
Abstract

Acute inpatient healthcare for medical and surgical conditions is complicated by infections related to multi-drug–resistant organisms (MDRO). 1 Accordingly, substantial and system-wide efforts are directed at addressing MDRO prevention, identification, and management. Infection control (IC) committees, IC advanced practice providers, antibiotic utilization committees, and antimicrobial stewardship committees all focus on care that influences MDRO prevention, evolution, spread, and eradication. 2 Multi-drug–resistant organism infection often drives infectious disease consultation for acute therapy (including access to formulary restricted therapeutics), monitoring, de-escalation, and termination as care often exceeds the duration of acute inpatient care. 3 Furthermore, such patients are often identified within the electronic health record (EHR) to help guide clinical care including isolation practices.
Accordingly, the inpatient setting is replete with policies, protocols, data streams, and performance improvement projects to enhance IC practices (Fig. 1). These efforts interdigitate with successful infection resolution, which for surgical patients integrates empiric followed by therapeutic antimicrobial therapy coupled with source control. 4 These efforts anticipatedly alter the host microbiome, which may have been already transformed into a pathobiome under the influence of the surgical disease process and luminal nutrient deprivation. 5 These microbiome alterations predictably impact the skin microbiome, an event that is generally not addressed with regard to surgical site infection prophylaxis when repeated intervention is required, even if a MDRO developed during the patient's index admission. These microbiome shifts may be particularly relevant for those requiring open wound management after injury or emergency general surgery (EGS) whether addressed by packing or negative pressure wound therapy (NPWT). These care elements are important during survivorship as patients leave the acute care facility.
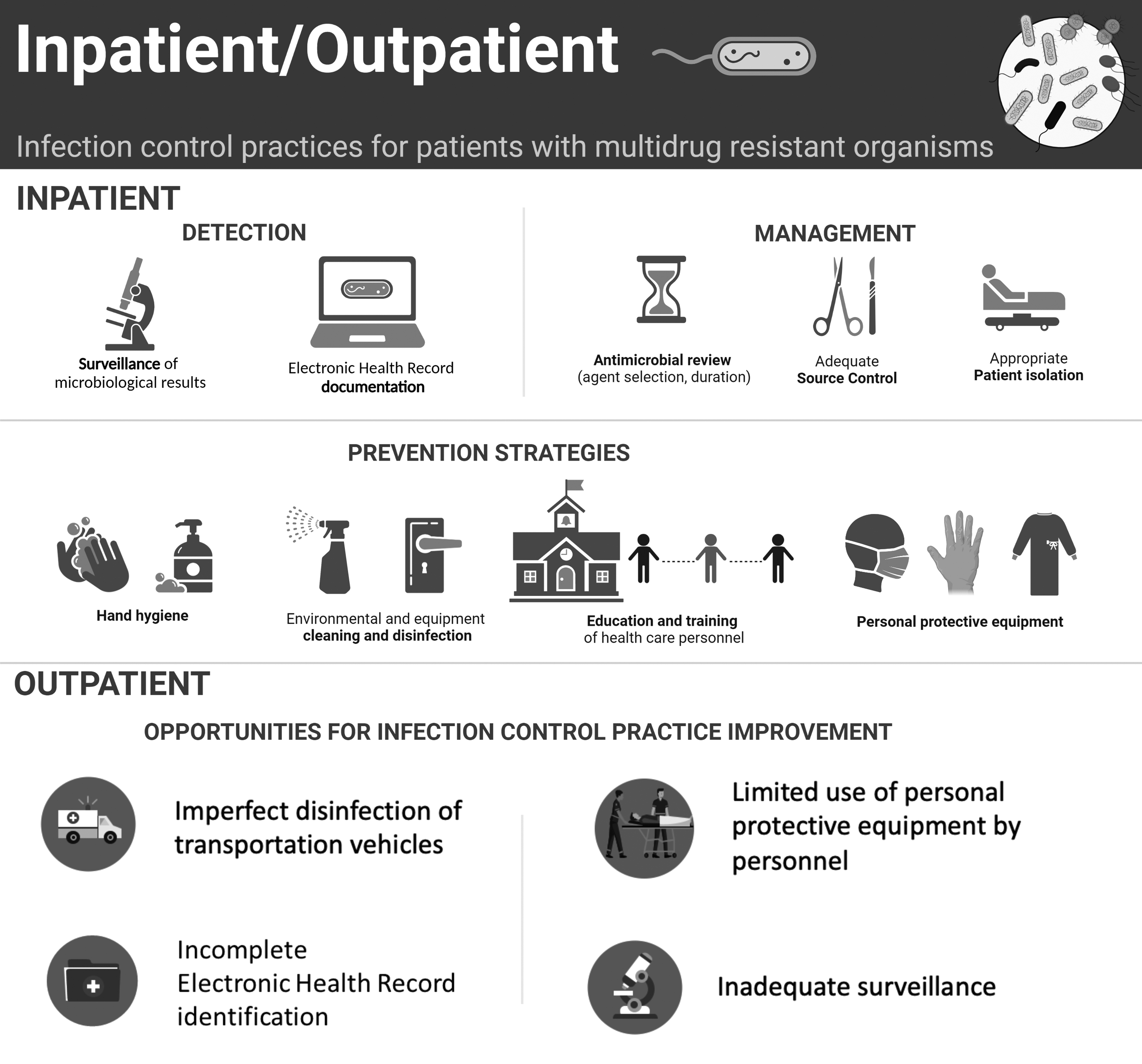
This image depicts how infection control practices widely diverge between the inpatient and outpatient spaces, including during interfacility transport.
Despite such attention, the inpatient setting is fraught with IC failures including those related to personal protection equipment (PPE) use, but especially hand hygiene. 6 The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic highlighted IC practices, but also outlined the value of a “dofficer” for safe PPE removal. 7
After life-threatening injury or illness, survivorship commonly leads to transfer to another site for care including a long-term acute care facility or other specialty facility; home repatriation is less common. When patients bear a MDRO, this transition initiates exposure of the larger environment to MDRO. Interfacility patient transport occurs most commonly by ambulance. Unlike the inpatient setting, the policies and procedures that address transport of patients who were in isolation during acute inpatient care are less clear and may be variable between transport services. 8
The use of gowns by ambulance personnel is similarly non-uniform, and clothing may serve as a vector for infection transmission. The completeness of rig disinfection is likely operator dependent. These aspects may be important when the rig is used to transport an immune incompetent individual following the transport of a MDRO-bearing patient, especially one with an open wound where wound dressing integrity may not be intact. Furthermore, infection transmission in this setting is under-surveilled and represents an opportunity for improvement. Interfacility transport is not the sole setting of potential transmission. Acute ambulance rescue may also unwittingly convey MDRO-bearing patients to an acute care facility. Those crews and their rigs may suffer from the same challenges as those used for interfacility transport. Moreover, rig disinfection, when not visibly soiled, may be more superficial when the crew is needed for another emergency.
The evolving practice of police transport after firearm injury raises similar concerns regarding the Police vehicle and the officer who may come into contact with a wide variety of individuals throughout their shift; violence recidivism may credibly occur in a patient with a MDRO supporting microbiome after surviving a life-threatening prior injury.
The outpatient space is similarly unaligned with inpatient isolation and IC practices. Regardless of the presence of an MDRO-bearing patient (with or without an open wound), all patients use the same waiting room and clinic examination rooms. If there are disparate EHRs or unlinked inpatient and outpatient charts, there may be no way to identify patients with MDRO ahead of their arrival and their medical history recall. Unsurprisingly, isolation gowns are infrequently present in clinic spaces. Accordingly, patients are not sequenced to group those with known open wounds with or without known MDRO, nor are they cared for in specific rooms with enhanced disinfection between patients. Common practices including wiping the examination table with a disinfecting cloth and changing the examination table paper; chairs and other high contact surfaces are often omitted. 9 As for ambulance transport, transmission in this setting is undersurveilled between patients, as well as between patient and clinician. Relatedly, zoonotic transmission from emotional support animals (when allowed in the clinic space) is undersurveilled; service animals are unlikely vectors as required badging helps preclude contact. 10 Clearly there is an opportunity for both policy and practice realignment between care spaces.
There are anticipatable impacts of changing policy and practice across each of these settings. These include, but are not limited to, supply costs, decreased patient flow related to disinfection practices and space constraints for those requiring ambulance transport, as well as additional scheduler time to group patients. Presently, the clinical relevance of so doing remains unclear but the anticipated benefits are intuitively attractive for controlled settings. Nonetheless, the patients who would be impacted by these practices may also visit uncontrolled settings throughout the community devoid of between use disinfection (i.e., restaurants, gas stations, supermarkets).
Therefore, it is reasonable to advocate for the following practice changes. First, secure data regarding IC practices as well as open wound and MDRO bearing patient volume in each of the aforementioned settings. Second, all such patients should be easily EHR identifiable using flags or banners. Third, clinicians should leverage the smartphone medical ID app to enter data so that during emergencies, or care rendered in a non-native system, key information is available to pre- and in-hospital clinicians; the app can be opened without needing to unlock the phone. Fourth, IC practices and infection transmission should be surveilled in the outpatient and transfer settings with the same vigor as the inpatient setting. This presents a unique opportunity for collaboration and facility outreach to support community health and wellness.
Footnotes
Authors' Contributions
Conceptualization: Bass, Somodi, Dzierba, Kaplan. Data curation: Kaplan, Bass. Visualization: Dzierba. Writing–original draft: Kaplan. Writing–review and editing: Bass, Somodi, Dzierba, Kaplan.
Funding Information
No funding was received for this work.
Author Disclosure Statement
Dr. Kaplan is a past president of the Society of Critical Care Medicine (2020–2021). Dr. Kaplan is in part, a federal employee. The views expressed within this commentary are independent and do not reflect views, opinions, or policies of the U.S. federal government. No other authors have any disclosures.