
Abstract
Background:
This study aimed to establish a threshold of C-reactive protein (CRP) level for early detection of post-operative infectious complications after surgery for colorectal cancer.
Patients and Methods:
In this single-center, retrospective analysis, we studied the data of 178 patients who underwent surgery for colorectal cancer between January 2018 and February 2022. Elective surgery with curative intent was performed, and serum CRP levels were measured on five consecutive days after surgery. Receiver operating characteristic curves were utilized to assess the cutoff point of the CRP level with maximum predictive value,
Results:
A total of 59 cases of early post-operative complications, including pneumonia, wound infection, intra-abdominal infection, and anastomotic leakage were evaluated. During the monitoring period, patients with complications had higher CRP level than those without complications. The cutoff points on the five post-operative days were estimated to be 6.50, 10.83, 11.44, 6.67, and 5.71 mg/dL, respectively, and they were correlated to the occurrence of infectious complications. Higher CRP levels were associated with greater blood loss during surgery (p = 0.003) and increased length of hospital stay (p < 0.001) than did lower CRP levels.
Conclusions:
C-reactive protein monitoring in the early post-operative period is a cost-effective test that can be easily performed to predict the occurrence of infectious complications. It may be helpful in improving surgical outcomes, shortening the length of hospital stay and appropriate antibiotic administration.
The rate of overall morbidity, including infectious complications, after colorectal surgery is approximately 30%, and the 30-day post-operative mortality rate is approximately 3% to 4% in several studies.1-3 Among infectious complications, anastomotic leaks are the most serious and the main reason for high post-operative morbidity.4,5 Therefore, early identification of an anastomotic leak could help avoid sepsis and prevent mortality. Many studies have shown that measuring the levels of C-reactive protein (CRP), which is an acute phase protein, to detect the magnitude of systematic inflammatory response can help predict the occurrence of postoperative infectious complications.6-12 The concentration of CRP in the blood is associated with infectious complications in patients who undergo surgery for cancer and infection. In particular, increased CRP concentrations are associated with the risk of infectious complications, including anastomotic leaks, during the post-operative period in patients who undergo colorectal surgery. Matthiessen et al. 13 reported that serum CRP level is a strong indicator of anastomotic leakage in patients undergoing anterior resection for rectal cancer. Moreover, Korner et al. 14 found that the concentration of serum CRP increased on post-operative day (POD) 3, and there is a relation between CRP levels and intra-abdominal infections. A recent study demonstrated that the concentration of serum CRP in a patient with anastomotic leaks after colorectal surgery increased on POD 4, and the optimal predictive threshold value was 18.0 mg/dL.
Although an association between the incidence of post-operative infectious complications and CRP has been identified, there is no clarity regarding the POD on which CRP measurement would be most predictive and the optimal threshold concentration of CRP that would enable prediction of infectious complications. Therefore, the aim of this study was to evaluate the significance of CRP as a predictive tool for postoperative complications, which in turn may help appropriate antibiotic administration after resection for colorectal cancer. Furthermore, depending on the elevation of CRP concentrations, abdominal computed tomography (CT) scans may be performed to facilitate timely identification of complications and safe, early discharge.
Patients and Methods
The study was reviewed and approved by the Ewha Womans University Mokdong Hospital Institutional Review Board (IRB File No: EUMC 2022-06-002). In this retrospective cohort, single-institution study, we evaluated the data of patients who underwent colon resection surgery for colorectal cancer from January 2018 to February 2022 at the Ewha Womans University Mokdong Hospital. A total of 357 patients with colorectal cancer underwent therapeutic surgery or abdominal colon resection. After excluding patients who underwent emergency surgery or procedures involving other organs, were in a subconscious state during surgery, and had metastatic or inflammatory disease, 178 patients were finally included in the study. The basic patient characteristics that were considered were gender, age, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status classification system score, hospitalization period, surgery date, discharge date, diagnosis name, surgery name, CRP concentration, and white blood cell (WBC) count on POD 1–5, and nature of complications.
Prophylactic antibiotic agents are administered within one hour before surgery and discontinued within 24 hours after surgery. Serum CRP levels were measured on five consecutive days after surgery; patients whose data were not obtained during these days were excluded. The association of CRP levels with post-operative complications was confirmed using the daily CRP values and the highest CRP value. Receiver operating characteristics (ROC) curves were used to evaluate the cutoff CRP value at which maximum prediction was possible. In addition, clinical parameters, including temperature (central temperature >38°C indicated fever), pulse rate, abdominal signs, bowel movements, and volume and aspects of drainage fluid, as well as CT scans and medical records were monitored during hospital stay to evaluate the occurrence of infectious complications. Patients were categorized into two groups based on whether or not they had infectious complications. The complications were further classified as infectious and non-infectious.
Post-operative infectious complications were defined as any septic event occurring after colorectal resection and included intra- and extra-abdominal infections as well as surgical site infections. 15 Surgical site infections were diagnosed based on the presence of clear signs of inflammation with purulent drainage from the wound. Anastomotic leakage and intra-abdominal infection were defined as the observation of a leak at the anastomosis or fluid collection due to complicated intra-abdominal infection on post-operative CT scans.
Pneumonia was diagnosed based on pulmonary infiltration observed on chest CT scans or radiographs accompanied by clinical symptoms or on physical or laboratory examination. Urinary tract infection (UTI) was identified based on positive urine sediment analysis combined with leukocytosis and/or fever. 16
Statistical analysis was performed using PASW Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY). Clinicopathological characteristics were compared between the groups of patients with and without complications using the χ 2 test or t-test. The predictive ability of CRP was assessed using ROC curve analysis. The area under the curve (AUC) was considered a direct measure of the diagnostic accuracy of the test. An AUC value >50% indicated the ability of a test to discriminate between positive and negative cases with regard to the classification variable. A test with an AUC >0.75 was considered as having a high diagnostic accuracy and indicated that at least 75% of the patients with the disease were classified correctly. A p value <0.05 was considered statistically significant.
Results
The data of 178 patients were analyzed in this study. Their baseline characteristics are shown in Table 1. The mean age of the patients was 68.8 (range, 14–94) years, and 98 (55.1%) of the patients were male. The mean BMI was 23.8 kg/m2, and mean length of post-operative hospital stay was 13.2 days. There were 119 patients (66.9%) with colon and 59 patients (33.1%) with rectum. A total of 51 patients demonstrated infectious complications (Table 1 and 2) that were 59 in number, including eight cases of duplicate complications; four, anastomotic leakage (2.2%); 11, intra-abdominal infections (6.2%); 14, pneumonia (7.9%); 26, wound infections (14.6%); and four, UTI, colostomy necrosis, and pseudomembranous colitis (2.1%).
Baseline Characteristics
Data are given as number of cases (%). Continuous variables were given as median (range).
BMI = body mass index; ASA = American Society of Anesthesiologists; EBL = estimation of blood loss; CRP = C-reactive protein; OP = operation.
Types of Complications and Their Incidence
UTI = urinary tract infection; PMC = pseudomembranous colitis.
Comparison of the two groups of patients with and without infectious complications showed that the frequency of infectious complications was not significantly correlated with gender, ASA physical status classification system score, BMI, operation time, and estimated blood loss (EBL). However, age and length of hospital stay were significantly associated with the occurrence of infectious complications (Table 1).
Analysis of the average CRP levels from POD 1 to POD 5 (Fig. 1), showed no difference between the two groups on POD 1 (5.97 mg/dL vs. 6.69 mg/dL; p = 0.293). However, there was a difference in CRP between the groups from POD 2 onward and the day on which highest CRP concentration was measured (Table 3; POD 2: 10.20 mg/dL vs. 12.96 mg/dL; p = 0.004; POD 3: 8.68 mg/dL vs. 13.81 mg/dL; p < 0.001; POD 4: 10.20 mg/dL vs. 12.96 mg/dL; p < 0.001; POD 5: 10.20 mg/dL vs. 12.96 mg/dL; p < 0.001; day on which highest CRP concentration was measured: 10.20 mg/dL vs. 12.96 mg/dL; p < 0.001).
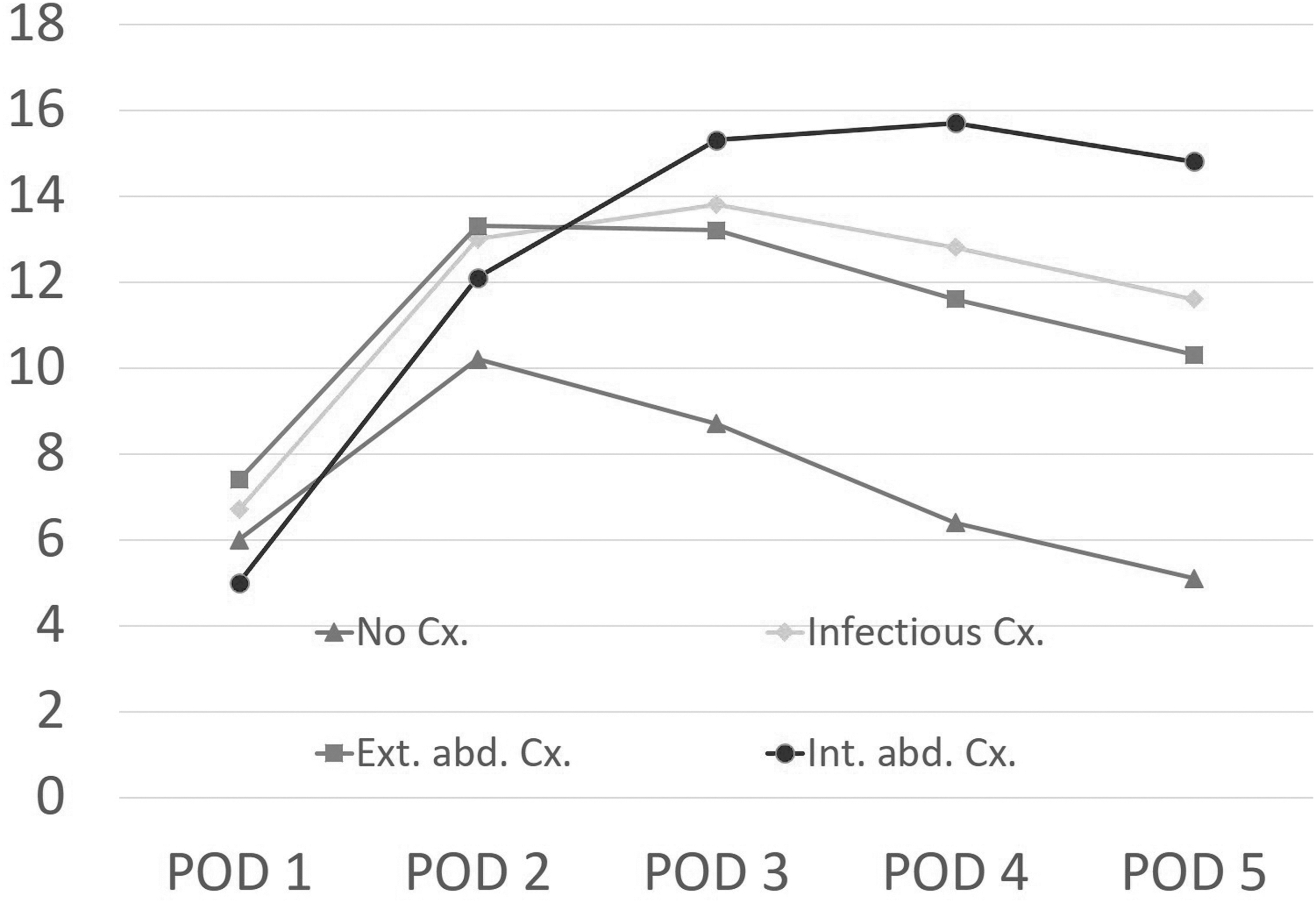
Serum C-reactive protein (CRP) levels in patients with and without infectious complications. In addition to infectious complications, both extra-abdominal complications and intra-abdominal complications had significantly higher serum CRP levels compared with no complications. POD = post-operative day; infectious Cx = infectious complications; Int abd Cx = intra-abdominal complications; Ext abd Cx = extra-abdominal complications.
Mean CRP Levels in Patients With and Without Infectious Complications on POD 1–5
CRP = C-reactive protein; POD = post-operative day; Infectious Cx = infectious complications; Int abd Cx = intra-abdominal complications; Ext abd Cx = extra-abdominal complications.
The complications were analyzed by dividing them into two groups. The groups of patients who had no complications, intra-abdominal complications, and extra-abdominal complications were further evaluated. There were significant differences among them on POD 3–5 (Table 3). Furthermore, the WBC counts were higher on POD 1–5 in the infectious complications group than in the no infectious complications group.
Figure 2 presents the ROC plots for the diagnostic accuracy of CRP levels in predicting infectious complications between POD 1 and POD 5. The AUC, cutoff value, sensitivity, specificity, and predictive values for POD 1–5 and on the day CRP concentration was maximum are shown in Table 4. The CRP value measured on POD 5 (5.7 mg/dL; AUC, 0.825) had the highest diagnostic accuracy. On applying the cutoff value of 5.7 mg/dL for CRP on POD 5, the sensitivity was found to be 82.4%; specificity, 70.9%; positive predictive value, 53.2%; and negative predictive value, 90.9%
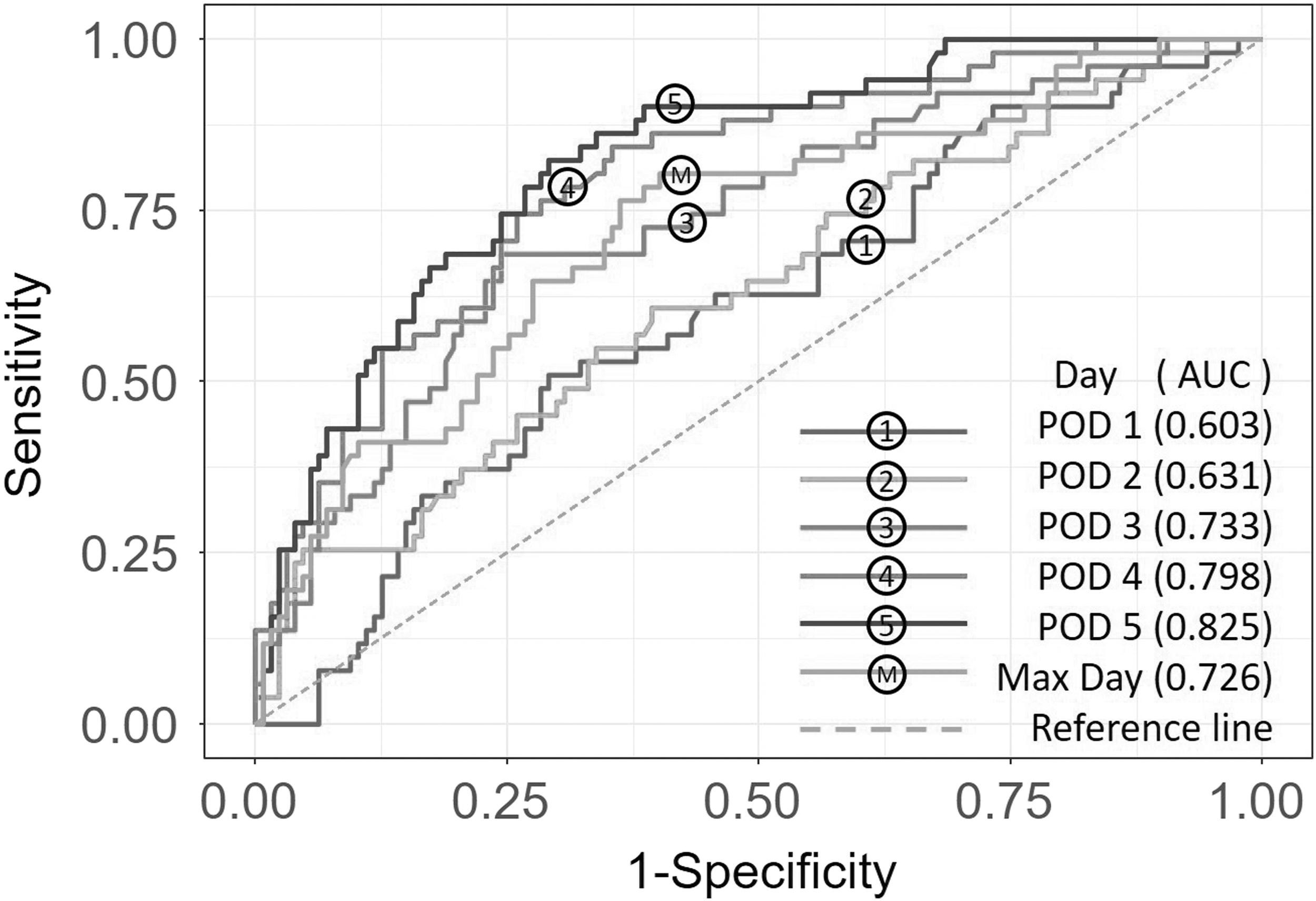
Association of C-reactive protein (CRP) levels with development of infectious complications after surgery for colorectal cancer. The area under the curve (AUC) value on post-operative day (POD) 5 is 0.825.
Receiver Operating Characteristics Curve Analysis of CRP as a Marker for Post-Operative Infectious Complications
CRP = C-reactive protein; AUC = area under the curve; POD = post-operative day.
Patients were classified into two groups according to the CRP cutoff level; the incidence of infectious complications was higher in the high CRP group than in the low CRP group (53.2% vs. 9.1%; p < 0.001). The high CRP group not only exhibited longer length of hospital stay (16.1 days vs. 11 days; p < 0.001) but also higher EBL during surgery (227.5 mL vs. 131.2 mL; p = 0.003) than did the low CRP group (Table 5).
Comparison Between Low and High CRP Groups on Post-Operative Day 5
CRP = C-reactive protein; BMI = body mass index; ASA = American Society of Anesthesiologists; OP = operation; EBL = estimated blood loss.
Figure 3 presents the correlation coefficients using Pearson pro coefficient analysis. A correlation is observed between infectious complications and CRP values on POD 5. Furthermore, a correlation exists between EBL and operation (OP) time.
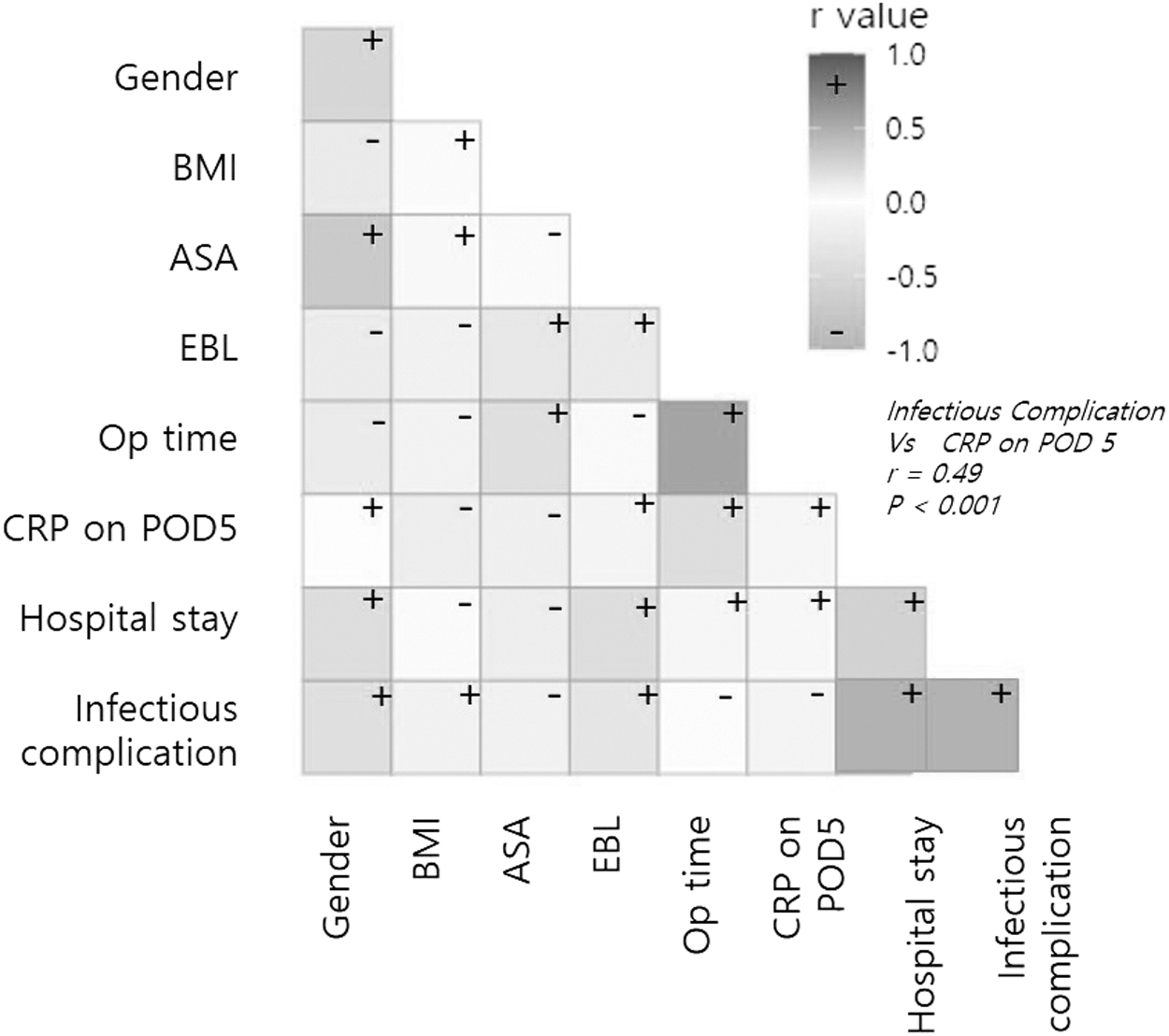
Correlation coefficients using Pearson pro coefficient analysis. A significant correlation is observed between infectious complications and C-reactive protein (CRP) values on post-operative day (POD) 5. Furthermore, a correlation exists between estimated blood loss (EBL) and operation (OP) time.
Discussion
C-reactive protein is an inflammatory marker in the blood that was first described by Tillet and Francis 17 in 1930. 18 The concentration of this acute phase protein, which has a short half-life of 19 hours, 19 increase between four and 10 hours after inflammatory stimulation, reaches peak concentration in the plasma at 48 hours, and returns to the baseline value after inflammatory stimulation is stopped. C-reactive protein can be measured easily and quickly; therefore, it is a reliable marker that is commonly tested in infected and surgical patients to detect the intensity of stimulation during acute inflammatory reactions. Furthermore, unlike clinical signs (vital signs), such as fever, tachycardia, and pain, or the response rate to low WBC counts, CRP begins to increase before post-operative infectious complications occur. 18 In patients with colorectal cancer, CRP is a useful indicator of the severity of infectious complications, such as anastomotic leaks and intra-abdominal infections. 18
The incidence of infectious complications after surgery is reported to be 20% to 40% after colorectal surgery.1,2,9,20 Despite the prophylactic use of pre-operative antibiotic agents, many infectious complications occur after colorectal surgery. Anastomotic leaks account for 2% to 14% of the complications7,21; this has not decreased despite advances in surgical technology and the development of pre-operative treatment. This morbidity has an impact on prognosis as well as functional and oncological outcomes. Other infectious complications may not only affect recurrence rates and prognosis but may also increase the length of hospital stay and treatment costs. 12 Currently, early discharge facilitated by the post-operative fast-track protocol system that helps reduce medical costs and improve patient outcomes is preferred. Nevertheless, very early discharges are potentially associated with an increased risk of a delayed diagnosis and treatment of postoperative infectious complications that occur after discharge. Delayed diagnosis is also known to increase mortality by 18%. 22 Therefore, early detection of developing complications after colorectal surgery and prompt treatment are mandatory for reducing post-operative morbidity and improving long-term outcomes.
Many studies have shown that patients with anastomotic leakage or infectious complications have higher postoperative CRP values than those without complications.6,7 Therefore, continuous post-operative CRP value monitoring can help predict the occurrence of post-operative complications. Although several studies have suggested that an abnormally elevated CRP value or persistent elevation of CRP may be a useful predictor of infectious complications, 10 a clear cutoff point has not yet been determined. Various CRP cutoff values ranging from 9.4 to 19.0 mg/dL have been reported depending on values measured on POD 3–5 as a threshold for predicting anastomotic leakage or infectious complications.8,10,14 However, measuring CRP in asymptomatic patients is considered inappropriate; moreover, CRP measurements are not often taken because of factors related to insurance and cost. Additionally, standard predictors of infectious complications have not yet been established. Therefore, we analyzed the significance of CRP as a warning marker and the validity of continuous CRP monitoring to determine the requirement for antibiotic administration or abdominal CT examinations when CRP concentrations are elevated and determined the CRP threshold value. This would facilitate the performance of early abdominal CT scanning, if necessary, or the timely administration of appropriate antibiotics for therapeutic purposes in cases where there are no other clear causes for CRP elevation after surgery.
The outcomes of patients suspected of having inflammatory complications after colon surgery can be significantly improved by providing pre-emptive antibiotic treatment. A previous study has also shown that preemptive antibiotic therapy can significantly improve outcomes in patients with inflammatory complications after colorectal surgery. 23
Early detection of complications would not only contribute to improved prognosis and oncologic outcomes but also allow safe and early discharge. In cases of anastomotic leakage, early detection before clinical signs appear can reduce patient morbidity and play an important role in preserving anastomotic sites. However, we found that some complications, such as wound infection and pneumonia, did not require abdominal CT scanning for detection. Thus, relying on imaging tests is not feasible in all patients even if the CRP value exceeds the threshold level and may be avoided to prevent increased false negative results, exposure to excessive radiation, and unnecessary expenses. Abdominal CT scanning may be useful in cases where no clear causative lesions were observed on clinical examination. Moreover, we confirmed that the negative predictive value was high, which meant that there was a high possibility that complications would not have occurred if the CRP concentration did not rise above the threshold value. Therefore, unnecessary tests were not performed, and safe, early discharge of the patients was possible.
Additionally, we determined the cutoff values with the highest diagnostic accuracy on each POD through ROC analysis. Statistically, the CRP values obtained on POD 5 had the most reliable thresholds. Nevertheless, our results indicated that in patients undergoing colorectal resection, serial postoperative CRP measurements after POD 3 may contribute to early identification of infectious complications related to anastomotic leakage.
Despite these findings, our study had some limitations. First, because of the retrospective nature of the study, the severity of each complication could not be determined from past medical records that might have been subjected to omission or prejudice. Second, patients whose five-day CRP data were not available were excluded from the study; therefore, the number of patients who had complications was low. Prospective studies including more patients are required to obtain more accurate and reliable results.
Conclusions
Considering this is a single-institution study, the findings are reliable enough to be regarded for protocols related to patient management, surgical skill, and confirmation of complications. Additionally, the detailed analysis of complications revealed that CRP was significantly higher in patients with extra-abdominal infections as well as in those with intra-abdominal infections, including anastomotic leakage, than in those without complications. Therefore, CRP is a useful marker for early detection of infectious complications.
Evaluating CRP concentrations after colorectal surgery proved useful in predicting post-operative infectious complications. We also determined the cutoff values of CRP for each postoperative day. In cases in which the CRP concentration is above the cutoff value or the CRP concentrations are persistently high, early imaging studies should be considered to exclude the possibility of infectious complications, such as wound infection, pneumonia, and anastomotic leakage. Early detection of infectious complications using CRP measurements reduces morbidity and facilitates early discharge of patients after colorectal surgery.
Footnotes
Authors' Contributions
Conceptualization: Lee, Noh, Chung, Kim. Data curation: Nam.
Formal analysis: Nam, Noh. Investigation: Nam. Methodology: Nam, Noh.
Writing—original draft: Nam, Lee.
Funding Information
No funding was received.
Author Disclosure Statement
None of the authors have any conflicts of interest.