
Abstract
Background:
Thoracic empyema is a disease with high mortality and morbidity. Video-assisted thoracoscopic surgery (VATS) is recommended to treat advanced stage empyema. The purpose of this study was to explore risk factors associated with post-surgery mortality for community-acquired empyema.
Patients and Methods:
We retrospectively reviewed 440 patients who received VATS for community-acquired empyema, higher than stage 2, in a tertiary medical center in Taiwan. Patients' age, comorbidities, pleural effusion analysis, and post-surgery outcome were compiled. Cox regression model for survival was applied to identify risk factors of 90-day death after surgery.
Results:
Fifty-three patients (12.05%) had died within 90 days post-surgery. The risk factors of mortality were advanced age (hazard ratio [HR], 1.027; 95% confidence interval [CI], 1.001–1.052), chronic kidney disease (HR, 5.322; 95% CI, 2.635–10.746), cancer (HR, 6.038; 95% CI, 2.737–13.321), pleural effusion pH ≤7 (HR, 2.61; 95% CI, 1.344–5.069), pleural effusion protein ≤4 (HR, 2.021; 95% CI, 1.035–3.947), and late surgery (HR, 3.014; 95% CI, 1.595–5.696). The 90-day mortality in the early surgery group versus the late group was 6.85% versus 26.05%. The increased mortality risk from late surgery was observed in most subgroups, except for patients who were female, had chronic renal disease, and had coronary artery disease.
Conclusions:
Patients who are elderly, have chronic kidney disease, cancer history, low pleural effusion pH, low pleural effusion protein, and late surgery are associated with post-surgery mortality for community-acquired advanced empyema. Early VATS surgery for advanced empyema or treatment failure of chest tube drainage appears to beneficial and is recommended.
The incidence of pleural space infection is increasing globally [1]. In the United States, comparison of the rates between 1996 and 2008 showed that the hospitalization rates of parapneumonic empyema were increased two-fold [2]. Empyema leads to a prolonged hospital stay, high fatality, disability, and economic burden. The reported 30-day mortality rates ranged from 10% to 20% [3–5]. Thoracic empyema progresses in three stages: exudative (simple parapneumonic), in which exudative fluid accumulates without loculation; fibrinopurulent (complicated parapneumonic), in which pleural fluid becomes turbid or purulent with loculation; and organizing (empyema), in which thickened pus or fibrin peels begin to form, and granulation tissue replacement of the pleural space occurs [6]. The mortality rate and length of hospital stay increase with stage progression. Renal insufficiency, age (elderly), purulence of the pleural fluid, nosocomial infection source, and dietary factors, known as the RAPID score, predicted poor clinical outcomes [7]. Diabetes mellitus, chronic obstructive pulmonary disease, body mass index, pathogens (Klebsiella pneumoniae, tuberculosis, fungal infection), and different intervention maneuvers (conservative chest tube drainage, fibrinolysis, and surgical decortication) were reported to affect the survival of empyema [8–12]. According to the RAPID score for empyema, nosocomial pleural infection leads to higher mortality than community-acquired infection.
Previous studies seldom divided infection into nosocomial and community-acquired groups. Chest tube drainage was the main therapy for empyema. However, nearly one-half of patients with initial chest tube therapy needed surgical intervention [12]. The American Association for Thoracic Surgery recommended that video-assisted thoracoscopic surgery (VATS) should be the first-line approach in all patients with stage 2 acute empyema [13]. Video-assisted thoracoscopic surgical decortication offers superior clinical outcomes than open surgery in terms of decreased length of stay, less pain, and less overall morbidity [14]. Here, we documented the 10-year retrospective study to determine clinical characteristics and risk factors of mortality after video-assisted thoracoscopic surgical decortication with community-acquired advanced thoracic empyema in Taiwan.
Patients and Methods
Study participants
This retrospective study recruited patients hospitalized because of community-acquired thoracic empyema at Changhua Christian Hospital, a 1,200-bed tertiary medical center in Taiwan, from April 2005 to May 2014. The collected data contained information on patient's demographics, comorbidities, symptoms on admission, laboratory analysis of blood, serum, and pleural effusion, ventilator use, and mortality. The culture reports for pleural fluid and tissue were obtained. Empyema is diagnosed when one of the three following conditions is met: frank pus aspirated from the pleural space; positive gram stain or culture of pleural effusion or tissue; and pleural effusion pH <7.2, glucose <40 mg/dL, or lactate dehydrogenase (LDH) >1,000 U/L [15]. Surgical intervention would be recommended if the patient had poor drainage function of the chest tube, loculated pleural effusion by chest radiography or chest computed tomography (CT) image, separated pleural effusion by chest echocardiogram. The exclusion criteria included no video-assisted thoracoscopic surgical decortication; age younger than 20 years; relative to nosocomial pneumonia, malignant pleural effusion, or tuberculosis; surgery and chest wall trauma involving the pleural cavity prior to the development of pleural effusion; undergoing intervention therapy at other hospitals before hospitalization; no pleural laboratory analysis or culture. Four hundred forty patients were enrolled in the study (Supplementary Figure S1). The study protocol was approved by the Investigational Review Board of Changhua Christian Hospital (approval #200317).
Definition of community-acquired versus hospital-acquired thoracic empyema
Community-acquired or hospital-acquired thoracic empyema was defined according to the origin of infection from community-acquired or hospital-acquired pneumonia [9].
Surgical intervention
The first-line surgical procedure in the study was VATS. The secondary VATS indicated that chest surgeons performed VATS again for patients with residual loculated empyema, which limited full expansion of the lungs. Towe et al. [8] reported that if pre-operative hospitalization lasted longer than five days, the re-admission rates, major morbidity, and prolonged length of hospital stay were all higher. Here, we defined late surgery as time from admission to surgery longer than five days. Anything else was considered early surgery. Death was defined as in-hospital or 90-day mortality from the surgery.
Statistical analysis
Categorical variables were presented as a number and percentage; continuous variables were presented as the mean ± standard deviation. Continuous variables were compared between the survivor and death groups using an independent samples t-test. Categorical data were compared using the χ2 test. The most important risk factor of post-surgery 90-day mortality was identified using the Cox proportional regression model with backward elimination. The Kaplan-Meier curve was used to present the survival rate over the time between the early and late surgery groups, and the differences were compared using log-rank tests. Data were analyzed using SPSS Statistics, version 22 (IBM Corp, Armonk, NY).
Results
Patient demographics, pleural effusion microbiology, and clinical outcomes
Of 440 patients, the overall mean age was 60.61 years. Male patients (78.86%) were predominant (Table 1). More than one-half of patients did not have a history of smoking. Hypertension (39.31%) and diabetes mellitus (31.59%) were the leading comorbidities. Infective pleural disease occurred more in the right chest. The predominant initial symptoms were fever (37.27%), chest pain (37.27%), breathless (31.59%), and cough (29.77%). Table 2 shows that microbiologic diagnosis was obtained for 211 patients (47.95%). The mixed-type (15.9%) pleural infection was the most common. Streptococcus viridans (15.52%) and Klebsiella pneumoniae (10.56%) were the two leading micro-organisms (Supplementary Figure S2). The major stage of empyema was stage 2 (72.84%). The average time from admission to surgery was 4.98 days. 321 patients (72.95%) underwent VATS within five days. Only five (1.13%) patients accepted conversion thoracotomy during the first operation. Ten (2.27%) patients underwent secondary VATS. In terms of outcome, average duration of ventilator use was 9.6 days; 12.27% patients had difficulty in discontinuing ventilator with prolong mechanical ventilator use. A prolonged hospital stay (23.81 days) was recorded. The 30-day and 90-day post-operative mortality were 8.41% and 12.05%, respectively.
Demographics, Comorbidities, and Clinical Characteristics
p < 0.001.
p < 0.05.
Data are presented as the mean ± standard deviation or as the count (percentage).
CKD = chronic kidney disease; CAD = coronary artery disease; COPD = chronic obstructive pulmonary disease; GERD = gastroesophageal reflux disease.
Clinical Characteristics, Microbiologics, and Clinical Outcomes
p < 0.001.
p < 0.05.
WBC = white blood cell count; Seg = segmented neutrophils; LDH = lactate dehydrogenase; IO = intra-operative.
Mixed type: Contain at least two of the three categories, gram-positive, gram-negative, and anaerobic bacteria.
Empyema stage: Defined by chest ultrasound and chest computed tomography imaging, or by surgical findings.
Secondary VATS indicated that chest surgeon performed VATS again for patient with residual loculated empyema, which limited full lung expansion.
Prolong ventilator: continue invasive mechanical ventilation for more than 21 consecutive days over 6 hours per day.
Data are presented as the mean ± standard deviation or as the count (percentage).
Univariate analysis of 90-day mortality
Regarding demographics and comorbidities, elderly patients, former smokers, patients with diabetes mellitus, chronic kidney disease (CKD), coronary artery disease (CAD), gastroesophageal reflux disease (GERD), and history of cancer had higher mortality rates (p < 0.05; Table 1). The deceased patients had presented with lower probabilities of fever (18.86%: 39.79%, p = 0.003) and chest pain (13.2%: 40.56%; p < 0.001). Low protein concentration in pleural effusion and mixed bacterial pleural infection were associated with high mortality (Table 2). Klebsiella pneumoniae empyema had higher death rates (18.37%), however, that was not statistically significant (p = 0.149). The 90-day mortality in patients undergoing early surgery was lower than late surgery (6.85%: 26.05%; p < 0.001). The deceased patients often had prolonged mechanical ventilator use and longer hospital and intensive care unit (ICU) stays than did survivors (p < 0.001).
Multivariable Cox proportional hazard model analysis for 90-day mortality
In the initial analysis, age, CAD, CKD, cancer, lung cancer, Esophageal, stomach, intestinal cancers, low pleural effusion pH (pH ≤7), low pleural effusion protein (≤4), and late surgery were significant risk factors for 90-day mortality (Table 3). After adjustment by Cox proportional hazard model with backward elimination, elderly, CKD, cancer, low pleural effusion pH (pH ≤7), low pleural effusion protein (≤ 4), and late surgery remained as the significant risk factors. Late surgery led to high-risk of 90-day mortality compared with the early surgery group (adjusted HR, 3.014; 95% CI, 1.595–5.696). Kaplan-Meier survival analysis showed that the early surgery group had a higher survival rate than the late surgery group (log rank test, p < 0.001; Fig. 1A). In the subgroup analysis, the increased mortality risk from late surgery was observed, except for patients who were female, had CKD, and had CAD (Fig. 1B).
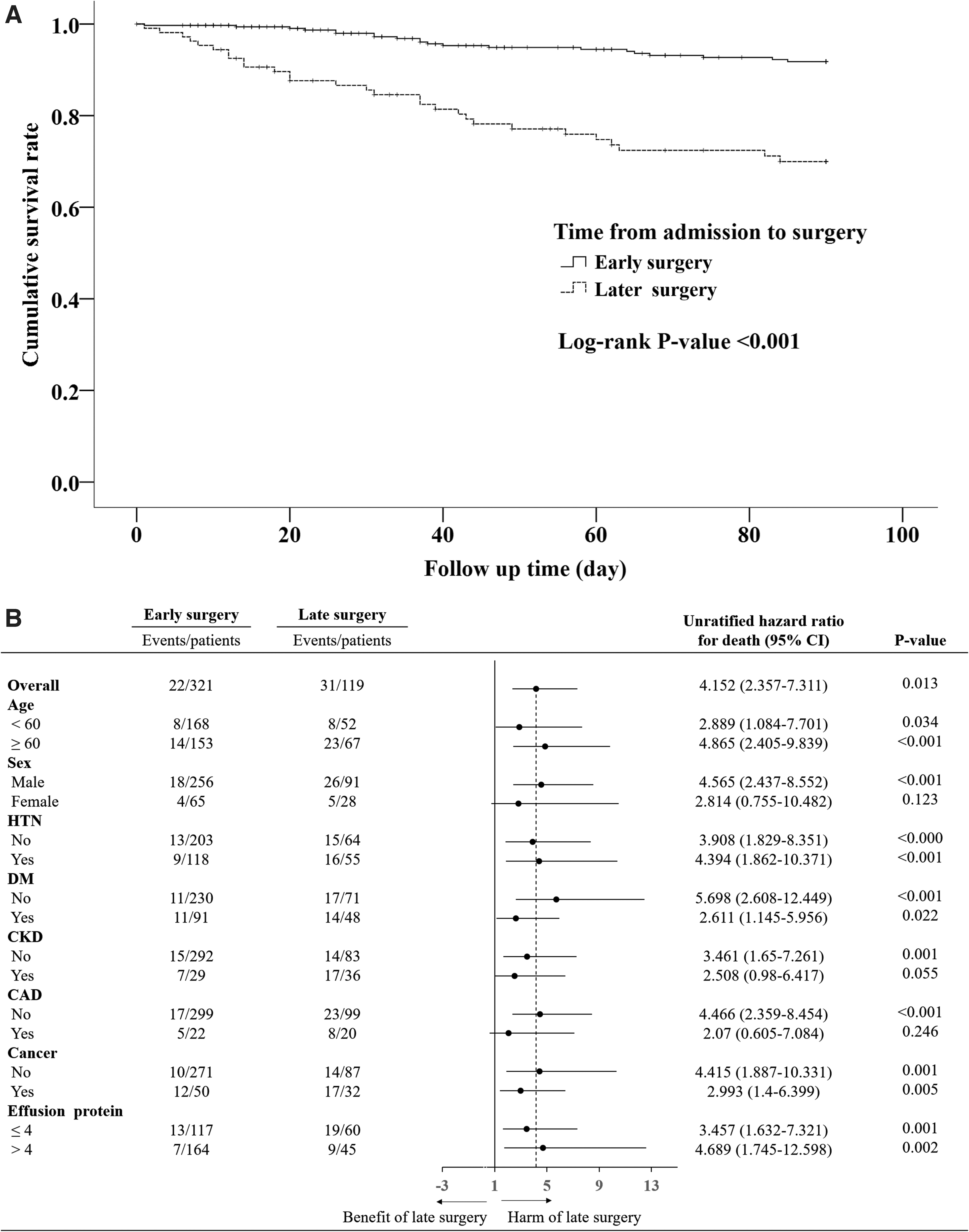
Survival curve analysis. (
Significant Risk Factors for Ninety-Day Mortality after Surgery
p < 0.05.
p < 0.001.
cHR = crude hazard ratio; CI = confidence interval; aHR = adjusted hazard ratio; CAD = coronary artery disease; CKD = chronic kidney disease.
Multivariable Cox proportional hazard model with backward elimination.
Discussion
To our knowledge, this is the first study for risk factors on surgical intervention to empyema focusing on community-acquired infection in Taiwan. Video-assisted thoracoscopic surgery to treat empyema was effective with few conversion thoracotomies (1.13%) and secondary VATS (2.27%). However, empyema still resulted in high mortality within 90 days after surgery (12.05%), prolonged mechanical ventilator use (12.27%), and prolonged length of hospital stay (23.81 days) in our study. Six clinical factors (elderly, CKD, history of cancer, low pleural effusion pH, low pleural effusion protein, and late surgery) were associated with the post-surgery outcome. Benefits of early surgery were observed in most subgroups, except for patients who were female, had CKD and CAD.
In univariate analysis, mixed pleural bacterial infection led to higher mortality rate (18.37%). Viridans streptococcus was the most common bacterial strain, causing pleural infection, whereas Klebsiella pneumoniae was the second predominant strain. The result differs slightly from that of two previous studies [11,16] and are the same as those of Chen et al. [17] in Taiwan. This difference may be related to the fact that our patients were mainly recruited from community-acquired infection and to the different areas in Taiwan.
Viridans streptococcus infection is associated with poor oral hygiene and aspiration. The recruited patients in our study were elderly (61 years old) and had more comorbidities (average 1.3 comorbidities per person). These factors would contribute to Viridans streptococcus infection. Klebsiella pneumonia infection has a strong correlation with diabetes mellitus. High prevalence of diabetes mellitus in empyema has been observed in Taiwan (22%–27%) and in our study (31.59%), and it would cause a high incidence of Klebsiella pneumoniae infection. The pathogen analysis is different from that of other countries [4,10,18]. Nine patients (18.37%) with Klebsiella pneumoniae infection died during the 90-day post-surgery observation. High mortality of Klebsiella pneumoniae empyema in Taiwan had been published previously [11], as noted in our study, however, the result did not reach statistical significance. This might be because of the small sample size of Klebsiella pneumoniae empyema.
In Table 2, only 42 (9.54%) patients accepted chest tube drainage before operation. The result might be caused by one of the inclusion criteria, namely, VATS intervention for empyema. This selection would exclude stage 1 empyema. In stage 1 empyema, chest tube intervention was suggested and effective to treat empyema. According to Semenkovich et al. [12], the failure rate of chest tube drainage for empyema was close to 50%. Surgery with VATS decortication for complicated empyema was convenient and could be performed quickly in our hospital. These factors contributed to the low rate of chest tube intervention before operation in this study. In the initial crude Cox proportional hazard mode, the hazard ratio of chest tube intervention was 1.476 (95% CI, 0.664–3.282; p = 0.339). The association of the initial chest tube intervention and 90-day mortality was not significant.
Few studies discussed the association between pleural effusion analyses and empyema prognosis. Our Cox proportional hazard analysis showed that patients with low pleural effusion pH value (pH ≤7) and protein (≤ 4 g/dL) had higher post-surgery mortality. Previous studies reported pH values in advanced stage empyema were lower than in early stages [19,20]. Advanced stage empyema would be responsible for the high post-surgical mortality and morbidity. Pleural effusion arises from the systemic pleural vessels and flows across the leaky pleural membranes into the pleural space [21]. Two main components of proteins in human serum are globulin and albumin. We found that the serum albumin level in the pleural effusion protein ≤4 and >4 groups were 1.94 ± 0.48 g/dL and 2.42 ± 0.57 g/dL (p < 0.001), respectively. According to the RAPID score for empyema, low serum albumin level is associated with poor outcome. High mortality in empyema patients with lower pleural effusion would be relative to hypoalbuminemia.
The interval from admission to surgical intervention was an important prognostic factor. It was confirmed by the Cox proportional hazard analysis to eliminate confounding factors (adjusted HR, 3.014; 95% CI, 1.595–5.696). Early surgical intervention with VATS decreased disease mortality by 19.2% (number needed to treat, 5.21). The results are similar to those of Towe et al. [8]. According to the subgroup analysis, benefits of early surgery were observed in most subgroups, except for patients who were female, had CKD, and CAD. To date, the guidelines for managing empyema focused on VATS as the first-line approach in acute empyema [13,18,22]. Prolonged surgical intervention had an impact on empyema stage migration and reduces the success of VATS [23,24]. Meanwhile, late surgical intervention, observed in our study, was also associated with higher mortality and needs further attention from clinicians and surgeons.
As in previous reports, cancer worsened a patient's immunity and nutritional status, causing a high mortality rate when patients developed empyema. Being elderly and having CKD made patients more vulnerable, made management of empyema difficult, and resulted in more complications. Compared with previous research, our empyema mortality rate was high (Table 4). The 30-day death rate after VATS surgery was the lowest (2.8%) in the study by Towe et al. [8], which excluded patients with a history of cancer and recruited relatively younger patients (mean age, 55 years old). Reichert et al. [25] recruited patients with pure stage 3 empyema and higher cancer morbidity (11%). The intra-operative blood loss during VATS was higher (511 mL) than in our study (179 mL), which would be the reasons for high 30-day mortality rate (9.5%). The risk factors findings were compatible with our results.
Mortality and Pre-Operative Predictors of Outcome in Series of Empyema Patients Treated by Chest Tube Drainage or Surgery
VATS = video-assisted thoracoscopic surgery; BMI = body mass index; COPD = chronic obstructive pulmonary disease; ASA = American Society of Anesthesiologists; CKD = chronic kidney disease; CRP = C-reactive protein.
There were several limitations in this retrospective study. First, patients accepted surgical intervention maybe selected by initial surgeon's evaluation. The results may not include empyema cases with severe sepsis. Second, microbiologics were obtained only by general bacterial pleural effusion culture. Advanced molecular method was not applied to explore the accuracy of pathogen distribution. Larger prospective studies are needed to verify our results.
Conclusions
Community-acquired complicated empyema is a disease with high morbidity and mortality. Six clinical factors (age, CKD, history of cancer, low pleural effusion pH, effusion protein, and late surgery) affected the post-surgery outcome. Early surgical intervention with VATS would reduce risk of patient mortality by approximately 20%. The optimal timing of surgical intervention has not been determined. Further prospective investigation is needed.
Footnotes
Acknowledgments
The authors would like to thank Peter Chen for assistance with the English language translation.
This article does not contain any studies with animals performed by any of the authors. The study protocol was approved by the Investigational Review Board of Changhua Christian Hospital (approval no: 200317)
Authors' Contributions
C.W.L., S.H.L., M.H.H., K.Y.H., C.H.L., B.T.W., and C.T.K. designed the study together. C.W.L. was the lead author who organized the study. S.H.L. and M.H.H. were co-authors and helped coordinate the progress of the study. K.Y.H. and C.H.L. provided input into our database. B.T.W. was the main chest surgeon to provide technological assistance. C.T.K. provided the statistical analysis. All authors reviewed the manuscript.
Funding Information
This study was supported by Changhua Christian Hospital, Taiwan. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. No additional external funding received for this study.
Author Disclosure Statement
No conflicts exist for the authors and no funding was received.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.