
Abstract
Background:
Nosocomial and health-care–associated infections drive increased healthcare costs and negatively affect patient outcomes. The human microbiome has been heavily explored in recent years with incomplete data regarding hospital-specific and community-specific microbial communities. Although bacterial species differ between intensive care units in the same hospital, it is unclear if they differ between similar units in similar hospitals in the same community. Our hypothesis is that pathogens in surgical intensive care units (SICUs) are distinct between hospitals, even in the same community.
Methods:
From 2017 to 2021, data were collected prospectively from the SICUs of two 400-bed hospitals located three miles apart in the same city (Hospital A and Hospital B). Infections defined using U.S. Centers for Disease Control and Prevention (CDC) criteria were recorded for trauma and general surgery patients, as well as patient demographics, Acute Physiology and Chronic Health Evaluation (APACHE) II score, and causative organism.
Results:
Overall, Escherichia coli was the most commonly isolated pathogen in Hospital A, whereas Staphylococcus aureus was most commonly isolated at Hospital B. Enterococci were more common in Hospital A, and Haemophilus influenzae and Enterobacter spp. were more common in Hospital B. After stratification between trauma and non-trauma patients, however, these differences disappeared, with the exception of more overall gram-positive organisms and fewer gram-negative organisms among Hospital A trauma patients compared to Hospital B. There were no differences in rates of isolation of either fungi or resistant bacteria between hospitals.
Conclusions:
At a species level, admission diagnosis appears to be a greater determinant of pathogen isolation than hospital when comparing similar intensive care units (ICUs) in the same geographic area, but a larger body of data is needed to flesh out a distinct microbial map of the organisms occupying a certain geographic region. Further areas for investigation include comparison between hospital units, specific anatomic sites, and ICU versus floor patients.
Antibiotic resistance has been an ongoing struggle throughout history. As micro-organisms grow increasingly resistant to the spectrum of antibiotic agents regularly used in hospitals through further exposure, the standard treatment regimen escalates in kind. Depending on the methodology used, the estimation of the annual cost of antibiotic resistance is up to $35 billion in lost productivity and associated healthcare cost. 1 Patients are negatively affected when they contract a resistant organism or develop one through antibiotic exposure, as the cost of their hospital stay increases by an estimated $1400. The healthcare system is in turn impacted by longer intensive care unit (ICU) stays, possible closure of areas for quarantine/isolation, and the cost of increasingly complicated antibiotic regimens. 2
The community of microbes that colonize both humans and their environment is incredibly distinct while also being constantly mutable. The community inside a hospital room has been shown to change based on the individual patient occupying that room, with areas of patient contact being most similar to the skin flora of that patient. 1 However, the hospital microbiome itself has been shown to be relatively homogenous, with the predominance of a few taxa.3,4 If the microbiome of a hospital can be elucidated and potential pathogens can be determined, it could assist in creating individual antibiotic regimens. However, the question remains about generalizability between like environments.
Pathogens differ somewhat between intensive care units in the same hospital, 5 but it is unclear if there is a similarity between similar units in distinct yet similar hospitals. With the ability to understand the microbiome of individual units more comprehensively, preventing and treating hospital-acquired infection would become more streamlined. Presenting hospital-acquired infections would likely fall within the hospital's typical microbiome, allowing for tailoring of empiric antibiotics toward the hospital's microbiome and possibly measures to target eradication of known pathogens in the microbiome. Knowledge of the potential pathogens could also lead to a more tailored antibiotic regimen and decrease resistance in turn. Our hypothesis is that pathogens in surgical intensive care units (SICUs) are distinct between hospitals, even in the same community.
Methods
From 2017 to 2021, data were prospectively collected from two approximately 400-bed hospitals located three miles apart in the same city, labeled as Hospital A and Hospital B. Both hospitals have similar amounts of indigent patients (20%–25%, per hospital sources) with slight differences in age and trauma volume, but overlapping catchments. The hospitals share residents, but only a limited number of faculty (one surgical intensivist works at both hospitals). Nurses and other personnel are not shared between facilities. Although of similar size and both openly serving the same geographic area, based on traditional referral patterns, the populations are somewhat different, with one hospital serving higher numbers of psychiatric and neurologic disease patients, whereas the other has a larger trauma population and an embedded children's hospital. One hospital is an American College of Surgeons-verified level 1 trauma center, and one is a level 2 center. For this reason, those two populations (trauma and non-trauma) have been separated for analysis. Only patients on the general surgery and trauma surgery services were included in this data set; other surgical patients were excluded.
All surgical patients over 18 years of age were eligible for inclusion, including those from both the general surgery and trauma surgery services. Infections meeting U.S. Centers for Disease Control and Prevention (CDC) criteria were recorded, including patient demographics, causative organism, primary diagnosis and operation, and Acute Physiology and Chronic Health Evaluation (APACHE) II score. Data were compared between hospitals, including overall incidence of different organisms and resistance rates. During the study period, both hospitals used the VITEK® 2 system by bioMérieux (Marcy-l'Étoile, France) for microbial identification and susceptibility testing. Means were compared using the Student t-test, and proportions were compared using Fisher exact test or χ 2 as appropriate.
Antibiograms for the year 2021 were obtained from both hospitals. For Hospital A, isolates from the critical care units were tabulated; for Hospital B, only system-wide antibiograms were available. This research was deemed exempt by the Western Michigan University Institutional Review Board (ID number WMed-2022-0857).
Results
Demographics for patients in the two hospitals are given in Table 1. Because a difference in representation of trauma versus non-trauma patients was noted because Hospital B has a higher trauma volume, data are categorized by those two groups. Although the two hospitals have similar size SICUs, Hospital A admits a higher percentage of general surgery patients, whereas Hospital B admits a higher percentage of trauma patients. After categorization, no differences were found. On initial analysis there appeared to be a statistically significant difference between trauma and non-trauma patients (p < 0.0001), but when both trauma and non-trauma were further stratified by APACHE II score these differences disappeared.
Patient Demographics Between Hospital A and Hospital B, Stratified by Trauma Versus Non-Trauma Diagnosis
Percentages rounded to nearest whole number. There were no statistically significant differences between the hospitals overall or for each subgroup.
APACHE II = Acute Physiology and Chronic Health Evaluation II.
Mean ± standard error of the mean (SEM).
Table 2 gives the site of infection, also stratified by hospital and trauma diagnosis. The abdomen was the most common site at Hospital A (37%) but among trauma patients, lung infections were most common at 51%. Hospital B, however, demonstrated the lung as the predominant site (38%) both overall and among trauma patients, but the abdomen was the primary site among non-trauma patients (46%). The percentage of lung infections was comparable among trauma patients, with 51% and 54%, respectively. The difference between the hospitals could be explained by volume of trauma patients, because the Hospital B dataset contains three times the amount of trauma patients as Hospital A.
Infections by Site at Hospital A and Hospital B, by Admitting Diagnosis
Percentages rounded to nearest whole number.
p < 0.01 versus Hospital B overall.
p < 0.01 versus Hospital A non-trauma.
p < 0.01 versus Hospital B non-trauma.
Overall, Escherichia coli was the most commonly isolated pathogen in Hospital A, whereas Staphylococcus aureus was the most common isolate at hospital B (Table 3). Enterococci were slightly more common in Hospital A, and Haemophilus influenzae and Enterobacter spp. were more common in Hospital B. However, after stratification between trauma and non-trauma patients, these differences disappeared. Hospital A still had overall more gram-positive organisms and fewer gram-negative organisms among its trauma patients. No differences were noted in percentage of Staphylococcus aureus isolates that were methicillin-resistant Staphylococcus aureus (MRSA; Hospital A, 15%; Hospital B, 18%) or gram-negative isolates that were resistant to one or more major class of antimicrobial agents (Hospital A, 27%; Hospital B, 31%). There were no differences in rates of isolation of fungi between hospitals.
Breakdown of Pathogens Isolated by Hospital and Admitting Diagnosis
Escherichia coli was the most common isolate at Hospital A; Staphylococcus aureus was the most commonly isolated at Hospital B.
Trauma populations at both hospitals had the lungs as the primary site of infection. Percentages rounded to nearest whole number. The superscript * indicates p < 0.05.
MSSA = methicillin-susceptible Staphylococcus aureus; MRSA = methicillin-resistant Staphylococcus aureus; VRE = vancomycin-resistant enterococcus; GNR = gram-negative rod; GPC = gram-positive cocci.
p < 0.05 versus Hospital B overall.
p < 0.05 versus Hospital B trauma.
Hospital antibiograms for Hospital A (Fig. 1) and Hospital B (Fig. 2) are given. Overall, sensitivities were similar and generally within a few percentages of each other. For example, Pseudomonas aeruginosa sensitivities ranged from 84% to 98% at the hospitals, and was 97% for meropenem at both.
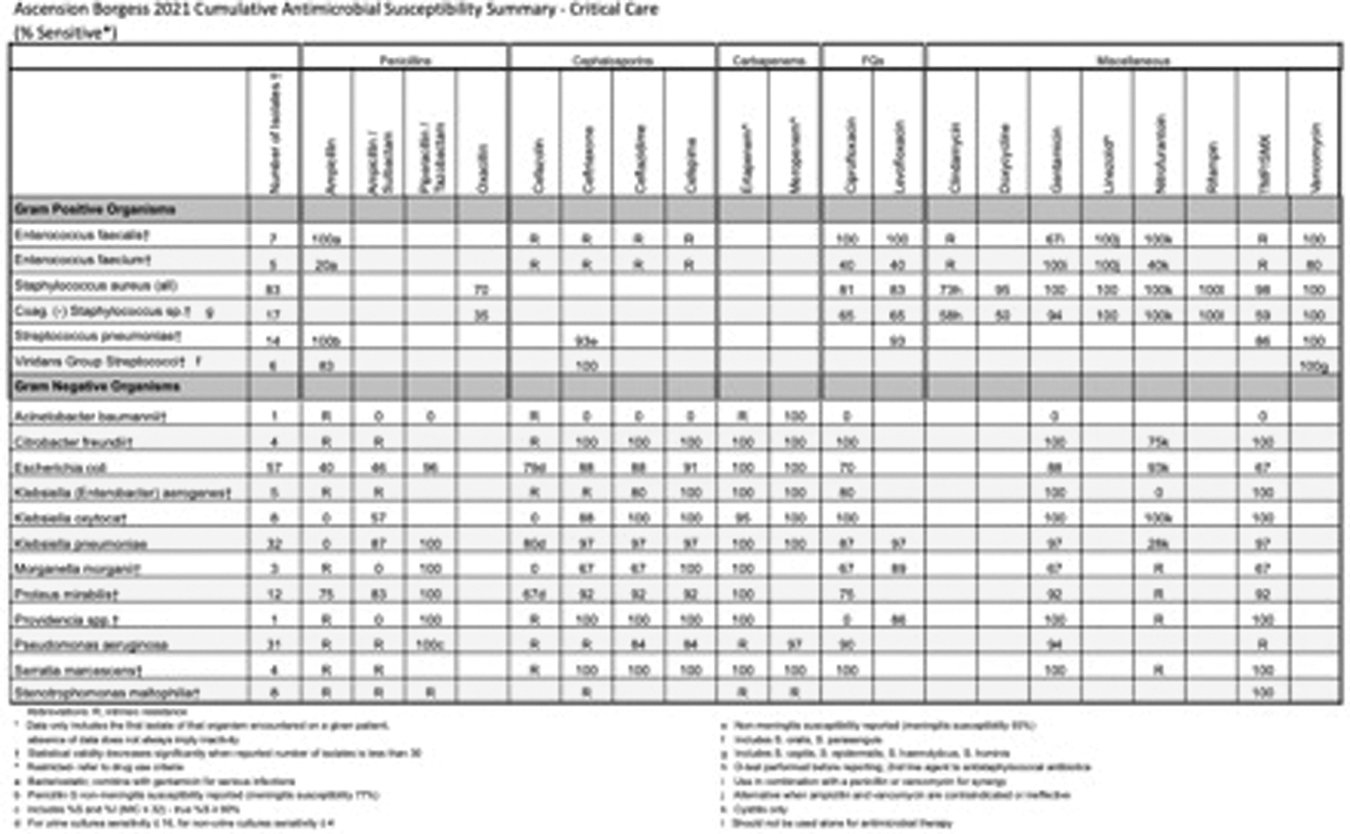
Antibiogram Hospital A, 2021.
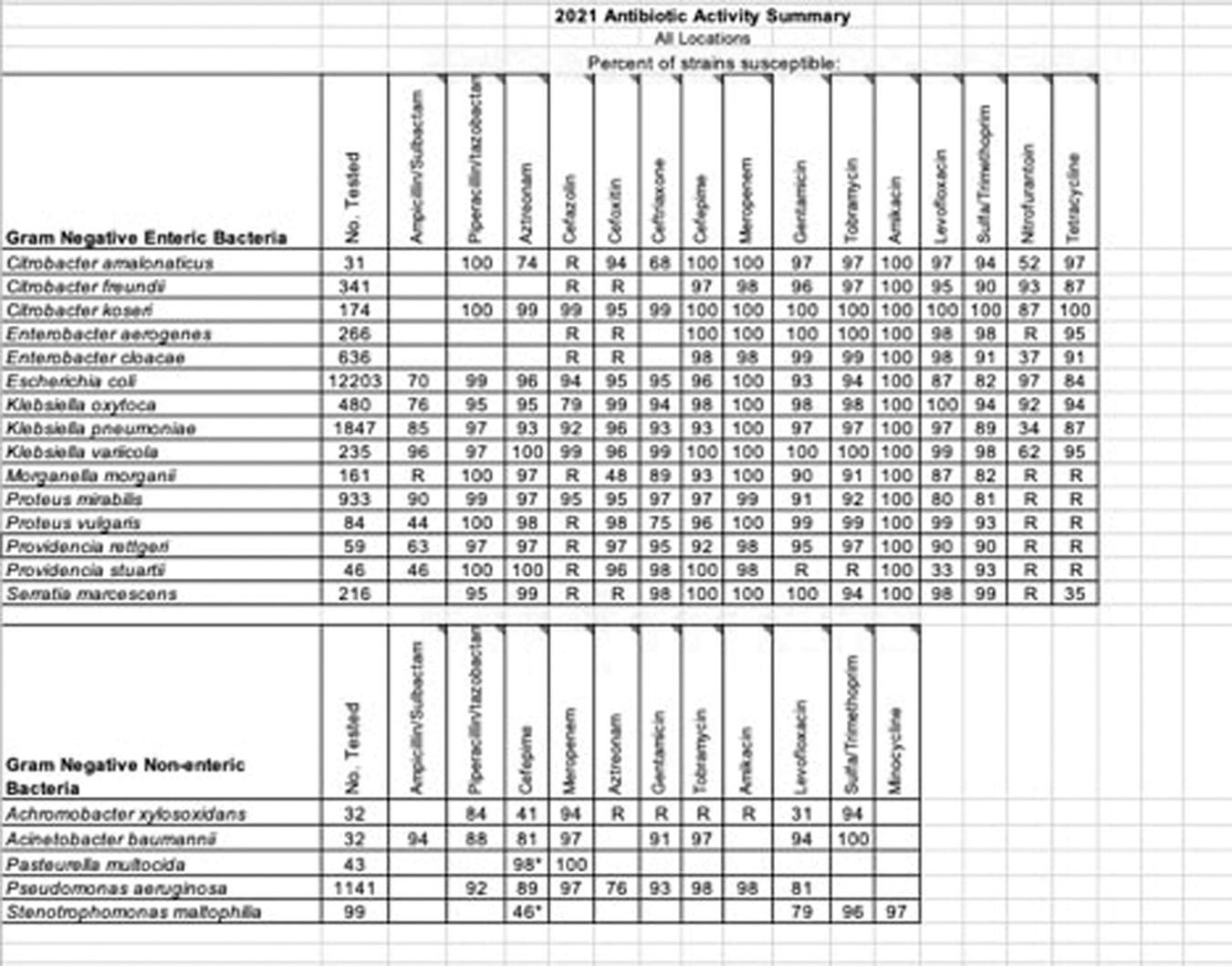
Antibiogram Hospital B, which has significantly more isolates than Hospital A.
Discussion
Admission diagnosis is more closely associated with pathogen isolation than an individual microbiome of a particular hospital. Prior to undertaking this study, patients in the catchments of each hospital usually had a distinct preference for each hospital, and so it was thought that the hospitals would each have a distinct microbiome. Hospital B has a far higher volume of trauma than Hospital A, and initially there appeared to be a higher prevalence of infections among trauma patients. However, when all patients were sorted by APACHE II score, a higher APACHE II score correlated with an increased likelihood of infection.
In addition, the predominance of lung infections in this dataset is largely unsurprising. Ventilator-associated pneumonia remains the most frequent infection among patients in the ICU. 2 Given that Hospital A has a higher percentage of general surgery patients than Hospital B (the general surgical patients at Hospital B are split between the medical ICU and the SICU observed in this study), both hospitals' most common site of primary infection among both general surgical and trauma patients tracks with the dataset. Total ventilator length of stay was not tracked during this study. The fact that the surgical patients at Hospital B are split between two different ICUs is a confounding factor in this study, because it does not allow for full analysis of the surgical patients at both hospitals and their interactions with a singular unit microbiome.
The placement of surgical patients in different units also confounds the antibiogram. At Hospital B, the intensive care unit antibiogram is created using both the medical ICU and the SICU, whereas Hospital A has two ICUs in which surgical and medical ICUs cohabitate. Having a singular ICU for purely surgical patients would allow for a more pure analysis of a microbiome that could affect the development of surgical infections.
Although we documented relatively similar pathogens between the hospitals studied, the data regarding multi-drug–resistant organisms (MDROs) is less clear. Our community has a relatively low baseline rate of MDRO carriage, and previous data from our group has demonstrated the majority of resistant infections in a surgical intensive care unit occur while patients are receiving therapy for other infections and less commonly appear to have been spread from other patients. 6 Therefore, the community MDRO microbiome may influence ICU-acquired infections but may not ultimately be the major driving force behind them. Additionally, humans clearly influence their environmental microbiome, both inside and outside the healthcare system, completing a bi-directional microbial loop.4,7 Future steps will need to be considered, therefore, to reduce antimicrobial resistance pressure in the environment starting with more precise antimicrobial prescription to humans or limiting antimicrobial usage in non-healthcare settings, e.g., to livestock.8,9
Limitations of this particular study include the mingling of surgical and medical patients at both facilities. Without a distinction between these two groups, it is very difficult to delineate if there is a specific microbiome involved in the genesis of surgical infections. In addition, while the antibiograms of both hospitals offer guidance in typical empiric regimens and their resistance profile, there are bound to be variance patterns in antibiotic prescribing between medical intensive care practitioners and surgical intensive care practitioners due to the pathologies treated by each. Universal application of standard antibiotic regimens would assist in clarifying these points. A comparison between surgical patients treated in the medical ICU and surgical patients treated in the SICU would also differentiate if unit-associated microbiomes are involved in the genesis of surgical infections, as given the current findings of our study, patients with similar diagnoses should develop similar infections.
To obtain a flawless comparison, antibiotic regimens would have to be standardized across all practitioners caring for patients with surgical infections. Currently, antibiotic prescription is at the discretion of the clinician caring for the patient, as is consultation with infectious disease. Implementing a platform to bridge any knowledge gaps between providers to ensure homogeneity of antibiotic approach would alleviate this; unfortunately, this does not exist currently. Standardization of antibiotic prescription is a major hurdle in differentiating if the unit microbiome is an important factor in the development of a surgical infection. In addition, tracking the number of days of treatment with antibiotics would also be helpful in further elucidating differences, as well as reducing the risk of overprescription.
In addition, the fact that one hospital is a level 1 and the other is a level 2 trauma center does not yield a perfect comparison and almost certainly led to differences in infection site and pathogens. For that reason, separate analyses of trauma and non-trauma populations were performed. With a larger sample size, a lack of association between hospitals and the pathogens therein could be definitively ruled out or ruled in, and further data could be gathered about the relation between admission diagnosis and pathogen isolation.
Finally, the influence of each individual patient on a hospital room environmental microbiome almost certainly overwhelms the influence of the environmental microbiome outside of that room. This concept is best demonstrated by the rapidity with which hospitals develop their “own” microbiomes 8 as they are populated with humans. This claim could be verified with culturing of the ICU surfaces. Our data, therefore, truly identifies merely a broad overview of bacteria species-level human communities, and subsequently can only be applied modestly to individual patients. Therefore, absent an epidemic, individual patient and ward characteristics are more likely to usefully predict pathogen isolation, rather than an in-depth knowledge of the external microbial environment.
Conclusions
Overall, at a species level, admission diagnosis appears to be a greater determinant of pathogen isolation than individual hospitals when comparing similar intensive care units. A larger body of data is still needed to flesh out a distinct microbial map of organisms occupying a certain geographic region. In conclusion, organisms isolated from surgical infections treated in the surgical intensive care unit seem to be more closely related to admission diagnosis and community prevalence (the “community microbiome”) than ICU-specific antibiograms. Whether similar findings would be reproduced in a SICU with a higher rate of ICU-acquired infections is unknown.
Footnotes
Acknowledgments
The authors would like to thank the support staff at the involved institutions, as well as Mitchell Stein, PharmD and Adam Warner, PharmD for offering support on both creation of antibiograms and microbial resistance at both participating facilities.
Authors' Contributions
Investigation: Moody. Methodology: Moody. Writing—original draft: Moody. Writing—review and editing: Sawyer. Conceptualization: Saywer. Visualization: Saywer. Supervision: Saywer. Formal analysis: Saywer.
Funding Information
There was no funding received for this research.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.