
Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic has brought about drastic hygienic measures, one upside of which might be the mitigated occurrence of surgical site infection (SSI). This study investigated the association of the pandemic with SSI occurrence after cardiac surgeries.
Patients and Methods:
From 2014 to 2022, patients undergoing cardiac surgery were included and categorized into pre-pandemic and during-pandemic groups. Surgical site infections were classified into harvest-site, superficial sternal, and complex sternal infection. Multiple logistic regression and inverse probability weighting assessed the association of the pandemic with SSI.
Results:
Among a total of 26,143 patients, 793 SSIs occurred. The during-pandemic patients were younger (61.87 ± 10.58 vs. 65.64 ± 11.82) with a higher male proportion (70.1% vs. 67.4%) and a higher prevalence of all studied comorbidities/risk factors (expect cigarette smoking). Total SSI rate decreased substantially from 3.3% before COVID-19 to 1.8% afterward (p < 0.001). Inverse probability weights analyses evinced an independent association of the pandemic with a reduced risk of total (adjusted odds ratio [OR]; 0.59; 95% confidence interval [CI], 0.45–0.78), harvest-site (adjusted OR, 0.36; 95% CI, 0.19–0.70), and superficial sternal infection (adjusted OR, 0.60; 95% CI, 0.43–0.81). No significant association was observed with complex sternal site infection (adjusted OR, 1.05; 95% CI, 0.55–2.01). Multivariable regression recapitulated these findings.
Conclusions:
The COVID-19 pandemic independently pertained to more than a 40% reduction in SSI occurrence, particularly affecting harvest-site and superficial sternal infections. However, there remains the possibility of the implications of other known and unknown confounders on the observed association. To some extent, the decrease in SSIs after the pandemic can be justified by reinforced hygienic precautions, emphasizing the necessity of extending the adherence to these measurements into the post-COVID-19 era to maintain the status quo.
Surgical site infection (SSI) is one of the major post-operative complications responsible for approximately half of all hospital-acquired infections (HAIs). Surgical site infection occurrence is inextricably intertwined with higher mortality and morbidity and imposes a great financial burden.1–-6 Various patient and hospital-level interventions are introduced to alleviate this condition. Hospital-level interventions comprise evidence-based skin sanitization, antibiotic prophylaxis, hospital traffic, hand hygiene, and antisepsis protocols during wound care.7–9
Despite numerous calls for action aiming at curbing the SSI rates, these calls have mainly remained disregarded, resulting in a substantial gap between the expected and the actual rates of SSIs. 10 Nevertheless, the coronavirus disease 2019 (COVID-19) pandemic taught us that drastic hygienic measures could be used effectively on such short notice. After the onset of the COVID-19 pandemic, new recommendations were integrated into the guidelines by the World Health Organization (WHO) and U.S. Centers for Disease Control and Prevention (CDC), including the permanent use of face masks, contact and droplet safety measures, and restricting visitors and patient density.11–13 Furthermore, healthcare workers' adherence to previously established evidence-based hygienic standards was considerably boosted.14,15 After the pandemic hit, studies demonstrated a sizable drop, as high as 40% to 70%, in the rates of SSIs after various procedures.1,16–18 To some extent, this reduction can be justified on the grounds of reinforced hygienic measures during this time. In light of this information, this study aimed to evaluate the possible impact of the COVID-19 pandemic on the rate of SSIs among a large cohort of patients undergoing cardiac surgeries.
Patients and Methods
Study design and population
This cross-sectional retrospective study was conducted at Tehran Heart Center, Tehran, Iran. This center is one of Iran's major tertiary cardiovascular centers with a high load of cardiac surgeries. 19 Data were collected from the Cardiac Surgery Databank of Tehran Heart Center. From 2014 to 2022, all patients who underwent cardiac surgeries were included. Patients were excluded if they had pre-operative active infections at the index hospitalization. A total of 26,143 patients were enrolled (age, 65.05 ± 11.71; male gender, 67.8%) and were categorized into pre-pandemic (n = 22,015) and during-pandemic (n = 4,128) groups (cutoff point: February 20, 2020 when COVID-19 protocols were enforced in our hospital). Supplementary Table S1 represents measures directed at COVID-19 infection prevention at our center. The study was approved by the local ethics committee (Institutional Review Board: IR.TUMS.THC.REC.1401.037) and conformed to the Declaration of Helsinki. The need for informed consent was waived due to the retrospective nature of the study and the anonymization of the data. The authors did not have access to information that could identify individual participants during or after data collection. The manuscript adheres to the STROBE guideline for observational studies (Supplementary Table S2).
Outcome and variable definitions
The study outcome was the occurrence of total and classified SSIs, including harvest-site (either superficial or complex), superficial sternal, and complex sternal infections. Surgical site infections were defined based on in-hospital infection control guidelines, compatible with the CDC definitions 20 (see Supplementary Materials for more details). Other variables were defined similarly to our previous studies on this population. 21
Causative pathogens were classified into the following groups based on their type and prevalence. Gram-positive bacteria included Staphylococcus aureus, coagulase-negative staphylococci (CoNS), and other gram-positive bacteria. Gram-negative bacteria encompassed Escherichia coli, Klebsiella spp., other Enterobacteriaceae, and non-fermentative gram-negative bacteria (NFGNB). The last group was fungi/polymicrobial pathogens.
Statistical analyses
Categorical variables are presented as frequencies (percentages) and were compared between the two groups using Pearson χ 2 or Fisher exact tests as appropriate. Normally distributed continuous variables are expressed as mean ± standard deviation and were compared using the Student t-test. Non-normally distributed continuous variables are expressed as median with 25th and 75th percentiles and were compared using the Mann-Whitney test.
To assess the association between COVID-19 pandemic and SSIs, two separate analyses were conducted time-wise. First, the during-pandemic group was evaluated versus the whole group before the pandemic (from 2014 to February 20, 2020) for the main analyses. Second, we chose a narrower period for complementary analyses to ensure that the clinical practice in the two groups has remained as unchanged as possible. Therefore, the exact period of enrolled patients who underwent surgery during the pandemic was calculated (February 20, 2020 to November 30, 2021; 649 days) and was compared against the exact corresponding time before the pandemic (May 12, 2018 to February 20, 2020).
The unadjusted and adjusted association of the COVID-19 pandemic with SSI occurrence was evaluated using logistic regression models. Variables that are known to affect SSIs were used for adjustments, including age, gender, diabetes mellitus, hypertension, hyperlipidemia, cigarette smoking, opium use, positive family history of coronary artery disease, body mass index of 30 or more, ejection fraction of 40 or less, and the type of cardiac surgery. To further address confounding bias, stabilized inverse probability weights (sIPW) based on the propensity scores of the COVID-19 pandemic and the abovementioned confounders were also calculated, and the association of COVID-19 pandemic with SSI occurrence was evaluated by applying sIPW. Figure 1 and Supplementary Table S3 depict the density distribution plot of the propensity scores and the standardized mean difference between the two study groups before and after sIPW balancing, respectively. The weights provided a high coverage, and the standardized differences were below 0.1, indicating that the two groups were appropriately balanced.
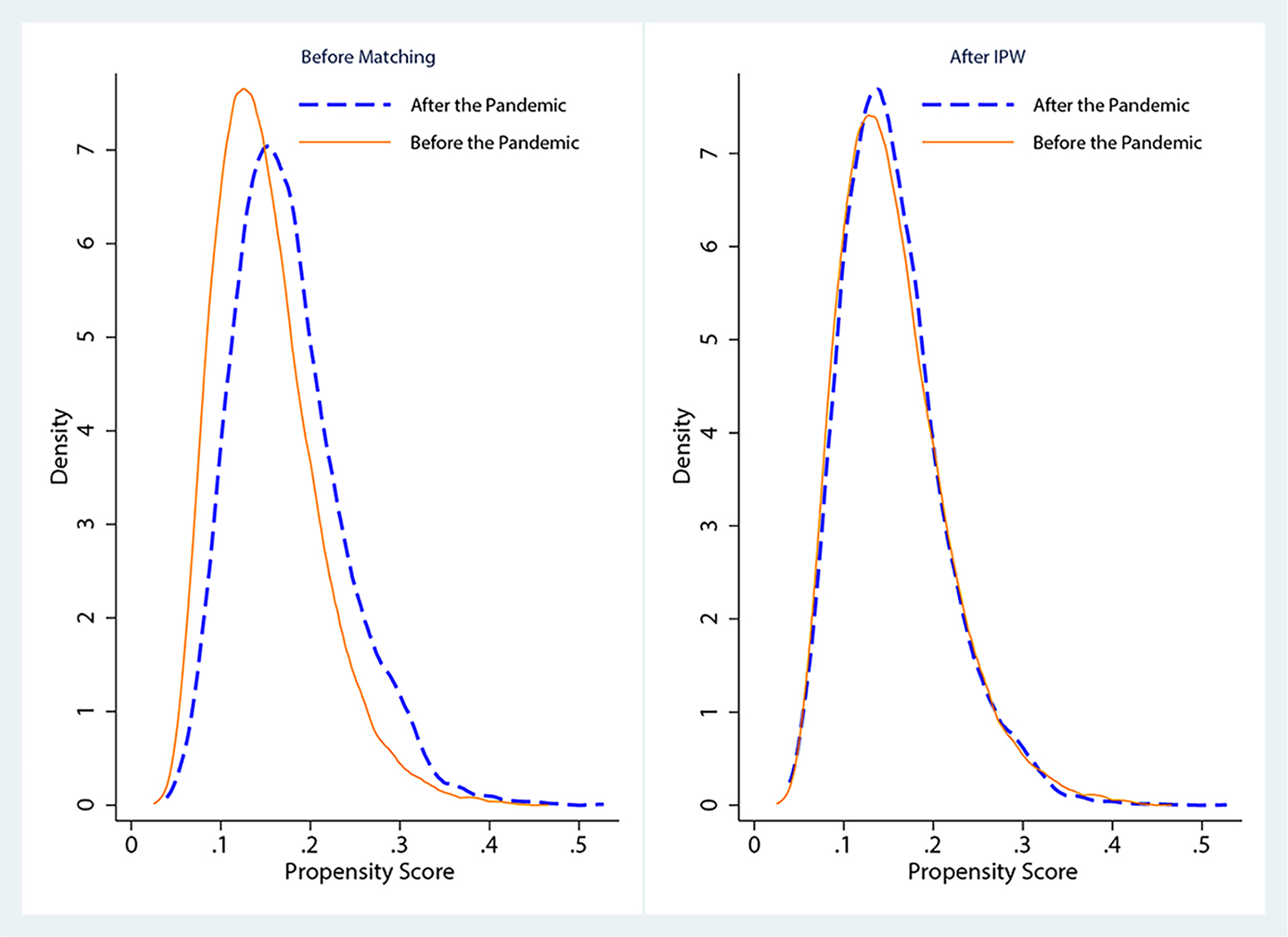
The density distribution plot of the propensity scores between the two study groups before and after sIPW balancing. *2019–2020 refers to 2019 until February 20, 2020 (pre-pandemic), and 2020–2021 is from February 20, 2020 onwards (during-pandemic).
The effects are reported as odds ratio with a 95% confidence interval. Missing data were handled using a complete case analysis (below 10%). Statistical analyses were performed using STATA, version 14.0 (StataCorp, College Station, TX).
Results
Baseline characteristics
Patients in the during-pandemic group were younger (61.87 ± 10.58 vs. 65.64 ± 11.82; p < 0.001), and more likely to be males (70.1% vs. 67.4%; p < 0.001), have diabetes mellitus (37.9% vs. 36%; p : 0.020), hypertension (55.6% vs. 49.9%; p < 0.001), hyperlipidemia (49.5% vs. 44.6%; p < 0.001), a positive family history of coronary artery disease (28.7% vs. 26.8%; p :0.016), body mass index of 30 kg/m2 or more (27.1% vs. 24.6%; p : 0.002), ejection fraction of 40 or less (34.9% vs. 32.4%; p : 0.001), and to use opium (18.0% vs. 15.0%; p < 0.001). On the other hand, they were less likely to be cigarette smokers (9.5% vs. 12.4%; p < 0.001; Table 1).
Baseline Characteristics
Data are presented as frequency (percentages), mean ± standard deviation (SD), or median [25th percentile to 75th percentile].
BMI = body mass index; EF = ejection fraction; CABG = coronary artery bypass grafting.
Surgical site infection characteristics
Table 2 represents details of the SSI characteristics. A total of 793 (3%) SSIs occurred in the study population. The total SSI rate decreased substantially from 3.3% before COVID-19 to 1.8% after (p < 0.001). This reduction was mainly attributable to the harvest-site infection (0.9%–0.3%) and superficial sternal infection (1.9%–1.1%). The onset of SSI was delayed for all the SSI types; however, it was only significant for complex sternal infection (15 [11–30] to 26 [20–58] post-operative days; p = 0.004).
Surgical Site Infection Characteristics
Data are presented as frequency (percentages), mean ± standard deviation (SD), or median [25th percentile to 75th percentile].
SSI = surgical site infection.
Percentages are reported among 576 SSIs in which pathogens were isolated.
Pathogens were isolated in 576 of 793 SSI cases (72.60%); others were diagnosed clinically (without performing the tests or in a clinically compatible setting when the test was inconclusive). Table 2 and Figure 2 demonstrate the distribution of isolated pathogens. Changes in causative pathogens were not significant (p = 0.368). However, an increase in gram-positive bacteria was observed from 64.6% to 72% and a decrease in gram-negative bacteria (from 33.1% to 28.0%). These changes mainly originated from a respective 3.8% and 4.5% increase in Staphylococcus aureus and CoNS, combined with a respective 4.9% and 2.9% decrease in Escherichia coli and Klebsiella.
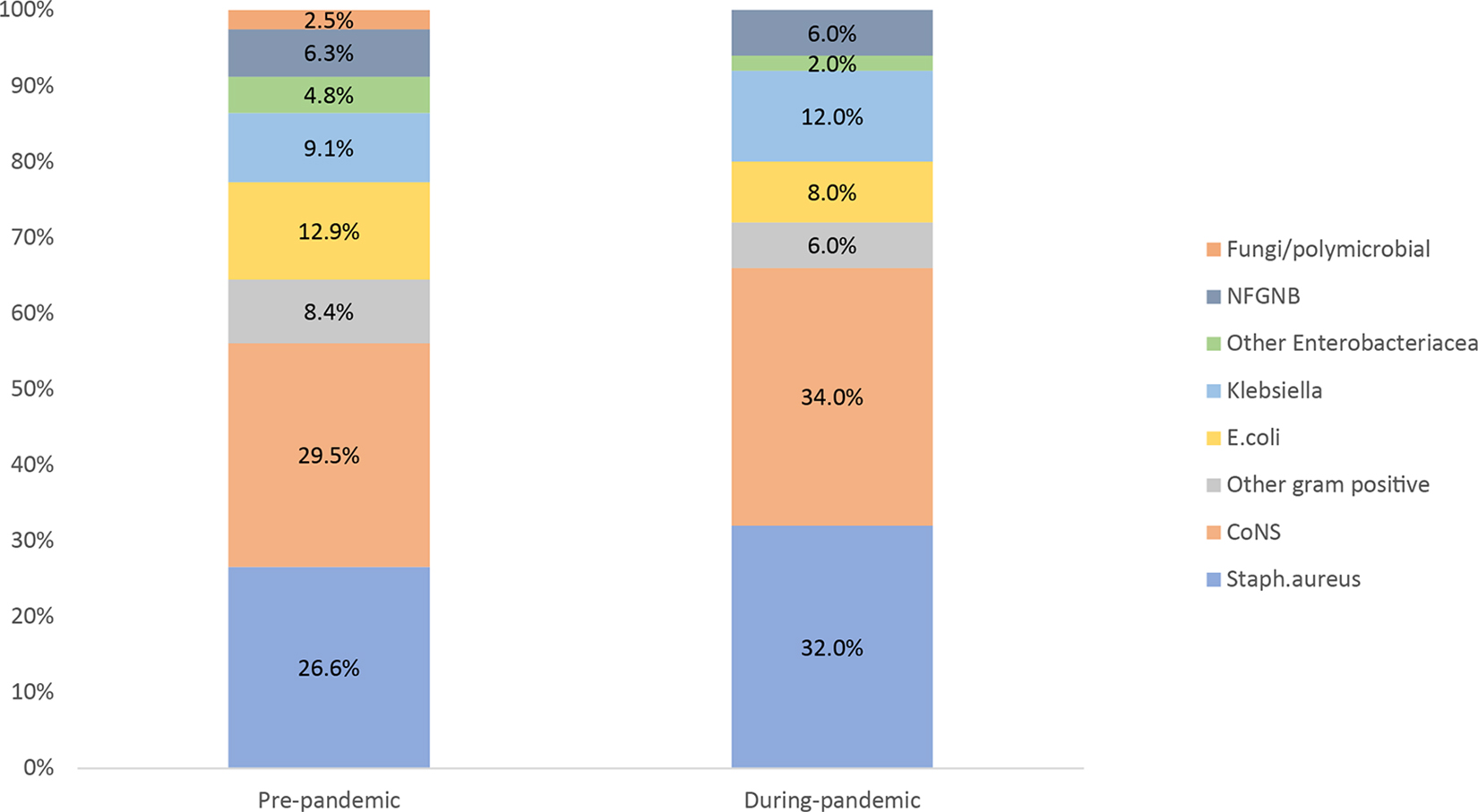
The distribution of isolated pathogens. *Staph. aureus = Staphylococcus aureus; CoNS = coagulase-negative staphylococci; E. coli = Escherichia coli; NFGNB = non-fermentative gram-negative bacteria.
Association between the COVID-19 pandemic and SSI occurrence
Table 3 demonstrates the association between the pandemic and SSI occurrence. Compared with the entire pre-pandemic period, the COVID-19 pandemic was associated with a 45%, 62%, and 44% reduction in the unadjusted risk of total SSI, harvest-site SSI, and superficial sternal SSI infections, respectively (all p < 0.001). After adjustments with multivariable regression, the association remained significant with comparable risk reduction to the unadjusted findings (total SSI: adjusted odds ratio [OR], 0.58; 95% confidence interval [CI], 0.44–0.75; p < 0.001; harvest SSI: adjusted OR, 3.37; 95% CI, 0.20–0.72; p < 0.001; superficial sternal SSI: adjusted OR 0.59; 95% CI, 0.42–0.83); p < 0.001). Full multivariable models can be found in Supplementary Table S4. The sIPW analyses recapitulated these findings. The COVID-19 pandemic did not substantially affect complex sternal SSI, either at the unadjusted, multivariable regression or sIPW models. The complementary analyses of the during-pandemic group versus the exact corresponding time in the pre-pandemic group confirmed these findings and were in high agreement with the abovementioned numbers (Table 3). To further explain, the adjusted odds ratios remained relatively stable from the main analysis to complementary analysis for total SSI (from 0.58–0.59), harvest-site SSI (from 0.37–0.32), and superficial sternal SSI (from 0.59–0.66), and the association remained non-significant for complex sternal SSI (from p = 0.963 to p = 0.760). These similarities were applicable to unadjusted and sIPW models, as well.
The Association Between the COVID-19 Pandemic and SSI Rates
SSI = surgical site infection; OR = odds ratio; CI = confidence interval; sIPW = inverse probability weighting.
Discussion
Main findings
This study indicated an association between the COVID-19 outbreak and reduced risk of 41%, 64%, and 40% for total SSI, harvest SSI, and superficial sternal SSI among patients undergoing cardiac surgery, respectively. No significant association was observed for complex sternal SSI. It is imperative to mention that the possible implications of other known and unknown confounders on these observed associations remain. Furthermore, we believe that these observed associations reflect the collective effects of changes in behavioral factors, hospital- and community-level policies, and re-enforced hygienic measures, rather than the era of the surgery per se.
Clinical implications
Surgical site infections are considered the most frequent, yet the most preventable, type of HAIs in low- and middle-income countries, 10 affecting 2% to 8% of surgeries. 2 Post-cardiac surgery SSI is linked to a 10-fold increase in mortality, lengthened hospital stay, doubled re-admission, and extended outpatient follow-up,2–6 hence the importance of curbing SSI rates. Although we did not find a reduction in complex SSIs, which carry higher morbidity and mortality compared with superficial SSIs, our findings remain clinically relevant. Experts agree that superficial SSIs also increase length of stay, which, per se, can result in increased hospital financial burden, patient discomfort, and dissatisfaction.22,23 Furthermore, studies have indicated that 100% of gram-negative bacteria isolated from superficial SSIs were resistant to most of the antibiotic agents, 24 hence the important role of superficial SSIs on multi-drug resistance. Finally, superficial SSIs constitute the majority of SSIs (almost five times prevalence of superficial compared to complex sternal SSI in our study). Thus, despite the lesser morbidity of superficial SSIs at the individual level, their influence on a large number of post-surgical patients and at the community- and hospital-levels cannot be overlooked.
Existing literature on the association between the pandemic and SSIs
The COVID-19 pandemic has changed the prevalence and manifestations of various clinical conditions.25–28 Congruent with our findings, many studies have reported a reduction in SSI rates after colorectal cancer surgery (48%), 29 neurosurgical procedures (51%), 18 general surgeries (60%), 16 and cardiac surgeries (73%) during the pandemic. 17 Nevertheless, a single-center study on patients who underwent oculofacial plastic surgeries failed to demonstrate a significant association, 30 which might be due to their very low SSI incidence, precluding the study from drawing any statistical significance. Another large multicenter study did not report a significant reduction in SSI occurrence either. 31 Remarkably, rather than using SSI rates, this study opted for the National Health and Safety Network (NHSN) standardized infection ratio (SIR) to asses SSIs. This ratio compares the observed numbers of HAIs to the predicted numbers, standardized to a specific population (such as the NHSN baseline). Besides the difference in the assessment method and procedure type, these authors have suggested that the hospitals and procedures with already lower rates of SSI during the pre-COVID-19 era might not benefit from heightened hygienic precautions as much as their counterparts with higher SSIs.
All in all, variations in the magnitude of the pandemic implications on SSI reduction can be justified on the grounds of different procedure types, pre-pandemic and during-pandemic periods included in analyses, confounder selection, risk factor distribution, and SSI definitions.
In addition to our study, others have reported a greater reduction in superficial rather than deep organ/space infections during the pandemic.32,33 This might be due to a naturally lower incidence of deep infections, their more challenging management, or their dissimilar predictors. 34
Possible justifications behind reduced SSIs in the COVID-19 era
Increased adherence to SSI preventive measures: hand hygiene and wound care
Despite vigorous calls for action to enhance infection control measurements during the recent years, these calls have remained unheeded. There has been an alarming gap between the expected and performed wound care practices. 10 Nonetheless, the COVID-19 pandemic disclosed that effective preventive actions could be used on such short notice, including evidence-based hand hygiene, using personal protective equipment, 14 and reducing hospital traffic within rooms and common areas. Importantly, these measurements have been in guidelines on SSI prevention for many years before the pandemic; however, caregivers' adherence has remained a crucial aspect. It is plausible that increased adherence of the medical staff to established guidelines during the pandemic could have played a considerable role in decreased SSIs risk.
Generally, pathogens can colonize the surgical site up until the complete healing of the wound, which encompasses the operative and immediate post-operative period. These pathogens can infect the surgical site incision thorough three pathways: endogenous bacteria from patient's skin (due to inappropriate skin disinfection and draping), exogenous bacteria from caregivers' skin (due to not properly cleaning or dressing the wound, touching it with unclean hands, or using wrong type of gloves), and distant sources from the surgical site, such as contaminated arterial lines and central venous lines, which could spread through blood and colonize the surgical site. Surgical site infections can develop via all three mentioned routes during the surgery and the two latter sources after the surgery, hence the importance of nursing incision care practices and effective hand washing, not only when directly dealing with the surgical site but also with arterial and central venous lines. 35
Preceding the pandemic, up to half of the nursing staff and physicians were not fully aware of guideline recommendations, and their adherence was suboptimal.36,37 According to pre-pandemic studies, almost one in five nurses displayed erroneous surgical site care management, including not wearing gloves or wearing the wrong type, contaminating the aseptic field, or not washing hands after incision care between patients. 35 Through observing medical staff, pre-procedural hand-washing compliance according to the CDC guidelines was evinced for only 5.2% of the staff, with only 8.5 and 6.6 seconds of hand-washing (i.e., ineffective hand washing 38 ) for physicians and nurses, respectively. 39 This is while the optimal duration of hand washing to effectively eliminate pathogens is at least 30 seconds. 38
Various negative (including insufficient evidence-based knowledge, skills, and perception of hand-washing as a norm in the hospital36,40) and positive predictors (including staff education of hand washing, awareness of being observed, encouraging attitude toward hand hygiene, and convenient access to hand-rub solutions36,40) of evidence-based hand washing has been changed during the pandemic,15,40,41 which can act as the link between the association between the pandemic and reduced SSI rates.
Other justifications
Other underlying etiologies might be related to personal protective equipment (PPE), the inconsistent use of which has been shown to increase the risk of HAI. Moreover, the role and responsibilities of infection preventionists were emphasized during the pandemic as team leaders in charge, implementing stricter monitoring and surveillance and ensuring the use of the best practices. 42 Additionally, keeping the operative room personnel to a minimum might have played a role since it lessens the dissemination of bacteria-carrying particles (BCP) from the medical staff. 43 Importantly, we should admit that our study was unable to actually measure the abovementioned explanations (such as increased hand hygiene compliance, the exact amount of PPE use, etc.) and assess their effect, rather, we had to assess the implications of the pandemic occurrence as a whole. Therefore, we cannot exactly identify the role of each hygienic measure in SSI occurrence separately.
Despite all the abovementioned promising progress, a subtle contention still exists. The adherence of staff to hygienic measures has been shown to decrease between pandemic waves. Thus, it is conceivable that standard hygienic practice is, to a great extent, a matter of self-protection rather than patient protection. Consequently, it seems imperative to implement stricter surveillance measures during the post-COVID-19 era rather than simply assuming that the pandemic has revolutionized the medical staff's attitude toward adherence to preventive measures for the patient's sake. 15
Conclusions
This study indicated a considerable reduction in the SSI rate after the pandemic hit. This decrease could, to some extent, reflect the implications of reinforced hygienic measures during this time. Hence, these findings emphasize the urgent necessity of extending infection control and surveillance fortification beyond the pandemic era.
Strengths and limitations
This study is limited by its observational, single-center, and retrospective nature. Although these associations could be attributed to collective modifications in the pandemic era, our study failed to measure the effects of each individual pandemic-related factor separately. Thus, there are no certain ways to ensure that to what extent the reduction in SSI rates was related to reinforced hygienic measures during the pandemic and not other factors. More importantly, we did not observe hand hygiene compliance among the hospital staff; nevertheless, as the working personnel, we can confirm that the increased compliance was evident in observation. Furthermore, although the poor versus well controlled status of diabetes mellitus affects SSI occurrence beside the mere presence of diabetes mellitus, 44 we did not have data on HbA1c. Finally, our model did not include risk scores such as the Society of Thoracic Surgeons (STS) score for deep sternal wound infection. However, we assume that this matter could not have resulted in considerable different findings. Conventional risk scores consist of numerous variables, which both decrease their implications to clinical practice and their feasibility to be used in research studies. Thus, newer tools for predicting SSIs have emerged that have even outperformed existing scores. The recent Barts Surgical Infection Risk (B-SIR) tool 45 is one of these models comprising seven predictive variables, six of which were evaluated in our models.
Despite these limitations, we tried to perform two methods of adjustment in an endeavor to control for known infection-related risk factors. An upside of our study is its large population and considerable time span compared with the literature.
Footnotes
Authors' Contributions
Conception and design: Jameie, Bagheri, Boroumand, Barkhordari, Bagheri. Data acquisition: Pashang, Ilkhani, Mameie, Nosrati. Data analysis: Mameie, Pashang, Jalali. Data interpretation: all authors. Drafting the article: all authors. Critically revising the article: all authors. Final approval: all the authors.
All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data Availability
Data are available from the corresponding author on reasonable request.
Funding Information
No funding was received.
Author Disclosure Statement
The authors declare that they have no conflict of interest. The study was approved by the ethics committee of Tehran Heart Center (IR.TUMS.TEH.REC.1401.037).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.