
Abstract
Background:
Despite the high prevalence of acute appendicitis in children and substantial resource utilization associated with this condition, no consensus has been reached on optimal timing for performing appendectomies. The aim of this study was to examine the association between time to appendectomy and outcomes and assess the feasibility of delayed appendectomy in children.
Patients and Methods:
We performed a retrospective analysis of all patients younger than 14 years of age undergoing an appendectomy for suspected appendicitis. We divided our patients into two groups based on whether their time to appendectomy was shorter or longer than eight hours: group A, early appendectomy and group B, delayed appendectomy. Then we compared the two study groups regarding demographic, clinical, and radiographic characteristics, peri-operative data, and outcomes.
Results:
During the eight-year study period, a total of 1,141 patients underwent appendectomies. After applying exclusion criteria, 852 children were included: 544 (63.8%) in group A and 308 (36.2%) in group B. There were no differences in the rate of complicated appendicitis at exploration, post-operative complications, length of post-operative hospital stay, and 30-day re-admission rate between the two study groups.
Conclusions:
Our study demonstrated that delaying appendectomy within 24 hours of presentation is safe and feasible for pediatric acute appendicitis. Therefore, patients presenting during nighttime hours could be initially treated conservatively with antibiotic agents. This allows the surgeon to delay surgery to the following day.
Acute appendicitis is the most common abdominal emergency that requires surgical management in children [1]. In the United States, surgeons perform more than 70,000 pediatric appendectomies every year [2–4]. The presentation of appendicitis is highly variable, with less than 50% of patients presenting with classic signs and symptoms [5]. Therefore, acute appendicitis can still confound the most skilled surgeons leading to complications such as gangrene, perforations, or abscess formation. These complications are usually associated with increased morbidity and mortality [6]. Therefore, early appendectomy has been long accepted as the gold standard for the treatment of acute appendicitis [7,8]. However, in our daily practice, patients who are admitted with acute appendicitis during nighttime hours (10:00
Patients and Methods
After Institutional Review Board approval, we performed a retrospective analysis of all patients younger than 14 years of age undergoing an appendectomy for suspected appendicitis at a single university-affiliated hospital from January 1, 2013, through December 31, 2020. Pre-, peri-, and post-operative data were collected from medical files, operative reports, and pathology reports of all patients. These data included demographic information, comorbidities, clinical features, laboratory data, imaging data, time of admission, pre-operative antibiotic administration (patients receiving antibiotic agents before presentation to the emergency department), time of operation, post-operative antibiotic administration, and post-operative complications. Inclusion criteria for the subjects were: patients between the ages of two and 14 years at time of appendectomy and patients diagnosed with appendicitis by clinical suspicion or via ultrasonography or computed tomography scan. Exclusion criteria were patients with missing data, patients with no appendicitis on pathology report, patients with time to appendectomy longer than the 95th percentile, and patients transferred from another hospital.
The definition of complicated appendicitis was based on surgical exploration. Complicated appendicitis included perforated appendicitis, gangrenous appendicitis, and generalized peritonitis of appendicular origin or intra-abdominal abscess. Perforated appendicitis was defined as a hole in the appendix. In our institution, all patients with complicated acute appendicitis receive a standard course of post-operative antibiotic treatment combining cefotaxime-metronidazole (three times per day for five days) and gentamycine (once per day for three days). Then, antibiotic treatment may be prolonged through an oral formula based on the surgeon's preference (the total duration of post-operative antibiotic therapy is seven to 10 days). Patients with simple appendicitis may or may not receive a post-operative antibiotic therapy based on the surgeon's preference.
We defined time to appendectomy (TTA) as the time from emergency department registration to operative incision. We divided our patients into two groups based on whether their time to appendectomy was shorter or longer than eight hours: group A, early appendectomy with TTA of eight hours or less and group B, delayed appendectomy with TTA longer than eight hours. Then we compared the two study groups regarding demographic, clinical, and radiographic characteristics, and perioperative data. Outcome measures included length of stay, mortality, and morbidity including incisional and organ space surgical site infections, bleeding, small bowel obstruction, and 30-day re-admission rate. Patients presenting after hospital discharge with recurrent abdominal pain, fever, vomiting, or abdominal distension were re-assessed for complications. Finally, we limited our study to patients with a TTA within the 95th percentile (24 hours). Our aim was to focus on a delay from emergency department admission to operative incision representative of contemporary practice. We performed statistical analyses using SPSS Statistics, version 20 (IBM Corp, Armonk, NY). Significance was assumed with p values <0.05. We used χ2 tests to compare categorical variables including demographic, clinical, and radiographic characteristics, morbidity, and outcomes between group A and group B patients. For continuous variables, we used Student t-tests.
Results
During the eight-year study period, a total of 1,141 patients underwent appendectomies. After applying exclusion criteria, 852 children were ultimately included (Fig. 1). Five hundred forty-four patients (63.8%) underwent appendectomy within eight hours of emergency department registration, and 308 patients (36.2%) after eight hours. The median age was 10 years (interquartile range [IQR], 7–12 years). There were 554 males (65%) and 298 females (35%). The median (IQR) time from emergency department registration to skin incision was 5.2 (2.5–11.7) hours. Abdominal pain was present in all patients. Overall, 84.7% (722/852) of patients underwent a pre-operative abdominal ultrasonography (US). The most common finding in US was the presence of an increased peri-appendiceal fat echogenicity in 86.1% (622/722) of patients. Computed tomography scan was used in 15 patients. A comparison of demographic, clinical, and radiologic characteristics between early (group A) and delayed (group B) appendectomy patients found no differences (Table 1).
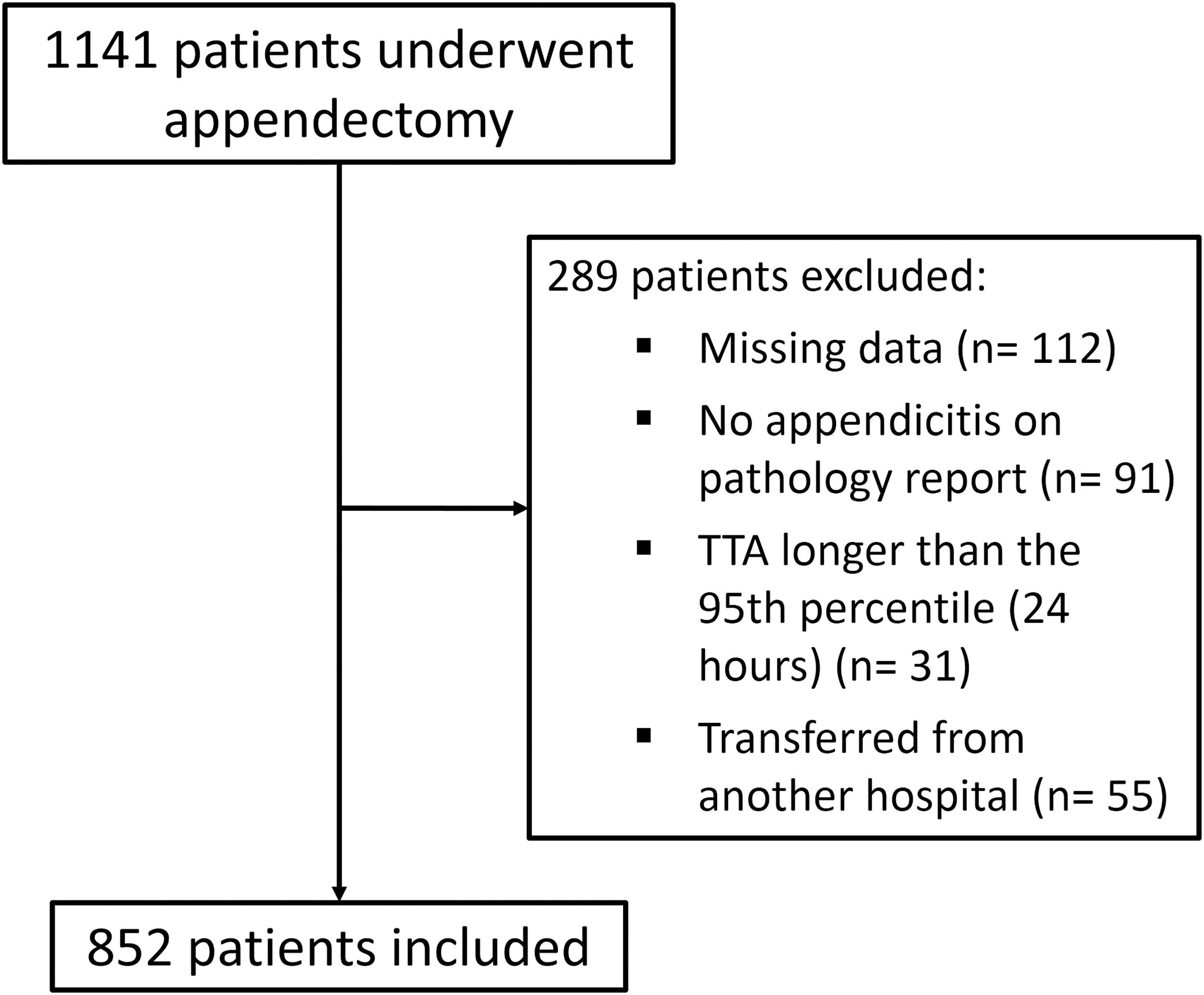
Study cohort assembly. TTA = time to appendectomy.
Comparison of Demographic, Clinical, and Radiologic Characteristics between Early (Group A) and Delayed (Group B) Appendectomy Patients
TTA = time to appendectomy; IQR = interquartile range; SD = standard deviation.
Table 2 shows the comparison of perioperative data between the two groups. There were no differences in operative time, pre- and post-operative antibiotic agent usage, the insertion of an intra-abdominal drain, the rate of complicated appendicitis at exploration, and the rate of a pathologic diagnosis of perforated appendicitis. There was a difference between early and delayed appendectomy groups in the ratio of operation during nighttime hours (10:00
Comparison of Peri-Operative Data between Early (Group A) and Delayed (Group B) Appendectomy Patients
TTA = time to appendectomy; SD = standard deviation.
We had no deaths in our study population. Overall, post-operative complications occurred in 42 patients (4.9%): 26 patients (3.1%) had surgical site infections, two (0.2%) had post-operative bleeding, six (0.7%) had urinary tract infections, and eight patients (0.9%) had small bowel obstructions. Twenty-two patients (2.6%) were re-admitted within 30 days of appendectomy. Among these 22 patients, 14 had intra-abdominal abscesses and eight had small bowel obstructions. Table 3 presents detailed overall outcomes and comparison between group A and group B patients. We found no differences between the two study groups regarding the overall morbidity (5.9% vs. 3.2%; p = 0.093), the length of post-operative hospital stay (66.6 ± 35.1 hours vs. 70.9 ± 35.9 hours; p = 0.086), and the 30-day re-admission rate (3.3% vs. 1.3%; p = 0.076).
Comparison of Outcomes between Early (Group A) and Delayed (Group B) Appendectomy Patients
TTA = time to appendectomy; n/a = not applicable; SD = standard deviation; SSI = surgical site infection.
Discussion
Several studies have examined the association between time to appendectomy and outcomes, but few have looked specifically at children. Even in the adult population, there is currently no consensus on the optimal timing for surgery in patients with appendicitis. Some surgeons suggested that the time from symptoms onset to appendectomy should not exceed 36 hours; other authors demonstrated that the time from presentation to surgery should not exceed 24 hours to avoid complications [9].
Our current study included one of the largest series worldwide studying the association between time to appendectomy and outcomes in children. Demographics, clinical, biologic, radiologic, and operative data of the two study groups were similar. This means that the features reflecting disease severity such as fever, guarding in the right iliac fossa, admission leukocytosis, and the presence of an appendicolith on ultrasound did not affect the timing of appendectomy.
In this study, there were no differences in outcomes between early and delayed appendectomy groups. This agrees with the majority of published studies that have reported similar rates of post-operative complications and adverse outcomes between early and delayed appendectomy [10–18]. However, other authors reported that delaying appendectomy, even for a short time of six to 12 hours, was associated with higher rates of post-operative complications such as surgical site infections [19–21].
Despite the strong evidence supporting the safety of delayed appendectomy, there is still no consensus on the optimal time of appendectomy in children. This is mainly because of the lack of studies that focused specifically on the pediatric population. In our daily practice, we still find it difficult to decide whether a patient who presents at 9:00
To fill these research gaps, this article presents a renovated analysis of the association between time to appendectomy and outcomes looking specifically on the pediatric population. Appendicitis in children is very different from that in adults especially in children younger than five years [22]. Communication with these children is usually difficult and their clinical presentation is non-specific. Moreover, irritability, inadequate physical examination, and overlap of symptoms with other common childhood diseases like mesenteric lymphadenitis, usually leads to a delayed diagnosis of acute appendicitis and a high misdiagnosis rate. Therefore, these children are more likely to develop complicated forms of acute appendicitis [22].
Our study showed that delaying appendectomy was not associated with an increase in complicated forms of acute appendicitis at surgical exploration. A literature review indicated that results in finding an association between time to appendectomy and risk of complicated disease were conflicting [18,19,21,23–30]. In a large study including 2,429 children, from 23 hospitals, recruited between 2013 and 2014, Serres et al. [31] found no association between time to appendectomy and an increased risk of complicated appendicitis. The authors suggested that we can manage pediatric appendicitis as an urgent rather than an emergent condition. They concluded that delaying appendectomy to the next day is a safe and an acceptable practice in children [31]. A meta-analysis was conducted by the United Kingdom Surgical Collaborative to evaluate the effect of timing of surgery on perforation rate. The results of this study revealed no differences between the different time-blocks (0–11 hours, 12–23 hours, 24–47 hours, and more than 48 hours) regarding the rate of perforated appendicitis [32].
Our study revealed that TTA was not associated with a prolonged length of post-operative hospital stay. Although Serres et al. [31] and Bolmers et al. [33] reported that a longer time to appendectomy was associated with a longer hospital stay, most published data suggested that the length of hospital stay was not affected by the time from admission to surgery [11,12,34–39].
In our series, 22 patients (2.6%) were re-admitted within 30 days from performing surgery. This rate is similar to that shown in the literature [11,40]. In our study, the 30-day re-admission rate was 3.3% in the early appendectomy group and 1.3% the delayed appendectomy group, the difference between the two study groups was not statistically significant. The same results have been reported by Shin et al. [12], Nagpal et al. [37], and Stahlfeld et al. [41].
The results of our study suggest that delaying appendectomy within 24 hours of presentation does not increase the rates of complicated appendicitis and adverse outcomes. In accordance with these results, current evidence shows that antibiotics as the initial treatment for uncomplicated acute appendicitis in children is safe and effective [42]. This has an impact not only in terms of management options, but also in terms of treating pediatric acute appendicitis as an urgent rather than an emergent condition. Moreover, recent data suggests that uncomplicated acute appendicitis in children could be managed medically with antibiotic agents. Therefore, surgery is not necessary in a large percentage of these cases [43]. However, we suggest that non-operative treatment is still an experimental treatment strategy for acute appendicitis in children. High-quality clinical trials with long follow-up are needed to validate this treatment option. These trials should take into account cost utility and outcomes. These findings could have important implications for the management of acute appendicitis in children, especially in developing countries. In fact, in our daily practice, we usually find significant logistical and fiscal challenges when performing surgical procedures during nighttime hours. Therefore, we suggest that appendectomy could be delayed to the next day without incurring any additional risk to the patient. However, we still consider that the optimal timing of appendectomy should be decided by the surgeon and should take into account the various factors involved such as available hospital resources.
The findings of this study should be considered in light of some limitations. First, it was a retrospective observational study. Therefore, errors in medical files documentation and data procurement were possible. Second, the present study does not consider the time from the onset of symptoms to hospital presentation when comparing the two study groups. Finally, we excluded patients with a prolonged TTA (>24 hours). We believe that patients with a delay from admission to appendectomy exceeding 24 hours should be considered as a separate cohort. These are often patients whose diagnosis remained uncertain after clinical and para-clinical examinations. These children were usually kept under observation in hospital for 24 to 72 hours.
Conclusions
In conclusion, our study demonstrated that delaying appendectomy within 24 hours of presentation is safe and feasible for pediatric acute appendicitis. Therefore, patients presenting during nighttime hours could be initially treated conservatively with antibiotic agents. This allows the surgeon to delay surgery to the following day. Non-operative management of pediatric acute appendicitis is still an experimental treatment strategy. High-quality clinical trials with long follow-up are needed to validate this treatment option.
Footnotes
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.