
Abstract
Background:
Ampicillin-sulbactam is a piperacillin-tazobactam–sparing alternative antibiotic administered as surgical prophylaxis during orthotopic liver transplant (OLT), but limited data are available describing its pharmacokinetics and impact of blood product resuscitation. The purpose of this study was to determine the intra-operative pharmacokinetics of ampicillin-sulbactam in patients during OLT and evaluate the effects of blood resuscitation on exposure.
Patients and Methods:
This was a pharmacokinetic study in 10 OLT patients receiving ampicillin-sulbactam surgical prophylaxis. A 5,000-patient Monte Carlo simulation was conducted to identify optimal ampicillin-sulbactam regimens. Linear regression assessed association between blood product administration and ampicillin exposures.
Results:
Ampicillin and sulbactam concentrations best fitted two-compartment models. Mean ampicillin pharmacokinetic parameters were central compartment volume (Vc): 6.9 ± 2.0 L, clearance (CL): 26.6 ± 18.4 L/h, and inter-compartmental rate constants (k12 and k21): 4.8 ± 2.6 and 2.3 ± 1.4 h−1. Sulbactam pharmacokinetic parameters were Vc: 8.1 ± 2.7 L, CL: 26.1 ± 7.4 L/h, k12 and k21: 4.9 ± 1.0 and 2.8 ± 1.1 h−1. Participants received between 500 and 23,642 mL of total blood product. No statistical relations were observed between blood product administration and exposures (R2 0.00–0.26). Ampicillin-sulbactam 2/1 g every two hours and 2/1 g bolus followed by 6/3 g continuous infusion provided acceptable probability of target attainment up to minimum inhibitory concentrations (MICs) of 16 and 32 mcg/mL, respectively.
Conclusions:
High and frequent ampicillin-sulbactam doses are required to maintain 100% fT > MIC at relevant MICs during OLT and no impact of blood product resuscitation was observed on ampicillin exposure. These are the first data available to guide ampicillin-sulbactam dosing in patients undergoing OLT.
Orthotopic liver transplantation (OLT) remains a life-saving treatment for many patients suffering from end-stage liver disease secondary hepatic failure or hepatocellular carcinoma [1]. Important advancements in surgical technique and supportive post-operative care since the first successful transplantation nearly 60 years ago allow patients to live long and relatively morbid-free lives [2,3]. Despite these advancements, transplant recipients are most vulnerable 30 days post-transplant because of the risk of surgical-related infection [4–6]. Surgical prophylaxis with intravenous antibiotic agents immediately prior to and during OLT is recommended to prevent surgical-related infection [7]. However, even with antimicrobial prophylaxis, infection rates post-transplant can vary from 8.8% to 43% [4–6,8–10]. There are many factors that make OLT patients susceptible to infection: the extensive surgical trauma, which disrupts natural protective barriers; the potent immunosuppressive regimens utilized, which deplete defense mechanisms; and the hemodynamic and metabolic instability during and immediately after the procedure, which inhibit regenerative and protective capacity. Multivariable analyses have identified duration of surgery, number of red blood cell transfusions, duct-to-duct anastomosis/bile leak, pre-operative dialysis needs, and immunosuppression as independent risk factors for deep organ/space and surgical site infection [8,10,11].
Although practice guidelines for prophylaxis in OLT have been published, the supportive evidence for choice of agent is weak relative to other types of surgery [7,12,13]. As a result, selection of antibiotic prophylaxis is most often decided by local practice/epidemiology based on recipient, donor, and surgical risk factors [13]. A number of recent reports have also identified multi-drug–resistant bacteria (i.e., bacteria not covered by the prophylactic antibiotic) as a common cause of infection [10,11]. Ampicillin-sulbactam, a broad-spectrum antibiotic that covers most gram-negative Enterobacterales, gram-positives including Enterococcus spp., and anaerobes, is an alternative antibiotic to piperacillin-tazobactam or ampicillin plus a third-generation cephalosporin for surgical prophylaxis of OLTs [12,13]. To our knowledge all studies exploring ampicillin, with or without sulbactam, as surgical prophylaxis for OLT have used a regimen administered every six hours [14–16]. This is despite guidelines recommending a two-hour dosing interval [7,13]. Furthermore, no pharmacokinetic studies in OLT have been conducted evaluating both ampicillin and sulbactam when administered together.
During OLT there are several interventions that theoretically could alter ampicillin and sulbactam pharmacokinetics. In particular, the potential for large volume blood loss accompanied by massive blood transfusions could hypothetically lower antibiotic concentrations below prophylaxis thresholds [17]. Unfortunately, the effects of blood loss and transfusion on the pharmacokinetics of antibiotics are largely unknown. Because the efficacy of antibiotic prophylaxis is directly related to maintaining therapeutic concentrations throughout surgery, it is paramount to understand how blood loss and transfusion affect their pharmacokinetics and whether early re-dosing is required to maintain concentrations above the minimum inhibitory concentration (MIC). Herein, we sought to characterize the intra-operative pharmacokinetics of ampicillin and sulbactam in OLT patients and assess the impact of blood transfusion on ampicillin exposure.
Patients and Methods
Study design and participants
This was a single-center observational pharmacokinetic study conducted at Harford Hospital (Hartford, CT). The study protocol was reviewed and approved by the Institutional Review Board and all study participants were required to provide written informed consent. Eligible participants included adults ≥18 years of age who were called in to the hospital for an OLT, and who were anticipated to receive surgical prophylaxis with ampicillin-sulbactam. Patients were excluded if they required a simultaneous liver and kidney transplant, had a creatinine clearance (CrCl) ≤30 mL/min (calculated by the Cockcroft-Gault equation) at time of enrollment, required continuous renal replacement therapy or intermittent hemodialysis, or were participating in any other interventional drug study within 30 days of the current study. Participants were followed for 30 days after OLT to determine occurrence of any post-operative infection.
Antibiotic administration and blood sampling
Ampicillin-sulbactam is the first-choice antibiotic for surgical prophylaxis in patients undergoing OLT at Harford Hospital. During this study, ampicillin-sulbactam dosing was prescribed at the discretion of the anesthesiologist on duty. Ampicillin-sulbactam is also routinely administered post-operatively for four to six days at a treatment dosage of 2/1 g every six hours, or dose adjusted for renal dysfunction. Participants had up to 24 intra-operative blood samples collected throughout the study, with three to five samples collected within each dosing interval. After collection of a 10-mL discard, whole blood samples were drawn from a central line in 4 mL ethylenediaminetetraacetic acid (EDTA) tubes and centrifuged at 2,000g for 15 minutes at 10°C to separate the plasma. Plasma was divided into cryovials and then immediately frozen at −80°C. Protein binding was measured in triplicate at the estimated peak concentration of the first dose. After separation, plasma was transferred to an ultrafiltration device (Centrifree®, Merck Millipore Ltd., Ireland), centrifuged at 2,000g for 45 minutes at 10°C, and then frozen at −80° C. Recorded administration of blood products (packed red blood cells [PRBC], fresh frozen plasma [FFP], platelets, cryoprecipitate, cell salvage [autologous] blood, and albumin) were collected from the anesthesia and perfusionist reports.
Analytical procedures
Concentrations of both ampicillin and sulbactam in plasma were determined using a validated high-performance liquid chromatography assay [18]. Analytical ranges for ampicillin and sulbactam were 1–50 mcg/mL and 0.5–50 mcg/mL, respectively. Mean inter-day coefficients of variance (CV) for low and high values of ampicillin in plasma were 5.44% and 2.42%. For sulbactam, these values were 3.53% and 3.45%, respectively. To assess ampicillin and sulbactam-free drug concentrations, the assay was modified slightly using a saline standard curve with the same concentration ranges. Inter-day CV for low and high check samples were 2.15% and 0.94% for ampicillin, respectively, and 3.48% and 6.50% for sulbactam.
Pharmacokinetic analyses
Ampicillin and sulbactam concentrations were fitted separately to one- or two-compartment models using the non-parametric adaptive grid algorithm (NPAG) in the Pmetrics package (Laboratory of Applied Pharmacokinetics, Los Angeles, CA) for R (version 4.0.3) [19]. Final model selection was determined by the Akaike information criterion (AIC) value, visual inspection of the observed versus predicted plots, and evaluation of pharmacokinetic parameter estimates for each participant. For each fit, a multiplicative error model was used whereby error = SD * γ, where SD is the equation of the regression line of best fit for the standard deviation versus observed concentrations from the ampicillin (0.5, 0.15) or sulbactam assay (0.25,0.15) and γ represents environmental noise as determined by the NPAG algorithm. After selection of a base model, linear regression (SigmaPlot Version 14, Systat Software, San Jose, CA) was applied to determine relationships between several patient covariates including body weight (WT), CrCl, as well as total units received of PRBC, FFP, platelets, cryoprecipitate, and albumin.
Monte Carlo simulation
Monte Carlo simulation was conducted for the ampicillin component of ampicillin-sulbactam in Pmetrics. The population pharmacokinetic estimates from the final model were recapitulated in 5,000 simulated patients receiving the following doses of ampicillin-sulbactam: 2/1 g as a 0.5 hour intravenous infusion every six hours, 2/1 g intravenous push (over 1 minute) every two hours, 2/1 g every two hours as 0.5 h infusion, and a 2/1 g intravenous push loading dose followed immediately by 6/3 g as a continuous infusion.
Ampicillin concentrations were simulated over eight hours, the approximate total time for most OLTs and then corrected for the average free fraction observed in these patients. The probability of target attainment (PTA) was calculated based on the free ampicillin concentration remaining above the MIC for 100% of the eight-hour procedure. The current Clinical Laboratory Standards Institute (CLSI) MIC susceptibility breakpoint for ampicillin-sulbactam (i.e., 8/4 mcg/mL) was used for the primary analysis [20]. However, MICs of 16/8 mcg/mL and 32/16 mcg/mL were also evaluated because these MIC values cover 81.8% and 91.5%, respectively, of the collective ampicillin-sulbactam MIC distribution for non-ESBL Escherichia coli and Klebsiella pneumoniae in the United States in 2018 [21].
Results
Patient characteristics
Thirteen participants were consented into this study from October 2019 until December 2020. Three were excluded because of cancellation of the surgery after consent was obtained, leaving 10 participants who completed the study. Baseline demographics of the 10 study participants can be found in Table 1. Participants received between 500 and 23,642 mL of total blood product. Study participants received ampicillin-sulbactam prophylaxis regimens at 1/0.5 g every two hours (n = 1), 2/1 g every three hours (n = 2), or 2/1 g every two hours (n = 7). Most doses were administered as an intravensou push over approximately one minute. All antibiotic regimens were well tolerated. One patient, who received 2/1 g every two hours as prophylaxis regimen, required antibiotic agents on post-operative day six for new onset fever and presumed biliary tract infection, but all cultures remained negative; no other infections were observed during the 30-day follow-up.
Characteristics for Ten Patients Undergoing Liver Transplantation Included in Ampicillin-Sulbactam Pharmacokinetic Analyses
SD = standard deviation; BMI = body mass index; CrCL = creatinine clearance; MELD = Model for End-Stage Liver Disease; PRBC = packed red blood cells; FFP = fresh frozen plasma.
Pharmacokinetics
A total of 118 plasma samples were collected for determination of ampicillin and sulbactam concentrations. Total ampicillin and sulbactam plasma concentrations ranged from 13–587 mcg/mL and 5–192 mcg/mL, respectively. The mean ± standard deviation protein binding in these patients was 17% ± 8% (range, 4%–30%) for ampicillin and 34% ± 13% (range, 11%–57%) for sulbactam. A two-compartment model fitted the data better than a one-compartment model for ampicillin (AIC, 1067.5 vs. 963.6) and sulbactam (AIC, 986.3 vs. 929.0). Multiple covariates, including CrCl, body weight, as well as blood product volumes, were explored using linear and allometric scaling on ampicillin clearance (CL) and volume of the central compartment (Vc). No covariate improved model fit by both AIC and visual inspection of data. Final ampicillin and sulbactam pharmacokinetic parameters are presented in Table 2. The Bayesian posterior observed versus predicted plots were acceptable for ampicillin population-predicted and individual-predicted plots (Fig. 1), as well as for sulbactam population- and individual-predicted plots (Fig. 2). γ for the final ampicillin and sulbactam models were good at 1.58 and 1.91, respectively.
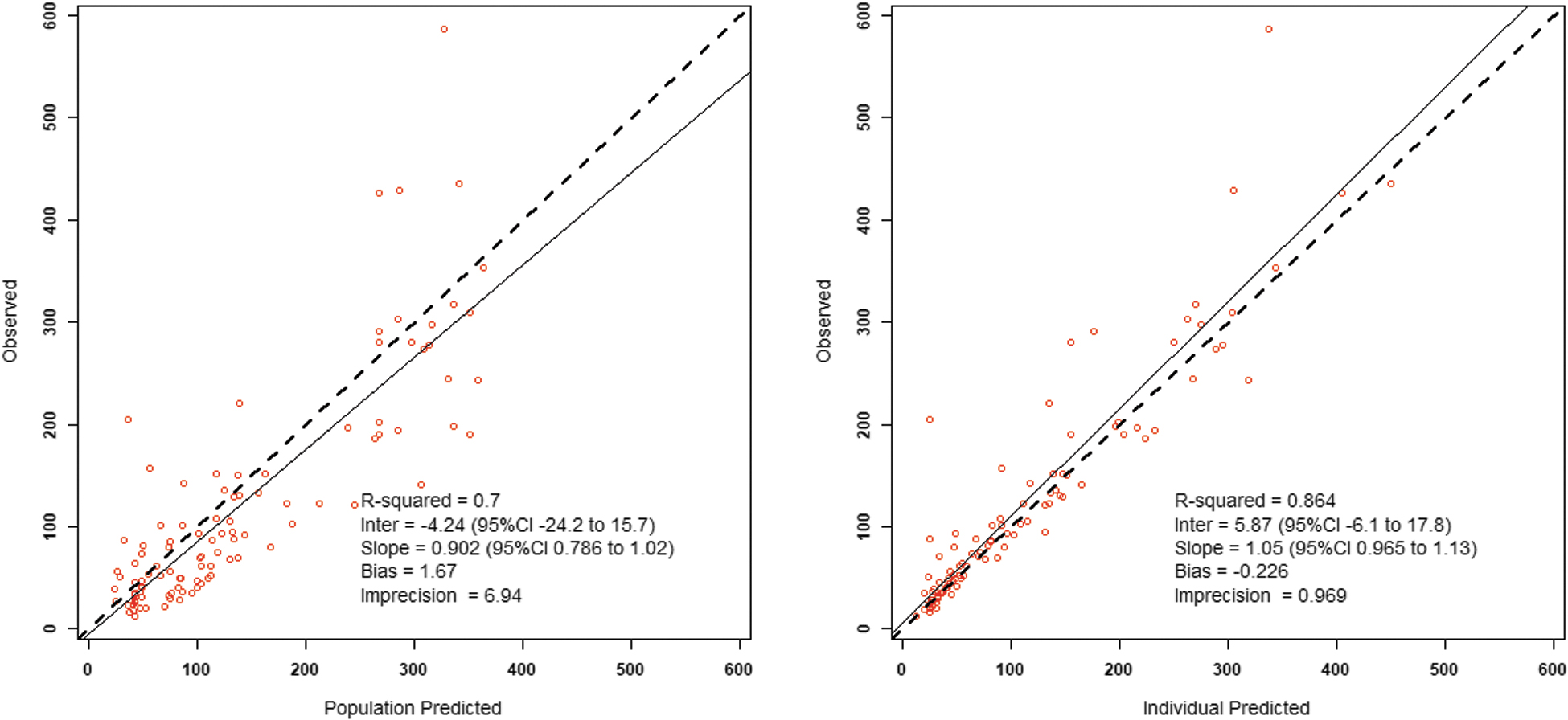
Observed versus population (left) and Bayesian individual (right) predicted concentrations for ampicillin. CI = confidence interval. Color image is available online.
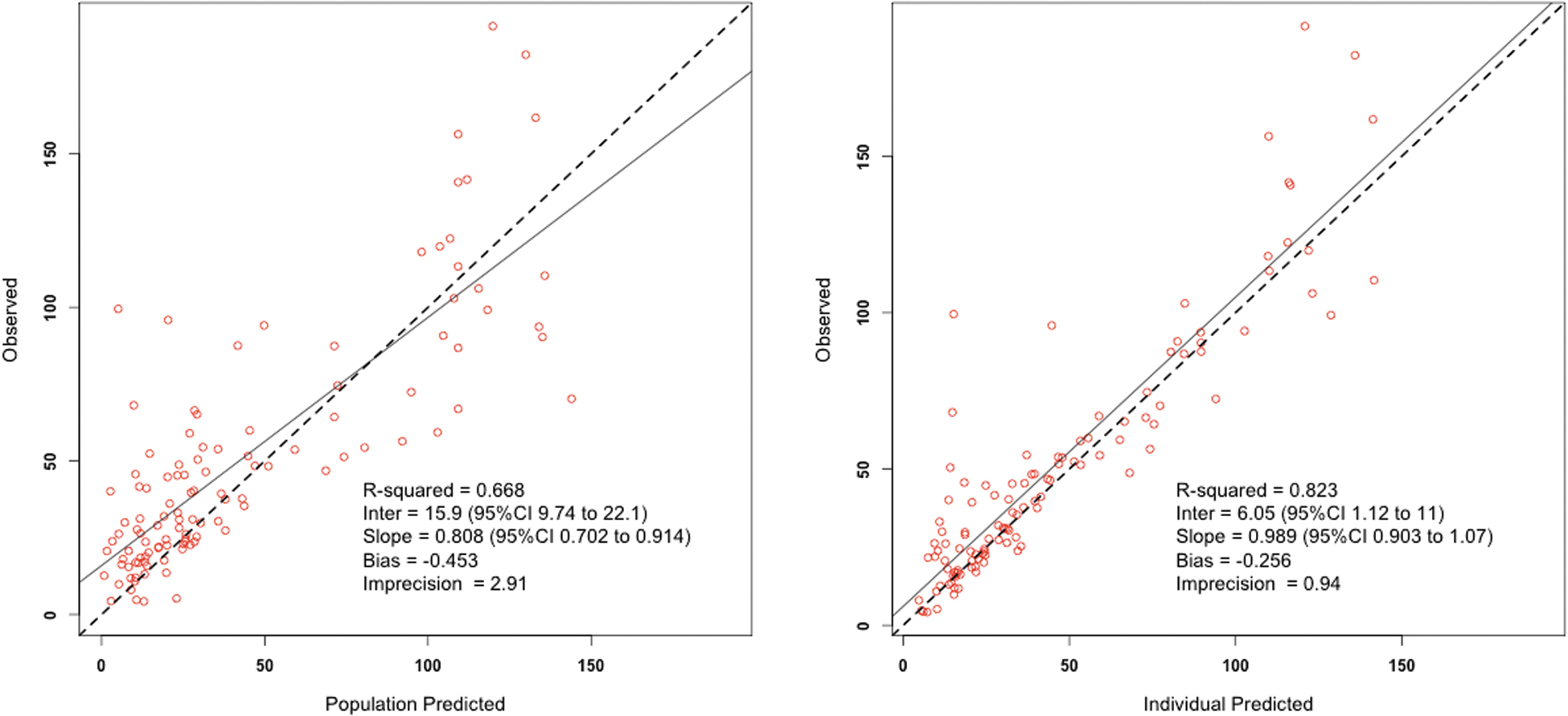
Observed versus population (left) and Bayesian individual (right) predicted concentrations for sulbactam. CI = confidence interval. Color image is available online.
Final Population Pharmacokinetic Parameter Estimates for Ampicillin and Sulbactam from Ten Patients Undergoing OLT
OLT = orthotopic liver transplant; PK = pharmacokinetic; SD = standard deviation; CL = clearance; Vc = volume of the central compartment; k12 and k21 = inter-compartmental transfer constant.
Impact of blood products on ampicillin exposure
To assess ampicillin exposure relative to blood product volumes administered, ampicillin concentrations for the three patients receiving lower doses were normalized to the 2/1 g every two hours ampicillin-sulbactam regimen (the most common regimen prescribed in these patients) by re-simulating their concentration time profile using their individual maximum a posteriori Bayesian pharmacokinetic parameter estimates. Logistic regression was performed to assess relations between blood product administration and ampicillin-free time above the MIC (fT > MIC) (referenced to 32 mcg/mL) or free area under the curve over eight hours (fAUC0-8). Coefficient of determinations and p values for each comparison are provided in Table 3. The linear regression plots for ampicillin fT > MIC32 and fAUC0-8 with units of PRBC are provided in Figure 3. All other linear regression plots for the comparisons are provided in Supplementary Figures S1 to S5 because no significant relations with exposure were identified.
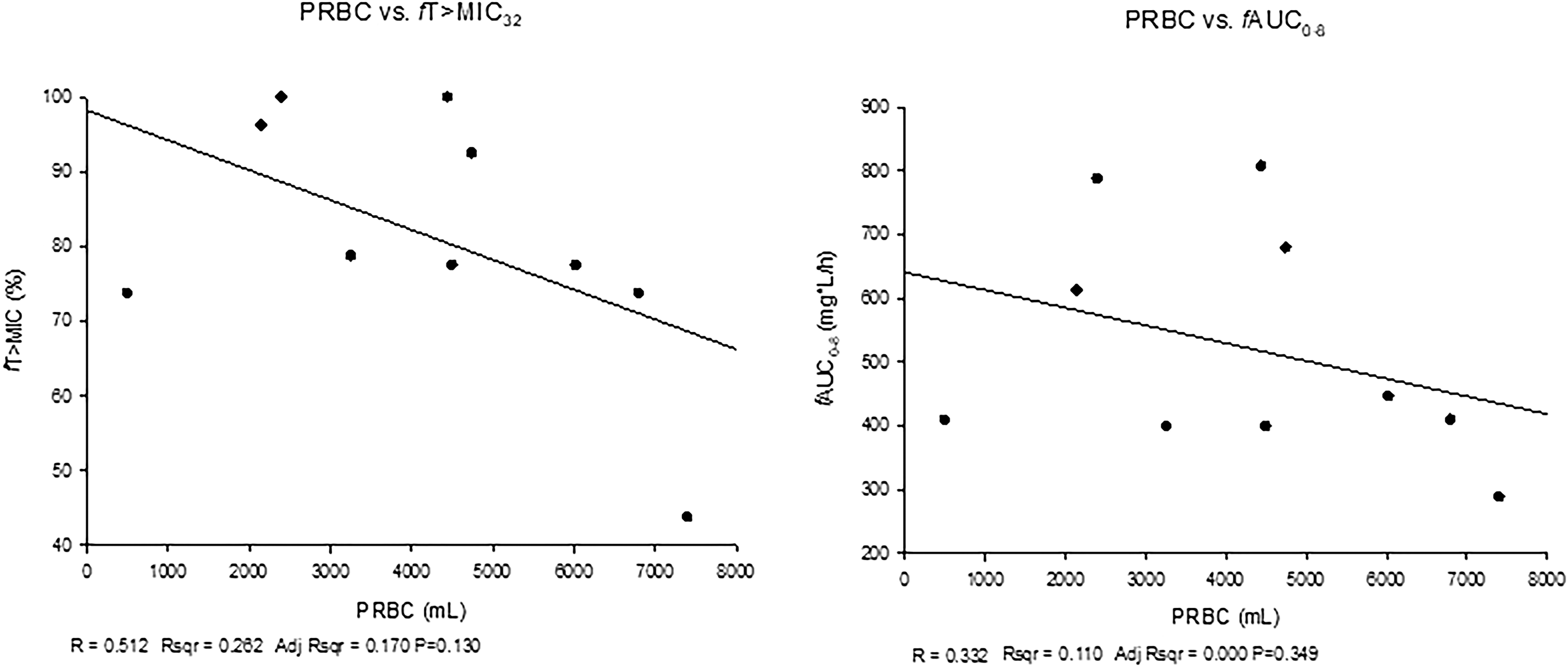
Linear regression for ampicillin free time above MIC32 (fT > MIC32) (left) and free area under the curve over eight hours (fAUC0-8) (right) versus volume of packed red blood cells (PRBC) received. MIC = minimum inhibitory concentration.
Coefficient of Determination (R2) and p Value from Linear Regressions of Ampicillin Exposures with Total Blood Product Volumes Administered During Surgery
% fT > MIC32 = percent of the dosing interval that free ampicillin concentrations remained above the minimum inhibitory concentration (MIC) value of 32 mcg/mL; fAUC0-8 = free ampicillin area under the curve from 0–8 hours; PRBC = packed red blood cells; FFP = fresh frozen plasma; PLT = platelets; ALB = albumin.
Monte Carlo simulations
The PTAs for the simulated regimens based on the ampicillin component of ampicillin-sulbactam are provided in Table 4.
Probability of Achieving 100% fT > MIC for the Ampicillin Component of Ampicillin-Sulbactam at SpecificAampicillin-Sulbactam MICs
fT > MIC = free time above the minimum inhibitory concentration (MIC); PTA = probability of target attainment
Discussion
Post-surgical infection continues to be the greatest cause of 30-day mortality in the liver transplant population [4–6]. Optimizing surgical prophylaxis regimens by maintaining antibiotic concentrations above the MIC for the duration of the procedure is imperative to mitigate surgical infection risk, however, the effects of blood loss and blood product replacement on antibiotic pharmacokinetics and exposure have not been established. In this study, we described the intra-operative pharmacokinetics of ampicillin-sulbactam during OLT and further explored the influence of blood product administration on exposure of the ampicillin component.
There are limited data characterizing the pharmacokinetics of ampicillin or sulbactam during liver transplantation. Arnow et al. [14] used non-compartmental pharmacokinetic analysis to evaluate cefotaxime given concomitantly with ampicillin in seven patients undergoing liver transplantation. All patients received ampicillin 2 g every six hours (infused over five minutes) during surgery. The investigators reported a mean ± standard deviation total body clearance and volume of distribution at steady state (Vss) of 11.0 ± 2.8 L/h and 16.0 ± 4.6 L, respectively. The reported half-life was 1.4 hours. Whereas their total Vss was similar to the median value of the patients in this study (∼19 L, total Vss calculated from [k12*Vc ]/k21), the ampicillin clearance was less than half of our findings (median, 23.12 L/h; Table 2). However, the median beta half-life for ampicillin in our patient population was similar at 1.3 hours (range, 0.4–1.7 hours.
A report by Muder et al. [22] evaluated cefoperazone and sulbactam pharmacokinetics during post-liver transplantation and reported sulbactam clearance and Vss of 7.2 ± 2.4 L/h and 20.7 ± 9.7 L, respectively. The observed half-life was 2.3 hours. Sulbactam Vss was comparable to that observed in our study population (20.1 L), but clearance was much lower than observed in the current findings (median, 29.61 L/h; Table 2). The substantial difference in clearance with no change in Vss was likely responsible for the lower observed sulbactam beta half-life in our population (median, 0.75 hours; range, 0.65–1.5 hours). These differences in total body clearances for both antibiotic agents might be explained by our 10 patients having moderately better estimated kidney function at baseline (CrCL, 98 mL/min vs. calculated 73 mL/min for Arnow et al. [14] and 66 mL/min for Muder et al. [22]), however, we were not able to identify a relation between CrCL and ampicillin CL in our analysis (covariate analysis not conducted for sulbactam). Notably, Muder et al. [22] were also not able to correlate intra-operative CrCL with the clearance of cefoperazone, another renally eliminated antibiotic. Additionally, the short dosing intervals (two to three hours) prescribed to our study patients may mask a more accurate estimation of the elimination half-lives for these drugs.
Finally, advancements in liver transplant surgical techniques from caval reconstruction technique with veno-venous bypass to a piggyback method may mitigate the risk for intra-operative renal impairment, thus diminishing its effects on drug clearance [2,23]. Whereas a few patients in the current study received the former method, most patients received the liver allograft through the piggyback method; the clamping technique used in the previous studies was not reported. Ultimately, more robust studies are warranted to delineate possible differences between surgical technique and impact on antibiotic clearance.
The volume of blood loss and blood product replacement during OLT can range from very little to massive (i.e., upwards of >100 units of total blood product administered) [24]. For perspective, an average-weight adult has eight to 12 units of PRBC volume, thus OLT recipients may have their full blood volume replaced upwards of 10-fold during surgery. Thus, the impact of blood product resuscitation on antibiotic exposure could be paramount to maintaining drug exposures required to prevent infection.
Swoboda et al. [25] evaluated cefazolin and gentamicin concentrations in relation to blood loss and reported a significant negative correlation between drug concentration and volume of blood loss in 11 patients undergoing elective procedures involving spinal instrumentation. Their observations should not be surprising, however, given drug concentrations reduce naturally over the duration of surgery and the absolute timing of the blood loss was not reported, but is more likely to accumulate with longer procedures. Their included patients received only a mean of three units of blood products and estimated free concentrations at the end of the approximate four-hour procedure were still above the MIC for Staphylococcus aureus. In contrast, Cameron et al. [26] evaluated the impact of blood product resuscitation on vancomycin pharmacokinetics, but the study included only burn patients, who themselves have different pharmacokinetics. Although the authors observed statistically significant reductions in vancomycin concentrations with greater PRBC replacement, they concluded the difference was not of clinical significance. However, the average PRBC received in that study was nine units, much lower than amounts often received during OLT. Indeed, the OLT patients included in the current study received on average 14 units of PRBC, but as many as 25 units, plus on average an additional seven units of FFP and six units of red blood cells via intra-operative cell salvage (i.e., cell saver).
Despite the large volumes of blood products received, as well as the robust range, we found no correlation between volume administered and ampicillin exposure, as calculated by time that free drug concentrations remained above the MIC of 32 mcg/mL or fAUC0-8 (Table 3, Fig, 3, Supplementary Figures S1–S5). The blood product with the highest coefficient of determination was PRBC, but the R2 was 0.11 to 0.26 and not significant. Blood product volume (specifically PRBC and FFP) was also evaluated during the pharmacokinetic model construction as covariates of ampicillin clearance or volume of the central compartment, but the resulting models did not provide improvements in fitting (data not shown). Collectively, these observations suggest little impact of blood product resuscitation on ampicillin pharmacokinetic parameters or exposure; therefore, re-dosing based on blood loss should not be necessary, provided the dosing regimen is optimized to begin with.
Cell salvage and autologous blood transfusion were also considered for inclusion into model development. This technique often used during high-bleed risk procedures minimizes the need for allogeneic blood transfusion [27–29]. Administration of cell salvage fluids may alter drug pharmacokinetics because of changes in volume of distribution and complete removal of drug during cell processing. Unfortunately, the timing of cell savage return to the patient was not recorded for many of the included patients, thereby preventing inspection of this covariate during population modeling. The impact of cell salvage has been previously studied in an ex vivo model, which suggested devices have minimal impact alone on extracellular drug concentrations but may play an additive role when added to blood loss and administration of blood products [30].
Although the pharmacodynamics of beta-lactam antibiotic agents are well established for treatment of infection, the exposures required for preventing a surgical infection have yet to be determined. In the absence of these data, it is suggested to maintain free beta-lactam concentrations above the target pathogen MIC for the entire duration of the surgery (i.e., 100% fT > MIC) [31]. In addition, epidemiologic bacterial resistance patterns must play a role in the selection of prophylaxis regimens. Ampicillin-sulbactam is a reasonable alternate choice for antibiotic prophylaxis during OLT because it covers the most common organisms causing deep tissue surgical infection after transplantation, including gram-negative enterics (Escherichia coli and Klebsiella pneumoniae), as well as methicillin-susceptible Staphlococcus aureus and Enterococcus spp. [13]. It also lacks activity and thus selective pressure against Pseudomonas aeruginosa, an organism less commonly associated with surgical infections in many OLT centers.
Using the population pharmacokinetic parameters derived from the 10 patients in this study, Monte Carlo simulations demonstrated that the standard ampicillin-sulbactam regimen typically used for treatment of infections (i.e., 2 g ampicillin/1 g sulbactam every six hours) results in a low probability (22%) of maintaining free ampicillin concentrations above 8 mcg/mL, the susceptibility breakpoint, for the duration of surgery (Table 4). However, re-dosing every two hours, as currently recommended in the surgical prophylaxis guidelines, will provide ≥96% probability of achieving this exposure against all susceptibility pathogens. The 2/1 g every two-hour regimen (as intravenous push or 0.5 hour infusion) also achieved high PTA at 16 mcg/mL, a MIC that would cover 81.8% of contemporary non-ESBL Escherichia coli and Klebsiellia pneumoniae in U.S. medical centers [21]. The PTA for these intermittent regimens drop off at MICs of 32 mcg/mL (MIC90 of non-ESBL Escherichia coli and Klebsiella pneumoniae), however, a loading dose followed by continuous infusion of ampicillin-sulbactam 6/3 g over eight hours would maintain these high exposures if necessary because of local MICs.
Conclusions
These data are the first to describe ampicillin-sulbactam pharmacokinetics in patients undergoing OLT. Blood product resuscitation was not observed to impact ampicillin pharmacokinetic parameters or exposure, thereby suggesting re-dosing based on blood loss or administration is unnecessary. Monte Carlo simulations suggest a minimum ampicillin-sulbactam dose of 2/1 g every two hours prior to incision and for the duration of the procedure will provide free time above the MIC against the majority of targeted pathogens that should be covered by the drug's spectrum. The results of this study can be used to guide intra-operative ampicillin-sulbactam dosing regimen selection in patients receiving OLT who do not require the anti-pseudomonal spectrum of piperacillin-tazobactam.
Footnotes
Acknowledgments
We acknowledge Elizabeth Martin, Debora Santini, and Christina Sutherland of the Center for Anti-Infective Research and Development for assistance with study coordination and analytical support, the Hartford Hospital transplant surgeons (Drs. Glyn Morgan, Caroline Rochon, and Patricia Ann Sheiner) and anesthesiologists (Drs. Joseph Hinchey, Leah Meisterling, Trevor Sutton, and Arun Uthayashankar), and all the Hartford Hospital liver transplant participants and their families for assistance with the conduct of study.
Funding Information
This study was funded by a grant from the Hartford Hospital Medical Staff and in kind support from the Center for Anti-Infective Research and Development.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.