
Abstract
Background:
Necrotizing fasciitis is a potentially fatal soft tissue infection in which the timing of surgical intervention significantly affects clinical outcome. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, the Site other than the lower limb, Immunosuppression, Age <60 years, Renal impairment (creatinine >141), and Inflammatory markers (CRP ≥150, WCC >25) (SIARI) score, and procalcitonin levels are intended to aid in the decision-making process to differentiate between necrotizing fasciitis and soft tissue infections.
Methods:
A retrospective analysis of cases of necrotizing fasciitis and soft tissue infections treated at Klinikum Nürnberg was performed. The two scores as well as procalcitonin levels were tested for their diagnostic value and a new score, the Laboratory and Anamnestic Risk Indicator for Necrotizing Fasciitis (LARINF), was created based on the results.
Results:
Procalcitonin, LRINEC score, and SIARI score showed insufficient discriminatory ability in our study. The newly created LARINF score combined laboratory parameters of the LRINEC score (hemoglobin and C-reactive protein) with procalcitonin and three comorbidities, resulting in a sensitivity of 84% and a specificity of 75% and the highest area under the receiver operating characteristic (ROC) curve of 0.83.
Conclusions:
The LARINF score is a novel decision-supporting tool. The decision, in which cases surgical exploration should be initiated, remains a clinical one. However, the score seems to provide an improved basis for identifying a rare clinical picture.
Necrotizing fasciitis (NF) is a subgroup of necrotizing soft tissue infections (NSTI) and represents a life-threatening soft tissue infection. Because of its rapid progression, it is associated with high morbidity and mortality. The mortality rate is approximately 13%, 1 and is strongly correlated with the timing of surgical treatment.2,3 Nawijn et al. 2 demonstrated the correlation between the timing of surgical debridement and the clinical outcome and coined the expression “time is fascia.” A case report by Almarzouqi et al., 4 in which a 17-year-old female developed NF after the birth of her child secondary to episiotomy and died 16 hours after admission to a tertiary hospital, further highlights the rapid spread of this disease. The clinical manifestations of NF, such as fever, hemorrhagic bullae, or swelling and erythema, are multifaceted and often ambiguous, making it nearly impossible to make a definitive diagnosis.5,6 Another subtype of NSTIs is gas-forming myonecrosis, in which intra-abdominal lesions are often involved and features of a systemic infection appear early in the course of the disease. 7 The two main factors determining early surgical therapy are the time of the patient's arrival after symptom onset and doctors delay, i.e., time from presentation to surgery. 2 Effective scoring systems could aid in reducing the time until surgical intervention.
In 2004, Wong et al. 8 introduced the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score. The score is designed to help distinguish NF from other soft tissue infections using six laboratory parameters (Table 1). The score has since been evaluated in numerous studies with varying conclusions regarding its applicability.9–12 The meta-analysis by Fernando et al. 5 came to the conclusion that the LRINEC score is not appropriate to exclude necrotizing fasciitis. In 2019, Cribb et al. 13 presented a new decision aid, the Site other than the lower limb, Immunosuppression, Age <60 years, Renal impairment (creatinine >141), and Inflammatory markers (CRP ≥150, WCC >25) (SIARI) score, that in addition to laboratory parameters, also includes the site of infection, age, and history of immunosuppression (Table 1). Kishino et al. 14 demonstrated the diagnostic value of procalcitonin (with a cutoff value of 1 ng/mL) for differentiating NF from soft tissue infections in their study from 2021.
The LRINEC Score
A score of 6 or 7 indicates moderate risk for NF and a score ≥8 indicates high risk for NF as described by Wong et al. 8 The SIARI score (the cutoff value for necrotizing fasciitis is ≥3) as described by Cribb et al.,13
LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis score; SIARI = Site other than the lower limb, Immunosuppression, Age <60 years, Renal impairment (creatinine >141), and Inflammatory markers (CRP ≥150, WCC >25 score; NF = necrotizing fasciitis.
The aim of this study was to evaluate the discriminatory ability of the LRINEC and SIARI sores as well as procalcitonin levels in the differentiation between NF and other soft tissue infections. Based on those results we aimed to develop a new scoring system combining the best aspects of these existing diagnostic tools and with higher diagnostic power. To that end, we introduce the Laboratory and Anamnestic Risk Indicator for Necrotizing Fasciitis (LARINF).
Methods
Formation of study population
Data were extracted retrospectively from our hospital database at Klinikum Nürnberg. The search criteria were International Classification of Diseases (ICD) codes for NF for the NF group and ICD codes for soft tissue infections for the soft tissue infection (STI) group; the search period was January 2003 to January 2022. Surgical therapy and intravenous antibiotic agents were additional inclusion criteria. For inclusion in the NF group, a chart review was performed, and the diagnosis of NF also had to be documented in the discharge letter, whereas the diagnosis was determined based on histologically confirmed findings. Other subgroups of NSTI were not included in the study. After the exclusion of patients whose current infection has been pre-operated in another hospital, a total of 130 cases with NF and 330 cases of STI remained. Laboratory values at admission were evaluated in this study.
Because this study was designed to test the LRINEC score, SIARI score, and procalcitonin as diagnostic tools, all patients with missing procalcitonin levels and in whom the scores could not be calculated because of missing data were excluded from the study 8,13,14. Most patients had to be ruled out because of missing procalcitonin levels, resulting in the exclusion of 44 additional cases from the NF group and 266 cases from the STI group. This study was conducted in accordance with the Declaration of Helsinki. Due to the retrospective and anonymous study protocol, an ethics vote was waived. All data analyzed were collected as part of routine diagnosis and treatment.
Statistical analysis
Data collection was executed in Microsoft® Excel (Microsoft Corporation, Redmond, WA) and statistical analysis in Microsoft® Excel and IBM SPSS Statistics (IBM Corp, Armonk, NY). Patients with missing values for procalcitonin were excluded from the study. The missing values for procalcitonin was not random but rather patients with severe STIs were more likely to have a value for procalcitonin. In addition, more than 50% of the patients with STI had missing procalcitonin values. Multiple imputation was therefore considered inappropriate. Significances were analyzed using t-tests and χ 2 tests, and a two-sided p value <0.05 was set as the significance level. Diagnostic tools were compared using the area under the receiver operating characteristic (ROC) curve and sensitivity, specificity, positive predictive value, and negative predictive value at the selected cutoff values. The LARINF score was generated from results of a multivariable logistic regression. Laboratory values of LRINEC score, hematocrit, procalcitonin, age, and all comorbidities included in the study were used as variables. The cutoff value for CRP was determined using the Youden Index. The cutoff values of hemoglobin and procalcitonin from the study by Wong et al. 8 and Kishino et al. 14 were applicable to our data and were therefore adopted in the LARINF score.
Results
Study population
A total of 86 patients with NF (NF group) and 64 patients with STIs (STI group) were included in the study. Descriptive data for the two groups can be found in Table 2. The age and gender distribution did not differ substantially between the two groups. All investigated comorbidities and risk factors except alcohol and drug abuse were relatively more frequent in the NF group than in the STI group. However, statistically significant differences were found only for heart, liver, or renal insufficiency and hypertension. In the NF group, the most common site of infection was the lower extremity (47%), whereas in the STI group, the upper extremity (52%) was most commonly effected. The length of hospital stay and mortality rate were higher in the NF group (p < 0.001).
Demographics, Comorbidities, and Risk Factors, Site of Infection, Laboratory Values, Scoring Results, and Outcome Parameters of NF and STI Groups
Values in bold indicate statistically significant results.
NF = necrotizing fasciitis; STI = soft tissue infection; LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis score; SIARI = Site other than the lower limb, Immunosuppression, Age <60 years, Renal impairment (creatinine >141), and Inflammatory markers (CRP ≥150, WCC >25 score; LARINF = Laboratory and Anamnestic Risk Indicator for Necrotizing Fasciitis.
Laboratory values and scoring systems
Laboratory parameters and the aforementioned diagnostic tools were compared between the two groups. Among the laboratory parameters, the average values for C-reactive protein (CRP), leukocyte count, sodium, creatinine, glucose and procalcitonin were higher in the NF group than in the STI group. Mean hemoglobin and hematocrit levels were lower in the NF group. Statistically significant differences were seen for hemoglobin, hematocrit, creatinine, and procalcitonin. The mean LRINEC, SIARI, and LARINF scores were higher in the NF group. For LRINEC score (6.5 compared with 4.9) and LARINF score (6.2 compared with 3.4), the differences were statistically significant.
The LARINF score is composed of three laboratory values (hemoglobin, procalcitonin, and C-reactive protein) and three comorbidities (heart, liver, or renal insufficiency combined as a single parameter, immunosuppression, and obesity; Table 3). The scoring result is formed by summing the points from the six items and thereby a value between 0 and 11 can be obtained, with the cutoff value for increased risk for NF being a score ≥5.
The Laboratory and Anamnestic Risk Indicator for Necrotizing Fasciitis (LARINF)
The cut-off value for an increased risk for necrotizing fasciitis is a score ≥5.
Diabetes mellitus should not be counted as immunosuppression in this regard.
In Table 4, the parameters of diagnostic quality of procalcitonin, LRINEC, SIARI, and the newly presented LARINF score are presented. The LRINEC score ≥8 had the highest specificity, but with low sensitivity (41%). The LARINF score showed the highest sensitivity, positive predictive value, and negative predictive value. The three scores, as well as procalcitonin, were subjected to a receiver operating characteristic curve analysis (Fig. 1). The LARINF score had the highest area under the receiver operating characteristic curve (AUROC) with 0.827.
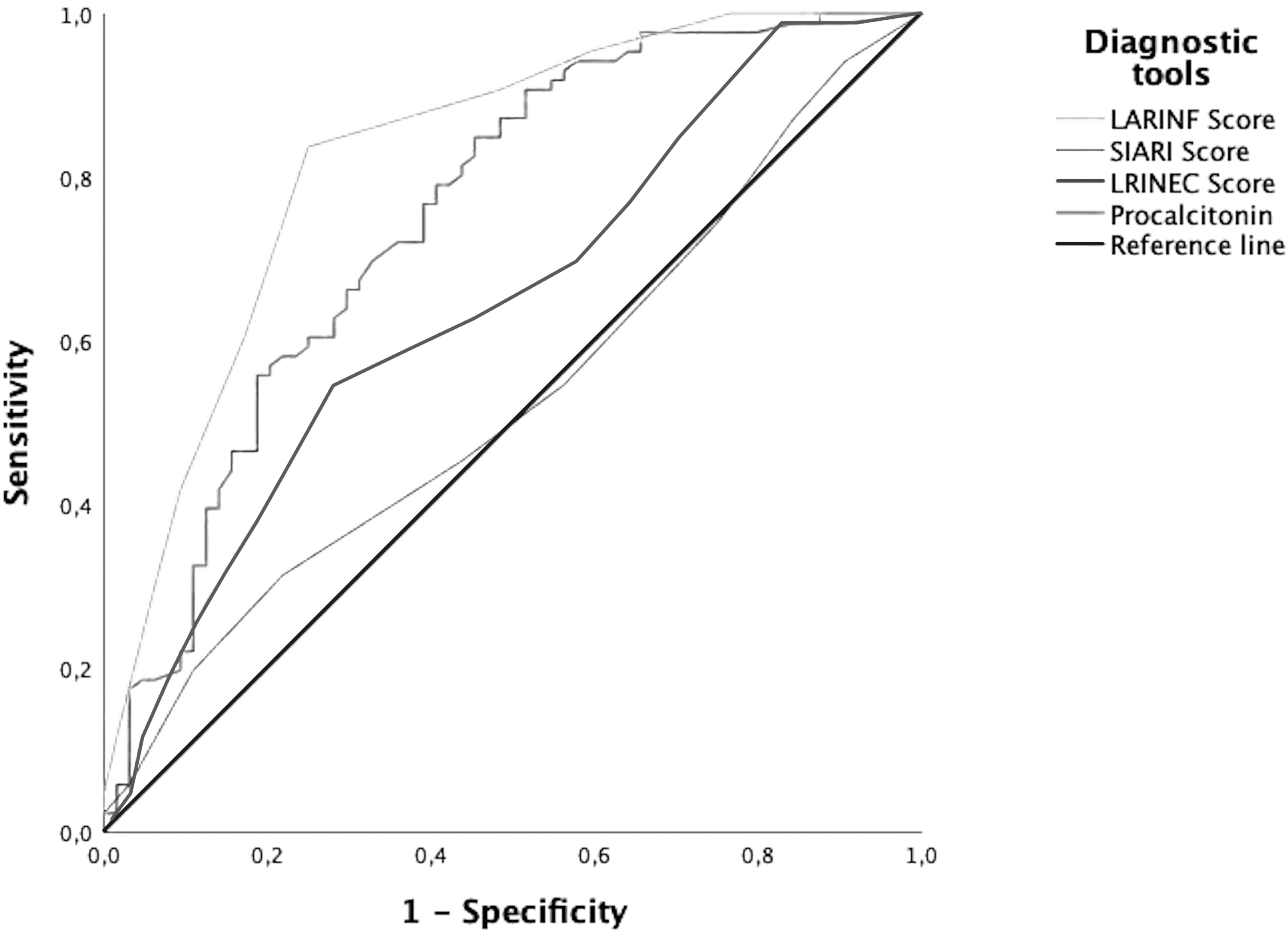
Receiver operating characteristic (ROC) curves of procalcitonin, Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, Site other than the lower limb, Immunosuppression, Age <60 years, Renal impairment (creatinine >141), and Inflammatory markers (CRP ≥150, WCC >25 (SIARI) score, and Laboratory and Anamnestic Risk Indicator for Necrotizing Fasciitis (LARINF) score.
Parameters of Diagnostic Quality for Procalcitonin, LRINEC, SIARI, and LARINF Scores
LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis score; SIARI = Site other than the lower limb, Immunosuppression, Age <60 years, Renal impairment (creatinine >141), and Inflammatory markers (CRP ≥150, WCC >25 score; LARINF = Laboratory and Anamnestic Risk Indicator for Necrotizing Fasciitis; ROC = receiver operating characteristic.
Discussion
Our study demonstrates that neither the LRINEC score, the SIARI score, nor procalcitonin showed sufficient discriminatory ability, with procalcitonin showing the best correlation with an AUROC curve of 0.75. The newly formed LARINF score, which incorporates procalcitonin and three comorbidities in addition to hemoglobin and C-reactive protein, showed a sensitivity of 84% and a specificity of 75% with a cutoff value of ≥5. The AUROC was 0.827 for the LARINF score. A test with an AUROC between 0.8 and 0.9 is considered to provide excellent diagnostic accuracy. 15
SIARI score
In the study by Cribb et al., 13 the sensitivity (81%–84%) and specificity (70%–73%) of the SIARI score were markedly higher than in our study. However, the composition with respect to the localization of the infections of the control group (STI group) differed considerably. Whereas in the study by Cribb et al. 13 the most frequent site was the lower extremity (94%), in our study it was the upper extremity with 52%. Because a site outside of lower limb results in 3 points in the SIARI score and the cutoff value is a score ≥3, this resulted in a very low specificity (25%) in our study. On this basis, it can be concluded that the specificity of the score is limited in a patient population with predominantly upper extremity infections. The sensitivity of the score was 74% in our study. In the study by Kishino et al., 14 the sensitivity of the SIARI score was 68% and the specificity was 68% and 73%, respectively (and thereby notably higher than in our study), depending on whether the control group consisted of patients with cellulitis or severe cellulitis. However, an elevated cutoff value for the SIARI Score of ≥4 was used in this study. We agree on the implementation of additional factors, in particular immunosuppression, as this may further improve the diagnostic value.
Role of procalcitonin and the development of a novel decision-making tool
The basis for the development of a new scoring system was the promising results of procalcitonin in our ROC analysis that outperformed the LRINEC score and SIARI score as a single laboratory value. However, the sensitivity (74%) and specificity (61%) at the cut off value of ≥1 was found to leave room for improvement in our study. In the study by Kishino et al., 14 procalcitonin with the same cutoff value had a sensitivity of 88% and specificity of 90%–93%, depending on whether the control group was patients with cellulitis or severe cellulitis. The case group was relatively small in this study, with 25 patients with NF. Procalcitonin levels were found to be dependent on the pathogen causing the possible bacteremia, with gram-negative pathogens being associated with higher procalcitonin levels.14,16
Regional differences in the pathogen spectrum of NF may accordingly also alter procalcitonin levels. Consequently, there might also be a relation between the causative agents of NF. In addition to the diagnostic importance, a study by Al-Thani et al. 17 also shows a prognostic value of procalcitonin levels and suggests a cutoff value of 5.6 ng/mL for the prediction of septic shock. In addition to C-reactive protein and hemoglobin, which were adopted from the LRINEC score, three comorbidities were implemented as scoring factors in the LARINF score. In the existing literature there are several publications describing associated comorbidities,6,18–20 and suggestions have been made to include clinical factors to the LRINEC score. 21 Leukocyte count, sodium, creatinine, and glucose did not further improve the diagnostic value of the scoring system in our study. The clinical signs and symptoms of patients with NF are often indistinct. 5 For this reason, and because the scoring system is intended to provide a simple and clear classification of patients, clinical factors (such as fever, redness, swelling) were not taken into consideration.
Outlook
In our study, the LARINF score showed high diagnostic value as a decision-supporting tool in possible NF cases. In addition to developing strategies to accelerate the diagnosis of necrotizing fasciitis, additional therapeutic options such as hyperbaric oxygen therapy also seem to show prognosis improving results.22,23 A strength of our study is the implementation of existing diagnostic scores into a combined scoring system. In addition, multiple imputation was avoided to eliminate a source of bias. However, this resulted in a reduced study population with the STI group predominantly consisting of severe STIs. This complicated the differentiation between NF and other STIs for all diagnostic tools tested. Because of the small number of cases in both groups, the study population was not divided into a developmental and a validation cohort, indicating that the study results still require external validation studies.
The retrospective study protocol is another limitation of this study. Because of the correlation between individual laboratory parameters and microbiologic results, it should also be examined in the future whether the LARINF score can be used independently of the causative pathogen. An area of future research should be an internal prospective validation of our study results as well as external studies comparing the LARINF score with existing and also novel scoring systems such as the CologNe-FaDe-Score and the Modified Laboratory Risk Indicator for Necrotizing Fasciitis (MLRINEC) score.24,25 The mentioned scores have included lactate as an additional factor, which was only sparsely available in our database and did not allow a comparison.
In addition to the comparison in terms of diagnostic accuracy, further studies can investigate whether the LARINF score also provides discriminative abilities in other subtypes of NSTIs or whether prognostic conclusions can be drawn from the scoring results. The diagnostic power of the LARINF score was the highest compared with the other diagnostic tools studied. However, sensitivity and specificity were not 100%, so it must be concluded that this newly created score also does not provide an error-free basis for decision-making and that the timely diagnosis of NF remains a dilemma. A total of 16% of NF cases were classified as low risk for NF, mainly because these patients did not have elevated procalcitonin levels and comorbidities relevant to the LARINF score. Nevertheless, the LARINF score is a strong instrument and represents an adjunct for the diagnostic process. When patients present with necrotizing fasciitis, often a misdiagnosis occurs initially. 26 The newly created LARINF score can be an aid to the difficult diagnostic process. Scoring systems, however, remain only supportive tools for the decision-making and should not be used in isolation. As with the existing scoring systems, a low LARINF score should also not overrule clinical suspicion of NF in the decision to perform surgical exploration.
Conclusions
Procalcitonin, the LRINEC, and SIARI scores showed unsatisfactory discriminative abilities in our study. The LARINF combines elements of the LRINEC score, SIARI score, procalcitonin, and two additional comorbidities. The dilemma of in which cases to initiate surgical exploration remains a clinical decision. However, in comparison to the diagnostic tools, the LARINF score appears to provide an improved basis for the identification of a rare clinical picture.
Footnotes
Authors' Contributions
Conceptualization: D.B. and I.-F.M. Methodology: I.-F.M., D.B., A.A.B., and M.B. Validation: I.-F.M., B.R., G.G., and A.M. Formal analysis: D.B., I.-F.M., W.H., and A.A.B. Investigation: D.B., A.M., and A.A.B. Resources: B.R. Surgical procedures: B.R., A.A.B., M.B., A.M., and I.-F.M. Data curation: D.B., W.H., I.-F.M., and G.G. Writing—original draft preparation: D.B., I.-F.M., G.G., and A.M. Writing—review and editing: I.-F.M., G.G., M.B., D.B., and B.R. Visualization: D.B., W.H., and M.B. Supervision: I.-F.M., B.R., and G.G. Project administration: I.-F.M. All authors have read and agreed to the published version of the manuscript.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
The authors declare no conflict of interest.