
Abstract
Background:
Post-injury inflammation and its correlation with anemia recovery after severe trauma is poorly described. Severe injury induces a systemic inflammatory response associated with critical illness and organ dysfunction, including disordered hematopoiesis, and anemia. This study sought to characterize the resolution of post-injury inflammation and anemia to identify risk factors associated with persistence of anemia.
Patients and Methods:
This single-institution study prospectively enrolled 73 trauma patients with an injury severity score >15, hemorrhagic shock, and a lower extremity long bone orthopedic injury. Blood was obtained at enrollment and after 14 days, one, three, and six months. Analytes were compared using Mann-Whitney U tests with correction for multiple comparisons.
Results:
Median age was 45 years and Injury Severity Score (ISS) was 27, with anemia rates of 97% at two weeks, 80% at one month, 52% at three months, and 30% at six months. Post-injury elevations in erythropoietin, interleukin-6, and C-reactive protein resolved by one month, three months, and six months, respectively. Median granulocyte colony-stimulating factor (G-CSF) and tumor necrosis factor (TNF)-α concentrations remained elevated throughout the six-month follow-up period. Patients with persistent anemia had longer intensive care unit and hospital lengths of stay, more infectious complications, and received more packed red blood cell transfusions compared to those with early anemia recovery.
Conclusions:
Severe trauma is associated with a prolonged inflammatory response, which is associated with increased transfusion requirements, lengths of stay, and persistent anemia. Further analysis is needed to identify correlations between prolonged inflammation and clinical outcomes after discharge.
Anemia occurs in nearly all patients after severe traumatic injury and persists even after the initial acute blood loss has resolved.1,2 This injury-associated anemia, although similar to anemia of inflammation, has unique features and a multifactorial etiology. 3 After acute injury, there is a systemic inflammatory and hypercatecholamine response with evidence of suppressed erythroid progenitor cell growth, impaired iron regulation despite adequate iron stores, an altered erythropoietin response, and prolonged mobilization of hematopoietic progenitors from the bone marrow to injured tissues.3–5
Anemia, however, is not limited to those individuals who experience traumatic injury with acute blood loss. It is common among uninjured critically ill patients, as well as those with chronic critical illness, but is not completely understood.3,6 Within their first eight days in the intensive care unit (ICU), almost all (97%) of critically ill patients were anemic, and more than 75% of survivors remain anemic at hospital discharge.1, 2 Previous studies have identified persistent anemia among ICU survivors and up to 50% of individuals are still anemic six months later.7–9 Anemia remains a negative prognostic factor associated with organ failure, increased length of stay, and increased mortality.10–12 Recent data also suggest that after sepsis and critical illness, the presence of anemia correlated with reduced physical function at 12 months. 13 The failure of various therapeutic agents, including iron and erythropoietin, to alleviate anemia of critical illness in clinical trials, suggests that further study is required to define mechanisms involved in patients at risk for persistent anemia.14–17
Despite the high incidence of post-injury anemia, recovery from anemia has not been defined long-term. This represents a gap in our understanding of post-injury anemia recovery and clinical outcomes after severe trauma. This study sought to characterize anemia recovery over six months after injury with serial assessment of hemoglobin, cytokines, and iron and explored factors that might contribute to persistence of anemia. We hypothesized that severe trauma associated with prolonged inflammation would correlate with lack of anemia recovery.
Patients and Methods
Study population
We performed a prospective observational cohort study of severely injured blunt trauma patients (n = 73) from a level 1 trauma center between October 2017 and June 2021. Patients were screened on admission for inclusion in the study, with prior approval by the Institutional Review Board (IRB201601386). Inclusion criteria were as follows: age ≥18; lower extremity long bone or pelvic fracture requiring operative repair; hemorrhagic shock at time of admission (defined by systolic blood pressure ≤90 mm Hg, or mean arterial pressure ≤65 mm Hg, or base deficit ≥5 mEq/L or lactate ≥2 mmol/L); and an Injury Severity Score (ISS) ≥15. Exclusion criteria included: survival <48 hours; incarceration; pregnancy; patients receiving long-term corticosteroids or immunosuppressive therapies; previous bone marrow transplantation; or end-stage renal disease.
This study was registered at ClinicalTrials.gov (NCT02577731). All non-intubated trauma patients gave written informed consent for the research procedures. For those critically ill trauma patients who were not able to provide written informed consent for tissue sampling, written informed consent was obtained from their surrogate decision maker. In such cases, written informed consent was later obtained from the patient when they regained decision-making capacity.
Patient characteristics
Clinical data regarding patient demographics and operative management were obtained from the electronic medical record by a physician reviewer and stored in an encrypted database. Demographic data included age, gender, hospital and ICU length of stay, transfusions received, discharge disposition, and complications (thrombotic, infectious, or other). Infectious complications were identified using a combination of progress notes, positive culture data, and the use of antimicrobial agents either in the setting of documented clinical suspicion or when otherwise not documented as prophylaxis.
Clinical anemia was defined as hemoglobin <12 g/dL in females and <13.5 g/dL in males. Mild anemia was defined as hemoglobin between 10.0 and <12.0 g/dL in females and between 10.0 to <13.5 g/dL in males. For both males and females, moderate anemia was defined as hemoglobin 8.0 to <10.0 g/dL, and severe anemia defined as hemoglobin <8.0 g/dL.
Blood collection and processing
Blood samples were obtained on the day of operative fracture fixation, at two weeks, one month, three months, and six months. Blood was collected in a fully filled heparinized 6 mL tube (Becton Dickinson, Franklin Lakes, NJ) that was spun at 800g for 10 minutes to separate plasma. Plasma was collected and stored in a −80°C freezer. Plasma norepinephrine (NE), hepcidin, C-reactive protein (CRP), interleukin (IL)-6, hepcidin, total iron, granulocyte colony stimulating factor (G-CSF), tumor necrosis factor (TNF)-α, and erythropoietin levels were measured using immunosorbent assays according to manufacturers' protocols (NE, Abnova, Taipei, Taiwan; iron, BioAssay Systems, Hayward, CA; all others, R&D Systems, Minneapolis, MN).
Statistical analysis
All statistical analyses were conducted in GraphPad Prism Version 9.2 (GraphPad Software, La Jolla, CA). Statistically significant differences between categorical variables were identified using Fisher exact test. Differences in clinical parameters and plasma analytes were detected using Mann-Whitney U tests with correction for multiple comparisons and an adjusted p value threshold set to 0.05. Continuous variables are presented as median (interquartile range) and categorical variables are presented as frequency (%).
Results
Study population
Of 113 trauma patients enrolled in the study from 2017–2021, 13 opted to withdraw from the study and 27 were found to not meet criteria because of low ISS and were subsequently excluded from analysis post hoc, leaving 73 subjects for analysis. There was one mortality in the study on day 14. Of the remaining 72 trauma patients, 88% had follow-up at two weeks, 40% at one month, 32% at three months, and 32% at six months. Demographic data are presented in Table 1. Sixty-three percent of trauma patients were male, with a median age of 45 years (31–59 years] and ISS of 27 (22–34).
Demographic Data of Patients Included in the Study
Data presented as median [IQR] or n (%).
ICU = intensive care unit; PRBC = packed red blood cells; IQR = interquartile range.
Time course of anemia after injury
On admission, median hemoglobin was 11.6 g/dL (10.2–13.1 g/dL). Median time to operative fracture fixation (and sample collection) was two days (1–4 days] after injury, at which time the median hemoglobin had decreased to 9.2 g/dL (8.25–10.1 g/dL). By day of enrollment, 96% of trauma patients met criteria for clinical anemia (Fig. 1). Anemia persisted throughout the duration of the study with a prevalence of anemia at two weeks of 97%, 80% at one month, 52% at three months, and 30% at six months (Fig. 1). Two weeks after injury, prevalence of anemia severity was characterized as 28% mild, 59% moderate, 11% severe (Fig. 1). The rate of moderate-to-severe anemia after severe traumatic injury remained high at 69% at two weeks and 35% at one month. At three months, 52% of subjects were anemic and 13% were moderately to severely anemic. By six months, only 5% of subjects had moderate-to-severe anemia. There were no differences in mean corpuscular volume, mean corpuscular hemoglobin, or mean corpuscular hemoglobin concentration at any time in the study (Table 2). Red blood cell distribution width (RDW) was increased at two weeks, one month, and three months post-injury compared with reference values of 11%–14% (Table 2).
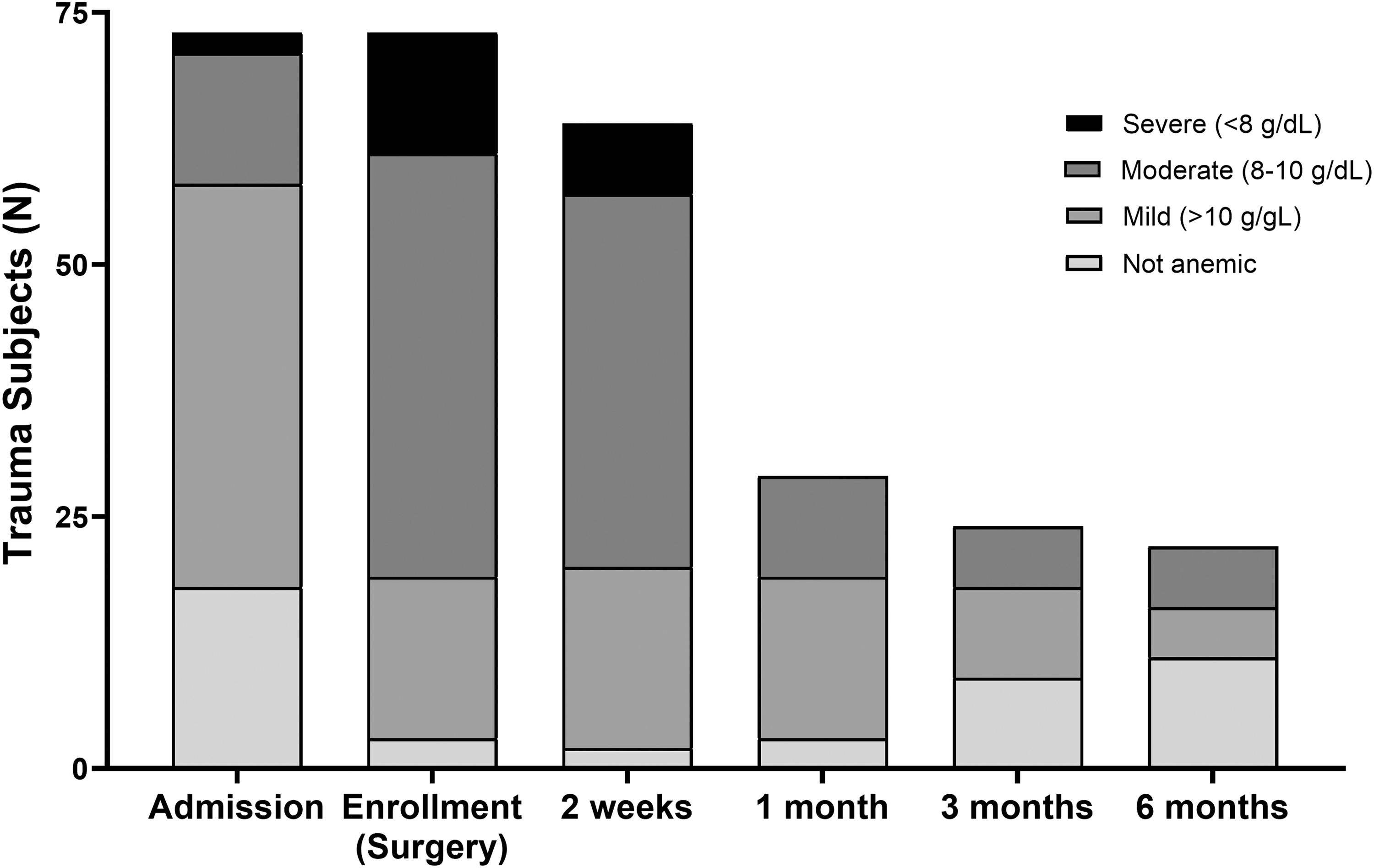
Classification of anemia severity over time in enrolled trauma patients.
Parameters of Erythropoiesis, Iron Metabolism, and Inflammation Throughout the Study
Data presented as median [IQR].
MCV = mean corpuscular volume; MCH = mean corpuscular hemoglobin; MCHC = mean corpuscular hemoglobin concentration; RDW = red cell distribution width; EPO = erythropoietin; CRP = C-reactive protein; TNF-α = tumor necrosis factor-α; NE = norepinephrine; G-CSF = granulocyte-colony stimulating factor; IQR = interquartile range.
Hepcidin levels and iron metabolism
Median plasma erythropoietin was elevated for one month after injury compared with reference intervals of 5–36 mIU/mL (Table 2). Systemic iron levels decreased acutely on days one to four of admission but returned to normal by two weeks (Table 2). Median plasma hepcidin levels were elevated on days one through four after injury and decreased over time (Table 2). Similarly, erythroferrone, released by erythrocytes as an inhibitor of hepcidin, was also elevated early on days one through four after injury and again at six months.
Markers of stress and inflammation after injury
Interleukin-6, TNF-α, and CRP were all elevated after severe trauma. Interleukin-6 remained elevated for at least one month and had not returned to normal until three-month follow up (Table 2). Tumor necrosis factor-α remained elevated for the entire duration of the study, up to six months, after trauma. Median CRP levels were elevated for at least three months (Table 2). Median plasma NE levels were elevated in trauma patients for up to two weeks after injury. Median G-CSF levels were highest early after injury but remained elevated at six months (Table 2).
Outcomes defined by anemia recovery
Trauma patients who were anemic at hospital discharge were divided into two groups for further analysis: those who had resolution of anemia by three months (early anemia recovery), and those who required longer than three months or had still not recovered at six months (prolonged anemia). Patients with prolonged anemia had a longer ICU length of stay and hospital length of stay and received more packed red blood cell transfusions both overall and during the first 24 hours of admission (Table 3). They also had a higher infectious complication rate when compared to those with early anemia recovery (Table 3). The presence of an infectious complication correlated with persistent anemia (odds ratio [OR], 7.1; 95% confidence interval [CI], 1.078–57.460; p = 0.0415). Based on anemia recovery, there was no statistically significant differences in ISS, age, gender, or discharge location.
Outcomes Defined by Anemia Recovery at Six Months
Data presented as median [IQR] or n (%).
p < 0.05.
ICU = intensive care unit; PRBC = packed red blood cells; AIS = abbreviated injury scale; IQR = interquartile range.
Similarly, we also sought to examine if any cytokines and inflammatory markers were predictive of early anemia recovery as defined above. Unfortunately, this study was underpowered for such a post hoc analysis of any samples beyond those collected on enrollment because of long-term follow-up limitations. There was no statistically significant difference in any of the cytokines or signaling factors assayed on samples drawn at time of enrollment (Table 4).
Plasma Analytes at Time of Enrollment Defined by Anemia Recovery at Six Months
Presented as median [IQR].
IL-6 = interleukin-6; G-CSF = granulocyte-colony stimulating factor; CRP = C = reactive protein; NE = norepinephrine; TNF-α = tumor necrosis factor-α; IQR = interquartile range.
Discussion
In this study, anemia is universal after severe traumatic injury and present in almost 100% of patients at hospital discharge. A moderate-to-severe anemia persisted in nearly 30% of patients six months after injury. Injured patients exhibited elevations in inflammatory and pro-hematopoietic mobilization cytokines extending up to six months after injury. Anemia persisted despite early elevations in erythropoietin levels and improvements in iron levels beyond the first two weeks. This is the first study that examines anemia recovery in trauma patients following severe injury.
Our six-month anemia rates were lower than published data from the wider critically ill population.7,18 In a retrospective analysis of over 6,900 ICU all-comers, Warner et al. 18 identified six-month persistent anemia rates of 52% and one-year anemia rates of 45%. A prospective analysis of 19 patients identified a 53% persistent anemia rate at six months. 7 Differences in our study may be attributable to the overall younger age of trauma patients compared with the critically ill populations studied. Trauma patient median age was 45 years compared with 67 years in both critically ill patient studies.7,18 In this study we demonstrated a functional iron deficiency early after injury, but systemic iron levels improved within two weeks after injury despite a number of patients with moderate-severe anemia. Erythropoietin levels also resolved within one month after injury despite persistence of anemia in most trauma patients. This finding suggests that there is either resistance to erythropoietin or a downregulation of the erythropoietin receptor.
Erythropoietin resistance has been shown to be mediated by hepcidin.19,20 In this study, median hepcidin levels remained elevated throughout the six-month follow-up period and could contribute to erythropoietin resistance.
Previous trials of exogenous iron use for the treatment of anemia of critical illness have been ineffective.15,16 The lack of efficacy in these trials is related to the fact that these patients do not have a true iron deficiency but rather a functional iron deficiency. With the persistent elevation of hepcidin, iron becomes sequestered within macrophages and hepatocytes decreasing systemic levels.19,20 When systemic iron levels are reduced, iron is inaccessible for incorporation into heme molecules within developing erythroblasts. 20 The persistent elevation of hepcidin provides some explanation as to why several clinical trials utilizing exogenous iron or erythropoietin failed to improve hemoglobin levels or decrease transfusion requirements.14–16 There is increasing experimental data to support the pharmacologic modulation of hepcidin for the treatment of anemia.21–23 There is also potential concern that interference with hepcidin could be harmful. Erythroferrone has been documented to inhibit hepcidin. This is the first study to demonstrate elevated erythroferrone levels early after trauma. 24 Erythroferrone levels did not remain elevated throughout the study period and could explain why there was a lack of anemia recovery in these patients.
Injury-associated anemia is also associated with mobilization of hematopoietic progenitor cells from the bone marrow to peripheral blood, suppression of bone marrow erythropoietic progenitor cell growth, and overall reduced bone marrow cellularity.4,21,25 Norepinephrine has been shown to increase G-CSF release. Granulocyte colony-stimulating factor is a key mediator of hematopoietic progenitor cells' egress from the bone marrow niche. In the current study, plasma norepinephrine was elevated for two weeks, and G-CSF was elevated for up to six months after traumatic injury. Previous studies have demonstrated increased G-CSF levels after injury, but none have examined the persistence of its elevation.4,26 In one study, Cook et al. 26 identified a group of severely injured trauma patients with persistent G-CSF elevations lasting ten days after injury, which was associated with lower hemoglobin, increased delayed transfusion requirements, and higher rates of hospital-acquired infections. A 2018 study looking at patients with sepsis identified inverse correlations between circulating inflammatory cytokines in the plasma and hemoglobin on day 14, including IL-6 and TNF-α. 27 These elevations in IL-6 and TNF-α were also seen in our injured patients. These proinflammatory cytokines also inhibit erythropoiesis. Interleukin-6 has a suppressive effect on erythropoiesis.28,29 In addition, persistent inflammation (evidenced in our study by ongoing elevations in both IL-6 and CRP) have been shown to increase hepcidin production.20,30,31 The negative impact of TNF-α on erythropoiesis is multifactorial, involving inhibition of erythroid transcriptional activity, reduction in erythropoietin and stem cell factor-induced colony formation, suppression of erythroid progenitor cell proliferation and maturation, and the induction of erythroid progenitor apoptosis.32–36
Those subjects with prolonged or no anemia recovery were recognized to have had greater infectious complications, and received more packed red blood cell transfusions, and spent more time in the ICU than those who recovered quickly. This is not the first study linking packed red blood transfusions to worse outcomes and suppression of erythropoiesis, despite being the current use of restrictive transfusion strategies.8,10–12,37–39 There were only 12 patients who did not receive any transfusions. This study was intended to identify predictors of lack of anemia recovery after trauma. However, our follow-up was insufficiently powered for additional post hoc subgroup analyses. This is a limitation of the current study. In addition, the long-term follow-up was only 32% at three and six months. Further investigation of those select patients with a prolonged rate of anemia recovery, including a larger follow-up population and assessment of bone marrow erythropoietic activity by measurement of circulating reticulocytes, will allow us to better stratify patients and identify those patients who would require targeted therapy to improve anemia recovery.
Conclusions
In this single-center observational study, anemia was universal after severe traumatic injury. Severe trauma was associated with a prolonged inflammation and an anemia that coincided with persistent inflammation despite elevations in erythropoietin and early improvements in systemic iron levels. This inflammatory response was linked to increased packed red blood transfusions and longer ICU stay. Further analysis is needed to identify targeted anemia management strategies in those trauma patients with persistent anemia.
Footnotes
Acknowledgments
The authors would like to acknowledge Brandi Buscemi, Jillianne Brakenridge, Ruth Davis, Ashley McCray, Jennifer Lanz, and Iverson Williams for their support with project administration and data curation, and specifically for their assistance with coordinating and obtaining follow-up samples.
Authors' Contributions
Conceptualization (lead): Mohr. Conceptualization (supporting): Kelly, Efron.
Data curation (equal): Kelly, Munley. Investigation (equal): Munley, Kannan, Pons. Investigation (supporting): Coldwell, Bible, Parvataneni, Hagen. Formal analysis: Kelly. Methodology (lead): Mohr. Methodology (supporting): Kelly, Kannan. Visualization: Kelly. Writing–original draft (lead): Kelly. Writing–review and editing (lead): Kelly. Writing–original draft (supporting): Munley, Mohr. Writing–review and editing (supporting): Munley, Pons, Coldwell, Bible, Mohr.
Supervision (lead): Mohr. Supervision (supporting): Efron. Funding acquisition: Mohr.
Funding Information
This work was supported by the National Institutes of Health [R01 GM105893, T32 GM-008721]. A.M.M. was supported by NIH NIGMS R01 GM105893. L.S.K. and J.A.M. were supported by post-graduate training grant T32 GM-008721 in burns, trauma, and peri-operative injury by NIGMS.
Author Disclosure Statement
The authors declare that they have no relevant conflicts of interests.