
Abstract
Background:
Although surgical stabilization for rib fractures (SSRF) has been adopted widely over the past decade, little information is available regarding the prevalence and outcomes of post-operative surgical site infection (SSI). We hypothesized that SSI after SSRF is uncommon but morbid.
Patients and Methods:
Patients undergoing SSRF at a level 1 trauma center from 2010–2020 were reviewed. The primary outcome was the prevalence of SSI, documented by clinical examination, radiography, systemic markers of infection, and microbiology.
Results:
Of 228 patients undergoing SSRF, 167 (73.2%) were male, the median age was 53 years (P25–P75; 41–63 years), injury severity score (ISS) was 19 (P25–P75, 13–26), with a median of eight fractured ribs (P25–P75, 6–11). All stabilization plates were titanium. SSRF was typically performed on post-injury day one (P25–P75, 0–2 days) after trauma. All patients received antibiotic agents within 30 minutes of incision, and a median of four ribs (P25–P75, 3–6) were repaired. Four (1.8%) patients developed an SSI and all underwent implant removal. Two patients required implant removal within 30 days (on post-operative day seven and 17) and two for chronic infection at seven and 17 months after SSRF. The causative organism was methicillin-sensitive Staphylococcus aureus (MSSA) bacteria in all patients. After implant removal, three patients received intravenous and oral antibiotic agents, ranging from two to six weeks, without recurrent infection. No patient required additional SSRF.
Conclusions:
Surgical site infection after SSRF is rare but morbid and can become symptomatic within one week to 17 months. Implant removal results in complete recovery.
Rib fractures are present in 10% of patients admitted after trauma and are the most common bony injury resulting from blunt thoracic trauma [1–4]. The use of surgical stabilization of rib fractures (SSRF) has increased for a broadening variety of indications [5,6]. Currently, a flail chest is the most common reason to perform SSRF, but failure of non-operative management or multiple severely dislocated rib fractures have also become accepted indications [7–11]. A possible complication after SSRF is a surgical site infection (SSI). The occurrence of SSI after SSRF has been described with a pooled incidence of 1%–2%, but little information is available regarding treatment and outcome of this complication [12]. Two case series have described acute implant infections (<30 days) after SSRF and demonstrated antibiotic beads to be a viable strategy, but no studies have addressed chronic SSI or the effect of implant removal in the presence of SSI [13,14]. This study aimed to describe prevalence, treatment, and outcomes in patients with both acute and chronic SSI after SSRF in a single level 1 trauma center over a 10-year time period. We hypothesized that SSI after SSRF is uncommon, but can present in the acute or chronic setting and is morbid, requiring a multimodal treatment approach.
Patients and Methods
Design and participants
A retrospective review of a prospectively maintained SSRF database at an American College of Surgeon-certified level 1 trauma center was performed. Patients who underwent SSRF between January 1, 2010 and December 31, 2020 were included. Institutional Review Board approval was obtained.
Management of SSRF
The practice of SSRF was implemented in 2010 and indications include a radiographic (two or more consecutive ribs fractured in two or more locations) flail segment or clinical flail chest (paradoxical breathing), three or more ipsilateral, severely displaced rib fractures with no cortical contact between fracture ends and either a Sequential Clinical Assessment of Respiratory Function (SCARF) score of two or more after optimal pain control or respiratory failure caused by chest wall injury [15], 30% or more volume loss of a hemithorax, as quantified on chest computed tomography (CT), and chronic pain or a clicking sensation caused by radiographic rib fracture non-union. All fractures of ribs three to 10, with at least 3 cm from the vertebral column, are considered amenable for SSRF.
Peri-operative procedures have been standardized and include general anesthesia, intravenous antibiotic administration (2 g of cefazolin or vancomycin), fiberoptic bronchoscopy, muscle-sparring incisions, video-assisted thoracoscopic surgery (VATS) inspection of the thorax, evacuation of retained hemothorax, pleural irrigation, and chest tube placement (at the level of the sixth intercostal space, regardless of proximity to the implant or surgical incision). If a chest tube has already been placed in the pre-hospital setting or emergency department, it is removed and replaced intra-operatively. Post-operatively, all patients receive pulmonary toilet regimens by respiratory therapists and receive locoregional pain control as well as scheduled acetaminophen, ibuprofen, gabapentin, oxycodone, or intravenous narcotics or diazepam as needed. Follow-up includes outpatient visits at four, eight, and 12 weeks post-operatively with inspection of the wound, as well as chest radiography.
Data collection and outcome
Data were collected from the SSRF database with supplementation from the patient's electronic medical file. The primary outcome measure was occurrence of SSI after SSRF, documented by clinical examination (e.g., erythema, induration, or purulent drainage) or radiography (e.g., irregular bone mineralization with lucency or gas formation around the implant on chest CT) as well as systemic markers of infection (i.e., white blood cell count and C-reactive protein). Infections were confirmed by microbiology as well as operative findings.
Baseline characteristics were age, gender, race, insurance, body mass index (BMI, kg/m2), and chronic obstructive pulmonary disease (COPD) or asthma. For patients with an SSI, additional baseline characteristics included alcohol or drug use disorder, hypertension, diabetes mellitus, peripheral vascular disease, chronic liver or renal disease, congestive heart failure, active or disseminated cancer, bleeding disorder, or steroid use. In addition, injury characteristics and treatment variables of the initial admission were collected for the entire study cohort. For patients with an SSI, collected SSI variables were time from initial SSRF to operative SSI treatment (post-operative days), clinical, systemic, or radiographic symptoms at time of presentation with SSI, SSI treatment characteristics, number of re-admissions, emergency department and outpatient visits attributable to SSI before and after SSI treatment, and number of follow-up visits.
Statistical analysis
Data were analyzed using the SPSS Statistics, version 25.0 (IBM Corp, Armonk, NY). Normality of continuous variables was tested with the Shapiro-Wilk test, and homogeneity of variances was tested using the Levene test. Descriptive analysis was performed to report data for the entire study population and patients with SSI. Continuous data were reported as median and percentiles, categorical data as numbers and frequencies.
Results
Within the study period, 4,728 patients were admitted with rib fractures of whom 228 (4.8%) underwent SSRF (Table 1). In total, 167 (73.2%) were male, the median BMI was 26.3 kg/m2 (P25–P75, 23.0–30.0), and age was 53 years (P25–P75, 41–63 years). Patients had a median injury severity score (ISS) of 19 (P25–P75, 13–26) and eight fractured ribs (P25–P75, 6–11). Patients underwent SSRF at a median of one day (P25–P75, 0–2 days) after injury and all patients received antibiotic agents within 30 minutes before incision. The median operative time was 143 minutes (P25–P75, 112–187 minutes) during which a median of four ribs (P25–P75, 3–6) were fixated with five plates (P25–P75, 4–6). The median hospital length of stay (LOS) was 10 days (P25–P75, 6–16 days) and intensive care unit length of stay (ICU-LOS) four days (P25–P75, 2–8 days). Four (1.8%) patients developed an SSI and underwent implant removal.
Baseline (chest) Injury, SSRF, Treatment, and In-Hospital Characteristics of Patients Who Underwent SSRF
Data are shown as median (P25–P75) or as N (%).
SSRF = surgical stabilization of rib fractures; COPD = chronic obstructive pulmonary disease; GCS = Glasgow Coma Scale; BPC-18 = blunt pulmonary contusion 18-score.
BPC-18 was available for 225 patients.
Case 1: Acute SSI
A 45-year-old male was admitted after a motor vehicle versus pedestrian collision with a history of alcohol and drug (i.e., amphetamine) use disorder as well as COPD and a bipolar disorder (Table 2). His ISS was 17 and he was hemodynamically stable upon arrival with a Glasgow Coma Scale (GCS) of 15. Chest CT showed 15 fractured ribs with 20 fractures. The concurrent hemopneumothorax did not require a chest tube. On hospital day two, at 37 hours after admission, the patient underwent SSRF with a unilateral longitudinal lateral incision during which eight ribs with 10 fractures on the right were plated with an operative time of 258 minutes. His hospital LOS and ICU-LOS were three and two days, respectively, without mechanical ventilation requirement. The patient was discharged to an acute rehabilitation facility.
Baseline, Injury, and Treatment Characteristics of Patients Who Developed an SSI after SSRF
SSI = surgical site infection; SSRF = surgical stabilization of rib fractures; BMI = body mass index; COPD = chronic obstructive pulmonary disease; BPC-18 = blunt pulmonary contusion 18-score; ISS = injury severity score; GCS = Glasgow Coma Scale; POD = post-operative day; MSSA, methicillin sensitive Staphylococcus aureus; I&D = incision and drainage.
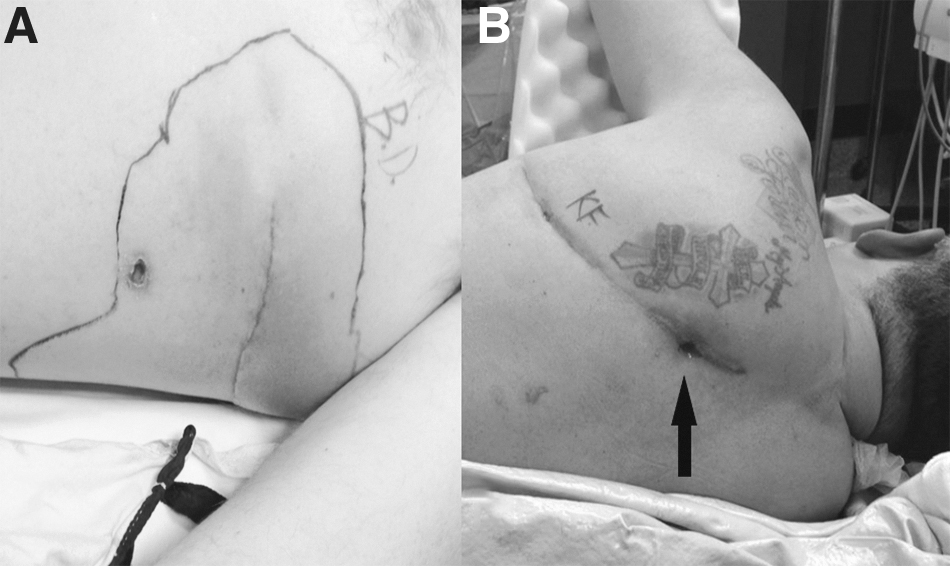
On post-operative day 16, the patient presented to the emergency department and complained of surgical site redness and swelling in combination with malaise (Fig. 1A). On chest CT, a submuscular fluid collection adjacent to the implant and loculated pleural effusion, characteristic of empyema was seen. The following day, on day 17 after initial SSRF, the patient underwent complete implant removal. Intra-operatively, purulent drainage was seen with no signs of osteomyelitis, and intra-thoracic exposure allowed for empyema wash-out. Cultures of the surrounding tissues grew methicillin-susceptive Staphylococcus aureus (MSSA). Post-operatively, he received intravenous antibiotic agents during his hospitalization and oral antibiotic agents up to six weeks after implant removal. His hospital LOS and ICU-LOS were 10 and two days, respectively. After discharge home, patient was seen two more times at the outpatient clinic for regular follow-up and showed good recovery. No emergency department visit or hospital admission was required.
Acute SSI (
Case 2: Acute SSI
A 56-year-old male was admitted after a motorcycle collision with a history of alcohol use disorder as well as COPD and chronic liver disease (Table 2). His ISS was 21 and he was hemodynamically stable upon arrival with a GCS of 15. The radiologic work-up showed a concurrent scapular fracture, and hemopneumothorax requiring a chest tube in the emergency department, without antibiotic prophylaxis. Chest CT showed eight fractured ribs with 12 fractures on the left. On hospital day two, at 38 hours after admission, the patient underwent SSRF with a longitudinal lateral incision during which four ribs with four fractures were plated with an operative time of 96 minutes. On post-operative day six, the patient became tachypneic, had clinical signs of superficial wound infection, and elevated systemic markers indicating infection. A repeat chest CT showed implant failure with two plates and screws displaced laterally, migrating into the chest wall with foci of gas and fluid along the left lateral chest wall, suspicious for a gas forming infection at the implant level (Fig. 2). On post-operative day seven, the patient underwent complete implant removal, open drainage of the left pleural space, partial excision of the comminuted fracture in rib six, and intercostal ligation of the associated intercostal bundle. Intra-operatively, frank pus in the muscular layer and deeper layers was identified with two migrated plates and purulent fluid in both the pleural space as well as in the subcutaneous tissue. Cultures were taken and showed MSSA.
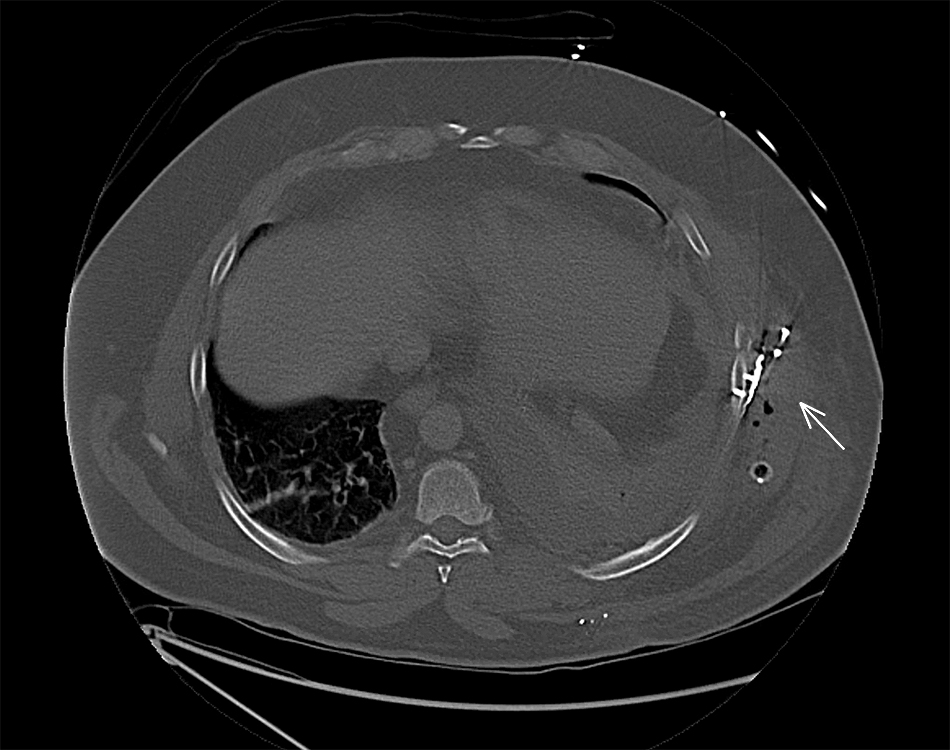
Chest computed tomography (CT) showing implant failure with plate and screw displacement, migrating into the chest wall with foci of gas and fluid along the lateral chest wall, suspicious of infection at the implant level (case 2, arrow).
Post-operatively, the patient received two weeks of intravenous antibiotic agents and four weeks of oral antibiotic agents, totaling six weeks. His hospital LOS and ICU-LOS were 24 and one days, respectively, with no mechanical ventilation requirement. Other than two regular outpatient follow-up visits, the patient underwent one additional incision and drainage of the thoracic surgical site for serosanguineous wound effusion with no signs of infection during a three-hour hospital admission at two weeks after discharge. He did not require additional antibiotic agents. A chest CT at three months after initial SSRF showed advanced healing rib fractures and scapular fracture.
Case 3: Chronic SSI
A 51-year-old male with no prior medical history was admitted after a motorcycle collision (Table 2). His ISS was 20 and he was hemodynamically stable upon arrival with a GCS of 15. Associated thoracic injuries included a clavicle and scapular fracture, and hemopneumothorax requiring chest tube placement in the emergency department, without antibiotic prophylaxis. Chest CT showed seven fractured ribs with 14 fractures on the left. On hospital day two, at 19 hours after admission, he underwent SSRF with a posterolateral approach during which four ribs with seven fractures were plated in 228 minutes. The admission was complicated by a pain catheter insertion site abscess close to the surgical site for which incision and drainage was performed, and a pulmonary embolism. The hospital LOS and ICU-LOS totaled 13 and 10 days, respectively, with no mechanical ventilation requirement.
At seven months after initial SSRF, the patient came to the outpatient clinic because of surgical site redness, warmth, and a fluctuant swelling that had spontaneously drained purulent fluid, blood, and blood clots from the initial surgical site. Cultures were taken and did not grow any bacteria. Subsequently the patient had one two-day hospital admission, two emergency department visits, and numerous outpatient visits for incision and drainage, chronic thoracic pain, negative wound pressure therapy of the SSI, and wound checks. A chest CT showed an abscess cavity, but no signs of osteomyelitis or implant failure. At 17 months after initial SSRF, the patient underwent complete implant removal without intra-thoracic exposure (Fig. 1B). Intra-operatively, two anterior sinus tracks were seen, which went up to the implant with no signs of osteomyelitis and consolidated rib fractures. Cultures were taken and grew MSSA. Post-operatively, the patient received two weeks of antibiotic agents. His hospital LOS was five days without ICU admission. After discharge home, patient was seen three more times at the outpatient clinic for regular follow-up and did not require additional emergency department visits or hospital admission.
Case 4: Chronic SSI
An 18-year-old female was admitted after a motor vehicle versus pedestrian collision with a medical history including methicillin-resistant Staphylococcus aureus (MRSA) skin infections (Table 2). Her ISS was 19 and because of a low GCS she underwent pre-hospital intubation. The radiologic work-up showed bilateral intra-cranial hemorrhage without midline shift, and a hemopneumothorax requiring a pre-hospital chest tube, without antibiotic prophylaxis. The chest CT showed three fractured ribs with four fractures on the left. On hospital day one, at 12 hours after admission, she underwent SSRF during which one rib with one rib fracture was repaired with one plate on the inner and one on the outer rib cortex, fixated with four sternal wires in 171 minutes. Her hospital LOS and ICU-LOS were 11 and five days, respectively, with three days of mechanical ventilation and discharge to an acute rehabilitation facility.
At six months after initial SSRF, the patient presented to the outpatient clinic with complaints of intermittent wound infections that had been aspirated twice at her general practitioner's office. The patient had completed several courses of antibiotic agents and had noted that two screws had fallen out of the surgical site wound. A chest CT showed decreased soft tissue and fluid attenuation around the implant, implant failure, and irregular bone mineralization of the seventh rib with lucency along the screws, suspicious for destruction related to infection or osteomyelitis (Fig. 3). At 7.5 months after initial SSRF, the patient underwent partial implant removal of the plate fixated on the rib's outer cortex and sternal wires. The bone was inspected and partially consolidated with no signs of osteomyelitis or frank pus after which the wound was irrigated without intra-thoracic entry. Cultures were taken and grew MSSA. No antibiotic agents were prescribed and patient was discharged home the same day. The patient was seen for one regular follow-up at which time advanced healing of the surgical site was seen without signs of infection. She did not require any additional outpatient or emergency department visits or hospital admission.
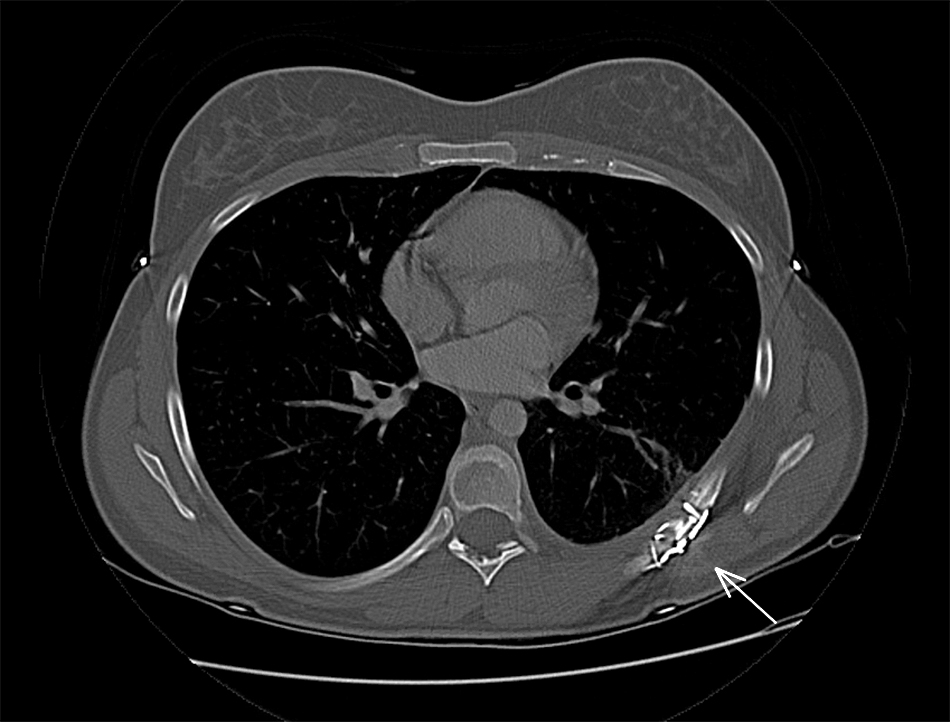
Chest computed tomography (CT) showing implant failure with screw dislodgement and irregular bone mineralization of the seventh rib with lucency along the screws, suspicious for destruction related to infection or osteomyelitis (case 4, arrow).
Discussion
Surgical site infections after SSRF are rare (1.8%) but morbid and can become symptomatic both in the acute and chronic setting. When present, multimodal invasive management centered around implant removal is required. In our experience, implant removal along with antibiotic agents was performed in all patients after which complete clinical recovery occurred without recurrent infection. All cultures of the implant grew MSSA. One patient required an incision and drainage after implant removal, but without signs of recurrent infection and no need for antibiotic agents or pain medication.
Infection at the surgical site has been associated with implant failure and shown to be the reason for removal in one third of patients requiring implant removal after SSRF [12,16]. The current study's incidence of SSI after SSRF was similar to a previous report [12]. To date, studies on surgical site or implant infection after SSRF are limited to case reports or series that only describe infection in the acute setting [13,14,17]. In the acute setting, antibiotic bead placement and vacuum-assisted closure is suggested to bridge time to union, until implant removal can be done after the rib fracture site has healed [11,13,14]. It is hypothesized that implant removal for infection before bony union leads to worse outcomes. In orthopedic long bone surgery, successful local treatment of infected non-union fractures through irrigation, debridement, and antibiotic agents alone, led to guidelines advocating treatment without implant removal [18]. A more recent study showed that only two-thirds of patients treated without implant removal or exchange achieved bony union after long bone infection [19]. In the two patients with chronic SSI site infection in our series, prolonged antibiotic agents, irrigation and debridement, and negative pressure wound therapy did not eliminate infection until implant removal.
The duration of prescribed antibiotic agents post-operatively was at the discretion of the surgeon and based on the acuity of the infection because, to our knowledge, no guidelines are available for antimicrobial treatment after implant infection after SSRF. In the cases of acute SSI, frank pus or empyema were present. Because the optimal antimicrobial treatment is not known, prolonged (6 weeks) antibiotic therapy was prescribed because of the presence of pus and pulmonary empyema [20]. In the patients with chronic SSI, intra-thoracic exposure was not performed and no pus or empyema was visible. Thus, after implant removal, antibiotic agents were prescribed for a short time frame or not at all after which the infection and chronic draining sinuses resolved. This lack of a guideline highlights the need for larger high-quality studies to develop a consensus on the treatment of this morbid complication.
In the current study, the SSI remained local with antibiotic agents and implant removal was associated with complete control of the infection without chronic chest pain or instability. In addition, the hospitalization for final implant removal was tolerated well by all patients with no in-hospital complications following this additional operative procedure, short ICU-LOS, and no post-operative mechanical ventilation requirement.
Implant infection in the acute setting should be suspected if the incision used for SSRF indicates spreading erythema, induration, skin separation, or purulent drainage [13]. In the case of chronic or late-onset infections, these complaints can still be present and warrant suspicion of infection, as are symptomatic pain at the fracture site or signs of implant failure (radiographically or clinically through visible plate displacement or even drainage of screws through the surgical site). Any recurrent signs of infection after antibiotics or failing NPWT should also raise awareness of possible implant infection.
Several limitations should be considered when interpreting these data. Although the SSRF database is collected prospectively, it is a single center study with retrospective additional data collection. This might have caused information bias through missing data. Also, patients might have presented to another hospital when experiencing complaints or possible SSI after SSRF. Second, because of the low prevalence of SSI after SSRF, the study was underpowered to determine risk factors for this complication, for example the proximity of a chest tube to the surgical incision site or implant. Furthermore, only one patient had radiographic follow-up after implant removal for SSI with short follow-up. We recommend standardized outpatient follow-up with chest CT at three or six months after implant removal to evaluate the rate of bony union and clinical recovery after implant removal for SSI.
Conclusions
Surgical site infections after SSRF are rare but morbid and can become symptomatic within one week to 17 months. An SSI is often associated with implant infection and failure. When present, implant removal might be considered because it was associated with complete recovery, both in the acute and chronic setting. With the current exponential increase in the use of SSRF, future large-scale research should be able to perform sufficiently powered studies on SSI after SSRF to determine risk factors and long-term outcomes.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Author Disclosure Statement
All authors declare no competing or personal financial interests, or any other competing interests.