
Abstract
To the Editor:
P
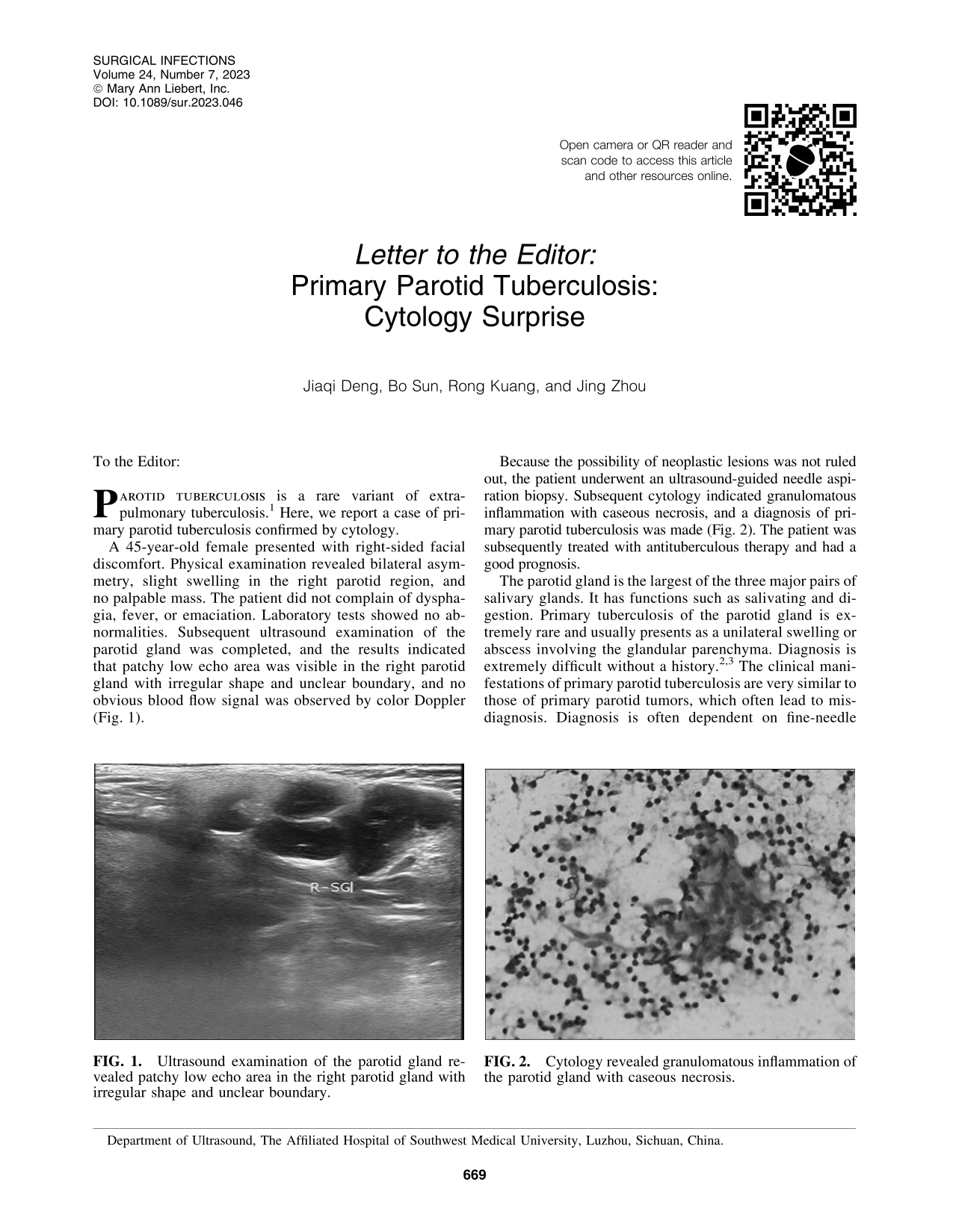
A 45-year-old female presented with right-sided facial discomfort. Physical examination revealed bilateral asymmetry, slight swelling in the right parotid region, and no palpable mass. The patient did not complain of dysphagia, fever, or emaciation. Laboratory tests showed no abnormalities. Subsequent ultrasound examination of the parotid gland was completed, and the results indicated that patchy low echo area was visible in the right parotid gland with irregular shape and unclear boundary, and no obvious blood flow signal was observed by color Doppler (Fig. 1).
Ultrasound examination of the parotid gland revealed patchy low echo area in the right parotid gland with irregular shape and unclear boundary.
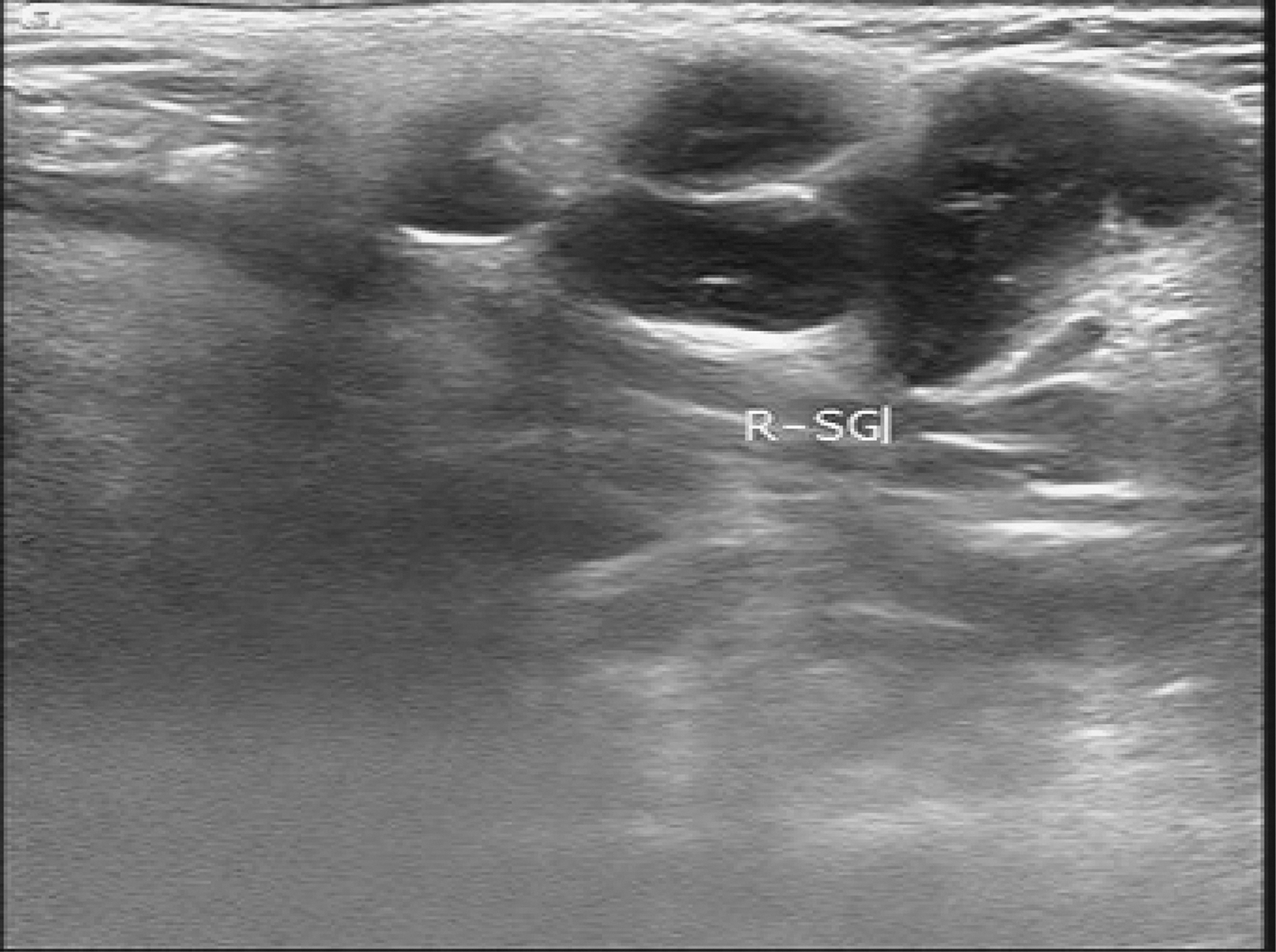
Because the possibility of neoplastic lesions was not ruled out, the patient underwent an ultrasound-guided needle aspiration biopsy. Subsequent cytology indicated granulomatous inflammation with caseous necrosis, and a diagnosis of primary parotid tuberculosis was made (Fig. 2). The patient was subsequently treated with antituberculous therapy and had a good prognosis.
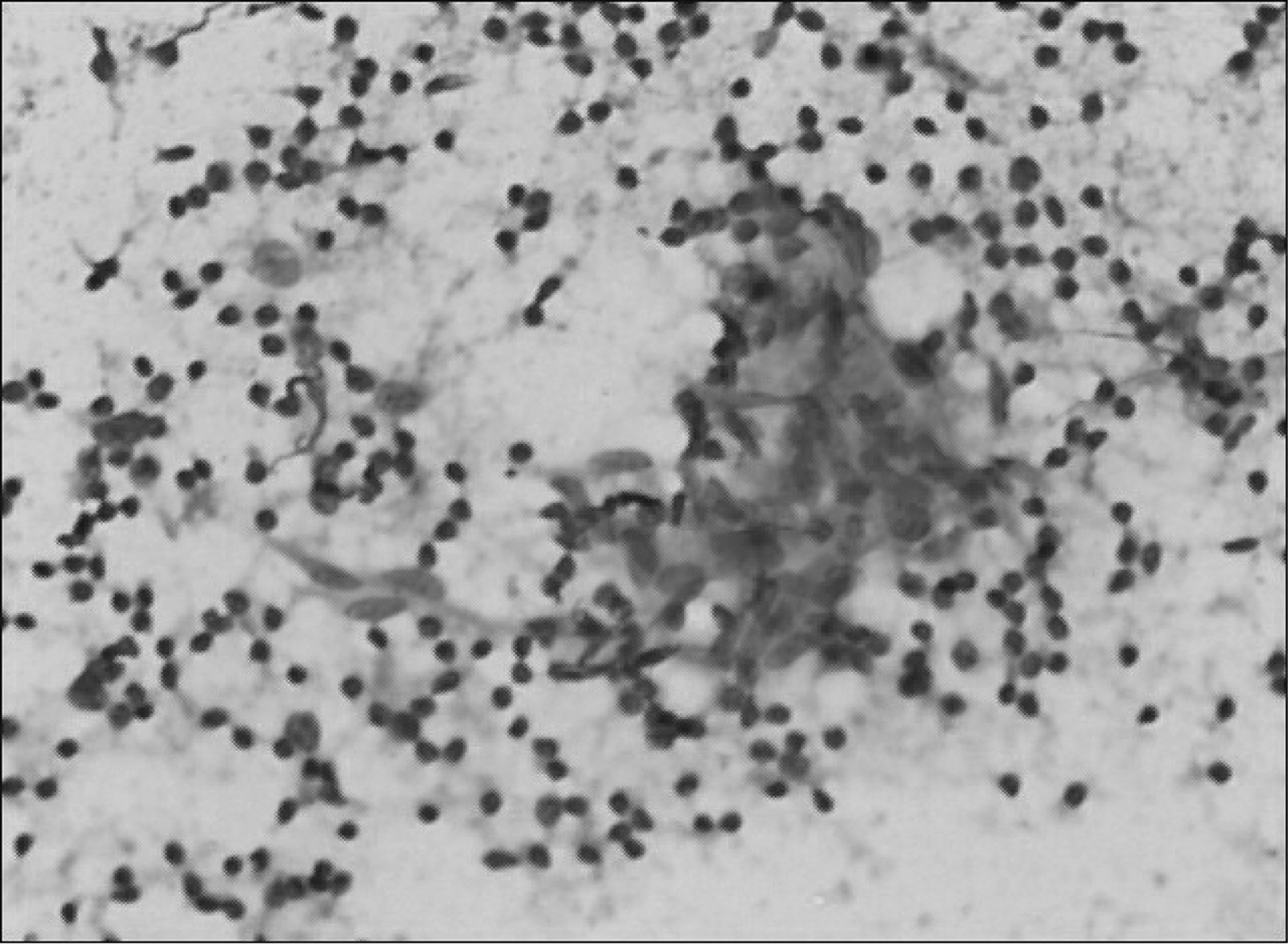
Cytology revealed granulomatous inflammation of the parotid gland with caseous necrosis.
The parotid gland is the largest of the three major pairs of salivary glands. It has functions such as salivating and digestion. Primary tuberculosis of the parotid gland is extremely rare and usually presents as a unilateral swelling or abscess involving the glandular parenchyma. Diagnosis is extremely difficult without a history.2,3 The clinical manifestations of primary parotid tuberculosis are very similar to those of primary parotid tumors, which often lead to misdiagnosis. Diagnosis is often dependent on fine-needle puncture biopsy or post-operative histopathologic examination. Because parotid tuberculosis responds well to antituberculosis treatment, once diagnosed, antituberculosis treatment should administered to avoid complications such as abscess and even facial ulceration caused by tuberculosis progression. The past history is an important clue for the diagnosis of parotid tuberculosis, and the patient's past infection history should be examined in detail. Because of the good prognosis of this disease, when the diagnosis is uncertain, further cytologic examination by fine-needle puncture can be performed to confirm the diagnosis, so as to avoid unnecessary surgical intervention.