysis was performed using the chi-square test to compare the incidence of post-operative infections between recipients with a positive drain tip culture and those with a negative culture. The threshold of statistical significance was p < 0.05. The statistical analysis was performed with IBM SPSS Statistics for Windows, Version 20.0. (IBM Corp; Armonk, NY).
Results
Population characteristics
In the period of January 2010 to December 2015, 200 adult liver transplants were performed in our hospital. After the procedure, abdominal drains were removed, and the drain tip was not sent for culture in 43 recipients. Among the remaining patients, systemic complications developed in 14, 27 had abdominal complications, and 22 had an infection (diagnosed or suspected) before removal of the abdominal drains. Ultimately, 94 patients with no previous complications were included in the study (Fig. 1).
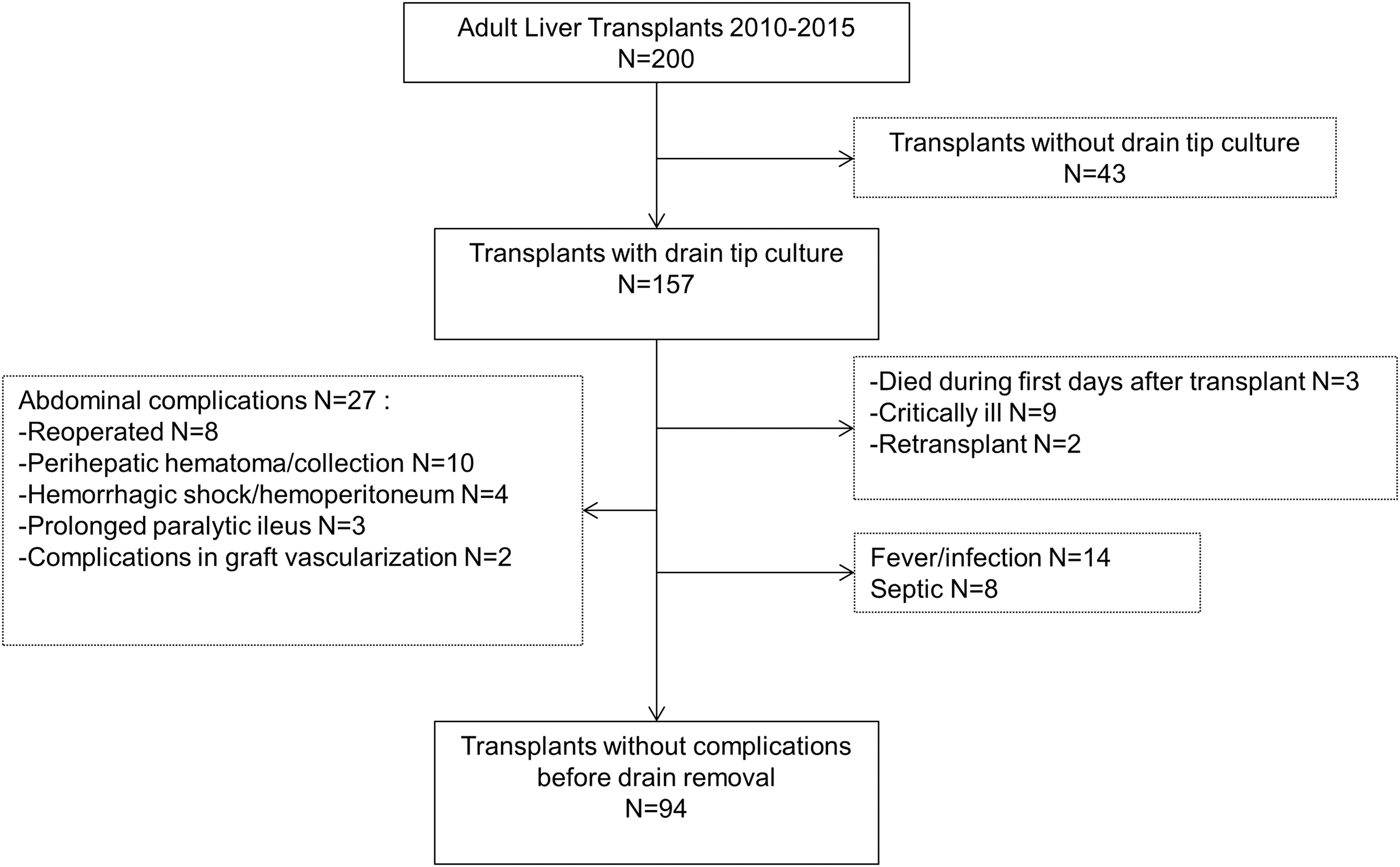
Patient recruitment flowchart.
Median age of the patients was 56 years (range 22–69), 80% were older than 50 years, and 68 (72.3%) were men. Cirrhosis was the main reason for transplantation (50%). The most frequent causes of cirrhosis were alcohol consumption (36, 38.3%) and chronic hepatitis C infection (32, 34%). Hepatocellular carcinoma was present in 46.8% of cases. The most commonly used peri-operative antibiotic agent was amoxicillin-clavulanate (79.8%). There were no complications during the surgical procedure in the majority of cases (84%). All patients survived to the end of follow-up (three months). Additional characteristics of the study population are summarized in Table 1.
Baseline Characteristics of Recipients
HCV = hepatitis C virus; MELD: Model for End-stage Liver Disease; HIV = human immunodeficiency virus; MP = methylprednisolone; MMF = mycophenolate; ATG = antithymocyte globuline.
Data are expressed in numbers and percentages unless otherwise indicated
Drain tip culture was positive in 78 (83%) recipients. Coagulase-negative staphylococci (CoNS) were the most frequent bacteria isolated (30.9%). Other mixed gram-positive cocci were present in 13.8% of cultures; in 21.3% the isolation was polymicrobial, and 17% of cultures had negative results. Other micro-organisms and their frequency are summarized in Table 2.
Micro-Organisms Isolated in Drain Tip Culture
GPC = gram-positive cocci.
Data are expressed in numbers and percentages unless otherwise indicated.
Post-operative infections
After liver transplantation, 26 (27.6%) patients experienced 35 post-operative infections. Most had only one infectious episode, whereas seven patients had two episodes and one patient had three.
There was a median of 14 days (range 5–30) since transplantation to the first infection. Among bacterial infections, the most frequent was respiratory infection with six (17.1%) episodes, followed by urinary infection (five episodes, 14.3%), and surgical site infection (four episodes, 11.4%), among which two infections were superficial and two were organ-space infections. During the study period, there were also nine episodes of cytomegalovirus viremia and four episodes of herpes virus stomatitis.
Drain tip culture was positive in 22 of the 26 (84.6%) patients who experienced at least one post-operative infection.
Regarding the primary objective of the study, 22 of the 78 (28.2%) recipients with a positive drain tip culture had a diagnosis of a post-operative infection, a percentage similar to those with a negative culture, four of 16 (25%, p > 0.99).
In two patients, the micro-organism isolated at the diagnosis of infection was consistent with that of the drain tip isolate: Staphylococcus aureus in both cases. Catheter-related bacteremia developed in one of these patients and a drain-related peritonitis developed in the other. Both patients were treated accordingly, and both did well.
Regarding the secondary objective, the positive drain tip culture result conditioned the clinical management in two recipients. Neither one had severe complications (renal impairment, septic shock, or respiratory failure).
One recipient received a diagnosis of an intra-abdominal abscess a few days after drain removal. The patient received targeted antibiotic treatment against Pseudomonas aeruginosa, which had been isolated from the drain tip. No other sample was collected to confirm P. aeruginosa infection, however.
Another recipient, who was still in the intensive care unit at the time of drain removal, was treated because the drain tip culture yielded multiple gram-positive cocci, although there were no symptoms of infection. Blood cultures tested negative, and the recipient did well.
Peri-hepatic hematoma
In the peri-hepatic hematoma subanalysis, there were no complications during the surgical procedure in the majority of patients (8/10), whereas one patient experienced a gastrointestinal perforation and the other had hemorrhagic shock during the surgical procedure.
Drain tips were sent for culture in nine of these patients, and positive test results were seen in eight. Two yielded poly-microbial growth, and two others yielded several gram-positive cocci. In the mono-microbial cultures, the micro-organisms isolated were CoNS (two cases), and Enterococcus faecium (one), and Enterococcus faecalis (one).
No specific measures were taken in any case. Nine of 10 patients survived to completion of follow-up. The patient who did not survive was the one with hemorrhagic shock during transplantation.
Discussion
The results of this study indicate that systematic culture of abdominal drain tips provides little useful information in patients undergoing liver transplantation. First, there were no differences in the incidence of post-operative infection between recipients with positive or negative drain tip cultures. Second, the micro-organisms recovered in drain tip culture were consistent with the isolates in cultures used to confirm a post-operative infection in only one case of 94 (1.06%) liver recipients studied. The presence of abdominal drains can favor ascending colonization by cutaneous microbiota and subsequent intra-abdominal infection. Thus, the S. aureus peritonitis may have developed by this mechanism.
The other patient with S. aureus isolated on drain tip culture ultimately received a diagnosis of catheter-related sepsis from S. aureus. Because this micro-organism is a common component of the skin microbiota, we believe that the catheter infection was not related to positive culture of the drain tip; that is, the two positive cultures were likely two independent events secondary to S. aureus skin colonization. Thus, in this case, the result of drain tip culture could be considered as a confounder, and the only recipient with consistent cultures would be the one with S. aureus peritonitis.
Concerning the impact of drain tip culture on the recipient's clinical treatment and survival, none of the patients had severe complications because of post-operative infection, and all survived up to completion of follow-up.
The incidence of positive drain tip cultures was quite high in our patients (83%), but in most cases, poly-microbial growth consistent with skin microbiota was obtained. In light of the overall incidence of early post-operative infections and the impact on survival, initiation of antibiotic treatment in all cases does not seem appropriate. Further, starting generalized antibiotic agents could lead to undesirable side effects and bring on post-antibiotic infections or future infections caused by multi-drug–resistant bacteria. In our study, the single case in which P. aeruginosa was isolated on drain tip culture and the patient had an intra-abdominal abscess was likely the only post-operative infection where routine drain tip culture truly could have been useful and decisive.
The usefulness of routine drain use in abdominal surgical procedures and the associated adverse effects has been discussed widely over the past decades. In 1993, Belghiti et al. [12] conducted a randomized trial including patients undergoing elective hepatic resection. They were allocated randomly to drainage and non-drainage groups. Patients who received drains had significantly higher rates of subphrenic collections (detected by routine ultrasonography) and post-operative fever. Cultures of these collections, with samples obtained by percutaneous aspiration, were more often positive in the drainage group, although the differences were not significant. In light of the bacteria isolated from the subphrenic collections (mainly gram-positive cocci) and the high rate of fever with no micro-biologic isolation, the authors suggested an ascending origin. Routine culture after drain removal was not performed, however.
More recently, several studies have discussed the usefulness of routine use of abdominal drains in liver transplantation [13–15], and the Cochrane Library published a systematic review on this subject in 2011 [8]. No randomized trials in this line were identified, so ultimately, only three non-randomized studies were included. The authors concluded that the available evidence did not suffice to decide whether routine abdominal drainage is useful or harmful in patients undergoing orthotopic liver transplantation.
To our knowledge, there are few well-designed studies investigating the relationship between asymptomatic positive drain tip cultures and the development of infections in the immediate post-transplant period, including an analysis of associated morbidity and death, nor has the utility of routine drain tip culture been evaluated in patients with no signs of complications.
One study has reported the incidence of positive bacterial smear of the drainage site [15]. As in our study, the rate was high (60.3%), but an infection necessitating antibiotic treatment developed in only 3.4% of patients with positive smears. The remaining positive smears ere considered to be contaminated.
Other studies have described the changes in ascitic fluid during the immediate post-operative course and intra-abdominal infections occurring in pediatric population [16,17]. In one study, Sanada et al. [16] found a high incidence of positive drain tip cultures (50%) in patients with split and reduced-liver grafts. Nonetheless, the incidence of post-operative intra-abdominal infection was 24.4%. As was seen in our study, patients with intra-abdominal infections did not have a significantly higher rate of positive prophylactic drain tip culture than those without infections (63.6% vs. 45.6%, p = 0.22).
Our study had some limitations, the most important being its retrospective design, which prevented collection of some data regarding drain tip culture. In addition, molecular analyses were not performed to confirm that the micro-organisms isolated in drain tip and cultures of infection were truly the same. The large sample of consecutive liver transplant recipients, in whom treatment related to the surgical technique, immunosuppression, and complications was homogeneous, is a strength of the study, because potential confounding factors are limited.
Conclusion
The results of this study indicate that routine drain tip culture in uncomplicated or asymptomatic liver recipients is not helpful for treating these patients. In addition, this practice could be a consumption of both economic and health resources. It may be more reasonable to perform drain tip culture only in patients with a suspicion of complications after transplantation.
Footnotes
Acknowledgments
The authors thank Celine Cavallo for English language support.
Funding Information
No grants or financial support have been received for this work
Author Disclosure Statement
No competing financial interests exist.