
Abstract
Objective:
This study investigates the practicability of serum kallistatin as a biomarker in the diagnosis of tubo-ovarian abscess (TOA) because C-reactive protein (CRP) is insufficiently specific for diagnosis.
Methods:
Thirty patients (control group) who presented for elective gynecological surgeries and 30 who were hospitalized due to TOA (study group) at the Antalya Training and Research Hospital Gynecology Clinic, Türkiye, between January 1 and December 31, 2022, were included in the study. Blood samples were collected for the calculation of complete blood count, biochemistry, CRP, and serum kallistatin values, and the results were recorded in a database.
Results:
Although no significant differences were observed between the control and study groups in terms of age or body mass index, significant differences were observed in terms of marital status, number of pregnancies, parity number, intrauterine device history, and previous surgical history (p > 0.05). Serum hemoglobin levels (12.61 ± 1.30 vs. 11.47 ± 1.77; p = 0.008), white blood cell (7.9 [6.15 ± 9.7] vs. 17.0 [11.6–19.6]; p < 0.001), neutrophil (4.6 [3.6–6.12] vs. 13.6 [9.25–16.1]; p < 0.001), lymphocyte (2.51 ± 0.71 vs. 2.33 ± 0.69; p = 0.307), and platelet counts (285.63 ± 78.0 vs. 407.03 ± 131.96; p < 0.001), neutrophil–lymphocyte ratio (2.11 ± 0.93 vs. 6.18 ± 2.20; p < 0.001), neutrophil–lymphocyte ratio (123.16 ± 52.63 vs. 184.39 ± 63.90; p < 0.001), hs-CRP (1.20 [5.55–1.92] vs. 240 [138.25–291.0]; p < 0.001), kallistatin (7.18 ± 3.15 vs. 3.83 ± 3.69; p = 0.006), and urine leukocyte values (1 [0.75–3] vs. 3 [1–6.5]; p = 0.038) also differed significantly between the control and study groups.
Conclusion:
The study findings show that serum kallistatin levels can be used as a biomarker in the diagnosis of TOA. Further studies involving more participants are now needed to test the accuracy of our results.
Introduction
According to the National Health and Nutrition Examination Survey data, 4.4% (2.5 million) of women of reproductive age in the United States have histories of pelvic inflammatory disease (PID). 1 Tubo-ovarian abscess (TOA) accompanies 2.3%–20% of hospitalized PID cases. This condition is associated with severe complications, such as abscess rupture or sepsis, which can lead to high morbidity and mortality. 2 When TOA causes sepsis, morbidity increases and the mortality rate can increase by 5%–10%. 3 In addition, a systematic review of nine studies evaluating TOA in 199 patients in the postmenopausal period reported a risk of malignant disease in TOA from 2.5% to 47%. 4 It is very important to establish prompt and accurate diagnosis through clinical evaluation, additional imaging methods, and biochemical markers and to initiate appropriate treatment as soon as possible, both in terms of evaluating the complications of TOA and of excluding differential diagnoses. 2
C-reactive protein (CRP), a ligand-binding plasma protein of the pentraxin family, is a reliable and frequently used biomarker in the diagnosis of TOA and is secreted depending on the responses of cytokines and interleukin (IL)-6. 5 CRP can also increase in conditions such as trauma, acute pancreatitis, burns, malignant disease, and myocardial infarction, independently of inflammation. However, it is not considered a specific biomarker in the diagnosis of TOA.
Kallistatin is a human serine proteinase inhibitor first discovered by Chao et al. in 1992 and identified as a tissue kallikrein-binding protein. 6 Kallistatin exerts its anti-inflammatory effect by inhibiting the tissue kallikrein-kinin system, activating the vasodilation mechanism, inhibiting the tumor necrosis factor -α response, and increasing the degradation of nuclear factor kappa-B in endothelial cells.7,8 A previous study showed that kallistatin exhibits a protective effect against myocardial ischemia by suppressing oxidative stress and inflammation and against renal ischemia by ensuring water and salt retention in the body. To summarize, kallistatin suppresses angiogenesis, inflammation, apoptosis, hypertrophy, fibrosis, and oxidative stress. 9
This study aimed to investigate the practicability of kallistatin as a more specific biomarker than CRP, which is currently used as a biomarker in the diagnosis of TOA but lacks high sensitivity and specificity.
Materials and Methods
This prospective case–control study was conducted at the Antalya Training and Research Hospital Gynecology Clinic, Türkiye, with ethics committee approval (reference number 18/12). Patients who presented between January 1 and December 31, 2022, with complaints such as groin pain, purulent discharge, severe pain during intercourse, and fever, who were aged 18–55, with purulent discharge during gynecological examination, cervical tenderness, and elevated CRP and white blood cell (WBC) values, with heterogeneous lesions compatible with a complicated abscess at ultrasonography (USG), and who were diagnosed with TOA were included in the study. The diagnosis of TOA was on the basis of the major and minor criteria of the Sexually Transmitted Infections Treatment Guidelines, 2021. 10 An USG (Hitachi HI VISION Avius) device was used to visualize the abscesses, which were evaluated by a single clinician (M.B.B.). Patients with other acute inflammatory processes accompanying TOA (appendicitis, necrotizing fasciitis, cholecystitis, etc.), chronic inflammatory diseases such as rheumatoid arthritis or polycystic ovary syndrome, and acute conditions capable of causing pelvic pain (such as ectopic pregnancy, torsion, and cyst rupture) were excluded from the study.
Two-milliliter blood samples were collected to calculate serum CRP and kallistatin levels before treatment. These were centrifuged at 2000 g for 10 min and then stored at −80°C. Similar samples were also collected from the members of the control group to determine serum kallistatin levels, and these were again stored at −80°C after centrifugation.
Biochemical measurement of serum kallistatin
A Human Kallistatin Elisa kit (Catalog No. E3392Hu 96 Tests) was used to measure kallistatin levels using the enzyme-linked immunosorbent assay (ELISA) method. Serum kallistatin levels were expressed as µg/mL.
Sandwich-ELISA was used as the kit method for measuring serum kallistatin. Briefly, the micro-ELISA plate provided with the kit was coated with an antibody specific to Human SERPINA4. Each sample was added to appropriate micro-ELISA plate tubes. A specific detection antibody for human SERPINA4 and Avidin-horseradish peroxidase (HRP) conjugate was pipetted and incubated into each tube. In this method, only the incubated tubes containing the human SERPINA4 detection antibody and Avidin-HRP conjugate exhibit a blue color. The enzyme-substrate reaction is terminated by adding an inhibitor solution, at which the color returns to yellow. Optical density (OD) was measured spectrophotometrically at a wavelength of 450 nm ± 2 nm, and the concentration of human SERPINA4 in the samples was calculated according to the OD standard curve of the samples. The sensitivity of the kit is 0.022 ng/mL, and the detection range is 0.05–20 ng/mL.
Data input
The patient’s age, body mass index (BMI), gravidity, parity, marital status, menopause status, intrauterine device (IUD) and tuba uterine ligation history, previous operations, laboratory findings, abscess localization morphology, and diameter were recorded in the database. The neutrophil-to-lymphocyte ratio (NLR) was calculated by dividing the absolute neutrophil number by the lymphocyte number, and the platelet-to-lymphocyte ratio (PLR) was calculated by dividing the absolute neutrophil number by the lymphocyte number.
Statistical analysis
IBM Statistics 22 software was used for statistical analysis. The Shapiro–Wilk test was applied to determine normality of distribution, p > 0.05 being considered normal. Skewness and kurtosis values were checked, and normal Q-Q PLOT graphs were also used for non-normally distributed data. Normally distributed data were analyzed using Student’s t test and one-way ANOVA and non-normally distributed data using the Mann–Whitney U and Kruskal–Wallis tests. The cutoff values of the independent variables for our dependent variable were calculated using receiver operating characteristic (ROC) curve analysis. Pearson’s correlation tests were used for normally distributed data, and Spearman’s correlation tests were used for non-normally distributed data. p values <0.05 were considered significant.
Results
Thirty patients diagnosed with TOA and 30 patients scheduled for elective gynecological surgery in the Antalya Training and Research Hospital gynecology clinic between January 1 and December 31, 2022, were included in the study.
The participants’ sociodemographic characteristics and laboratory values are shown in Table 1. Although age (control group 42.13 ± 11.36 vs. study group 37.5 ± 8.53; p = 0.079) and BMI (24.0 [22.0–25.0] vs. 22.95 [21.85–24.92], respectively, p = 0.594] were comparable between the groups, statistically significant differences were observed in terms of marital status (single 1 [3.3%], married 29 [96.7%] vs. single 15 [50.0%], married 15 [50.0%], respectively, p < 0.001), numbers of pregnancies (2.5 [1.0–3.0] vs. 3.0 [2.0–4.0]; p = 0.044) and parity (2.0 [0.75–2.0] vs. 3.0 [2.0–4.0]; p < 0.001), IUD history (0 [0%] vs. 22 [73.3%]; p = 0.005), and previous surgical histories (3 [10%] vs. 14 [46.7%]; p = 0.003).
Participants’ Sociodemographic Characteristics
Statistically significant.
BMI = body mass index; IUD = intrauterine device; Hb = hemoglobin; WBC = white blood cell; NLR = neutrophil-to-lymphocyte ratio; PLR = platelet-to-lymphocyte ratio; CRP = C-reactive protein.
The control and study groups’ serum Hb (12.61 ± 1.30 vs. 11.47 ± 1.77, respectively, p = 0.008), WBC (7.9 [6.15 ± 9.7] vs. 17.0 [11.6–19, 65]; p < 0.001), neutrophil (4.6 [3.6–6.12] vs. 13.6 [9.25–16.1]; p < 0.001), lymphocyte (2.51 ± 0.71 vs. 2.33 ± 0.69; p = 0.307), platelet (285.63 ± 78.0 vs. 407.03 ± 131.96; p < 0.001), NLR (2.11 ± 0.93 vs. 6.18 ± 2.20; p < 0.001), PLR (123.16 ± 52.63 vs. 184.39 ± 63.90; p < 0.001), hs-CRP (1.20 [5.55–1.92] vs. 240 [138.25–291.0]; p < 0.001), and kallistatin (7.18 ± 3.15 vs. 3.83 ± 3.69; p = 0.006) values differed significantly.
Table 2 summarizes the relationships between treatment type, serum kallistatin value, and abscess diameter. No significant difference was observed between the groups in terms of serum kallistatin levels (Group 1, medical treatment 4.91 + 1.64, vs. Group 2, medical treatment plus drainage 4.74 + 1.59 vs. Group 3, medical plus surgical treatment 2.08 + 1.40; p = 0.141). However, a significant difference was observed between medical treatment and the other two groups in terms of abscess diameter (3, (53 + 1.49 vs. 7.16 + 1.32 vs. 6.27 + 1.01, respectively, p < 0.001).
Relationship between Kallistatin Values, Abscess Diameter, and Method of Treatment of TOA
Statistically significant.
At ROC analysis (Fig. 1), the area under the curve (AUC) was determined at 0.746, with a serum kallistatin cutoff value of 2.81 (95% confidence interval [CI]: 0.609–0.862, sensitivity 73%, specificity 64%, [p = 0.002]). The positive predictive value of serum kallistatin was calculated as 66%, and the negative predictive value was calculated as 61% (Table 3).
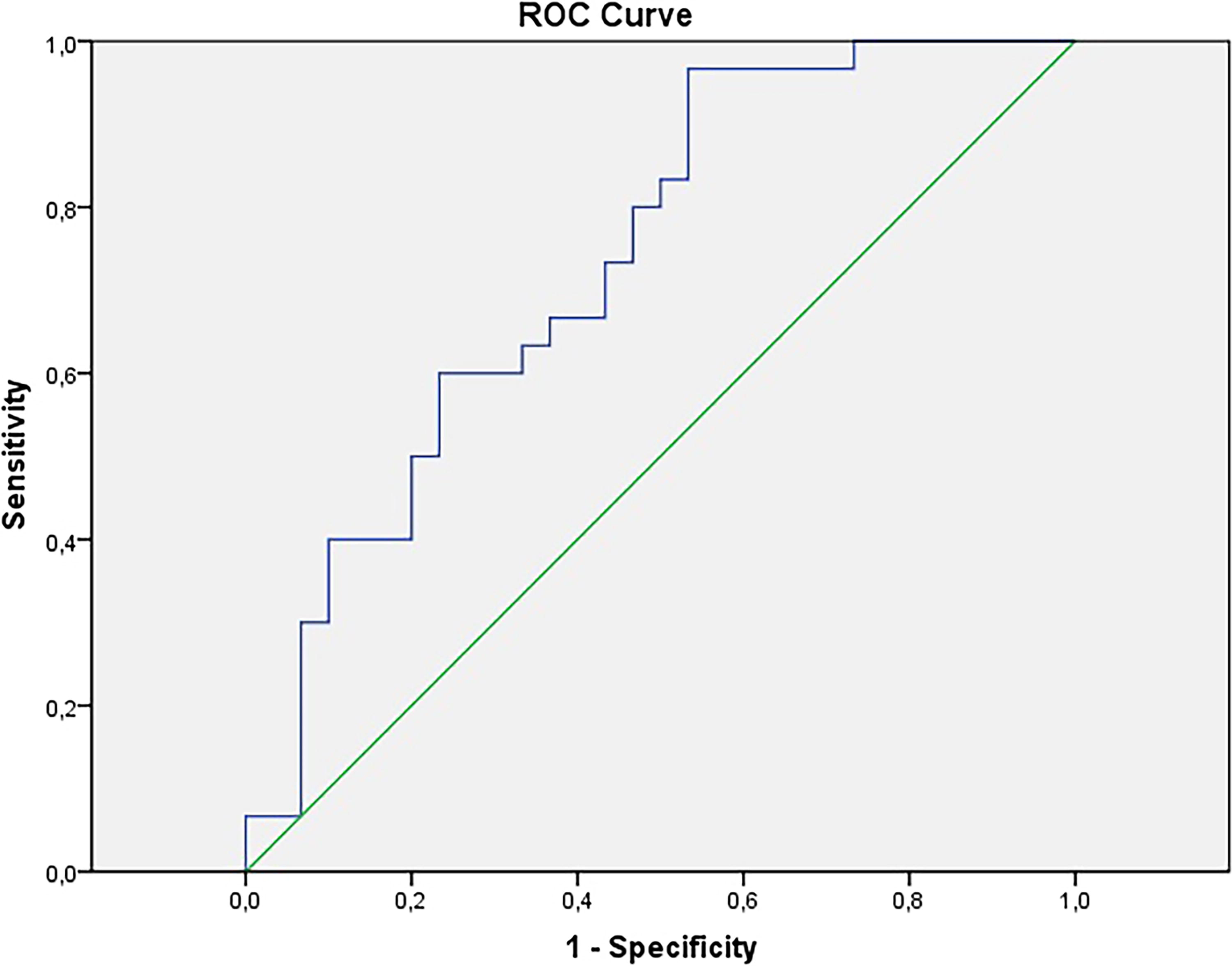
ROC analysis for kallistatin.
Kallistatin Sensitivity, Specificity, Positive Predictive, and Negative Predictive Values
Statistically significant.
AUC = Area under the curve; CI = Confidence interval; PPV = positive predictive value; NPV = negative predictive value.
Weak negative correlations were observed between serum kallistatin levels and age (r = −0.405; p = 0.026) and abscess diameter (r = −0.42; p = 0.019), and a strong negative correlation was also detected between serum kallistatin and CRP levels (r = −0.932; p < 0.001) (Table 4).
Correlations between Kallistatin with Different Variables
Statistically significant.
CRP = C-reactive protein; r = correlation coefficient.
Weak negative correlations were observed between serum kallistatin levels and age (r = −0.405; p = 0.026) and abscess diameter (r = −0.42; p = 0.019), and a strong negative correlation was also detected between serum kallistatin and CRP levels (r = −0.932; p < 0.001).
Discussion
The study results show that serum kallistatin can be used as a biomarker in the diagnosis of TOA, with a cutoff value of 2.81, 73% sensitivity, and 64% specificity.
Although TOA is seen in women of all age groups, it is mostly observed in those of reproductive age. A previous study reported that cases that developed TOA consisted of women aged 18–65, with an average age of 40.7 ± 8.6. 11 Those authors also reported that 16.9% of patients with TOA were in the postmenopausal period, with rates between 14% and 18% being determined in the previous literature. 11 The average age of the patients in the present study was 37.5 ± 8.53, consistent with the current literature, 20% of whom were in the postmenopausal period.
Numerous studies have shown a strong relationship between TOA and IUD use. Demirtaş et al. reported RIA in 62.5% of patients with TOA, whereas Sezgin et al. reported a rate of 40%.12,13 In the present study, 73.3% of the patients with TOA had IUDs.
Familiarity with the characteristics of the test, such as its physiopathological structure, false-positive and false-negative predictive values, clearance time, and half-life is essential to select a suitable biomarker in TOA. Many biomarkers are used for the diagnosis of TOA, CRP being the best-defined and most used in practice. CRP has a normal plasma level of 0.3–1.7 mg/L. It is thought to increase in response to inflammatory stimulation and is a mediator that initiates the inflammatory process by increasing cytokines. However, CRP elevation can also be present independently of inflammation. It can also increase in elderly patients and patients hospitalized in the intensive care unit for reasons other than sepsis and in conditions such as trauma, burns, acute pancreatitis, inflammatory disease, malignant disease, and myocardial infarction. 14 In addition, the release of CRP may be affected by immunosuppressive drugs, and its sensitivity and specificity vary depending on the threshold values determined by different laboratories. Peiper et al. observed serum WBC, sedimentation, and CRP levels of 57%, 70%, and 71%, respectively, in 120 patients diagnosed with TOA using laparoscopy. Those authors concluded that none of these tests were specific for the diagnosis of TOA. 15 It has therefore been concluded that these tests cannot be used in the definitive diagnosis of TOA but may be useful in supporting diagnosis. A prospective cohort study involving 94 patients with TOA identified CRP levels above 49.3 mg/L as a strong laboratory biomarker in the diagnosis of the condition (85% sensitivity and 93% specificity) and that an increase in a patient’s CRP value may predict the need for surgical intervention. 16 In the current study, the average serum CRP level of the patients with TOA was 240 mg/L.
The innate immune system includes a nonspecific response to the pathogen to control inflammation quickly and effectively. Neutrophils, which comprise 55%–70% of the leukocyte population, are the most important cells in the innate immune system. In the adaptive immune response, dendritic cells capture antigens and present them to lymphocytes. Lymphocytes circulating inactively in the blood become activated following antigen presentation, enabling neutrophils to be activated and reach the inflammatory area more quickly, whereas in the adaptive immune response, the time required for neutrophils to reach the inflammatory area is longer. 17 The NLR value, obtained by dividing the number of neutrophils in the blood by the number of lymphocytes, thus increases significantly in the acute period. Alay et al. found the cutoff value of NLR to be 6.97 (79.1% sensitivity and 57.9% specificity) in predicting surgical intervention in patients with TOA, and the authors claimed that NLR could be an important marker in predicting failure to medical treatment in TOA. 18 The NLR value in the present study is compatible with this information in the literature, at 2.11 ± 0.93 in the control group and 6.18 ± 2.20 in the TOA group.
A study of 318 patients diagnosed with TOA revealed that a diameter greater than 6.5 cm required an invasive procedure in addition to medical treatment. 2 Aksakal et al. showed that a TOA diameter of 6.7 cm and above, and Güngördük et al. a TOA diameter of 8.7 cm and above, required a surgical procedure in addition to drainage and medical treatment.19,20 Similarly, in the present study, TOA diameters of 7 cm and above required an additional invasive surgical procedure. It may therefore be concluded that the likelihood of success of medical treatment decreases as the size of the abscess increases, while the need for surgical treatment rises.
Previous studies involving kallistatin have mostly considered the renal and cardiovascular systems. Pamukçu et al. investigated whether kallistatin plays a protective role in pulmonary arterial hypertension (PAH) in their study of 78 patients. The authors posited that serum kallistatin levels are low in cases of PAH and that it exhibits a protective effect in the disease by repairing vascular damage, inhibiting VEGF and angiogenesis, and exerting strong vasodilator and anti-inflammatory effects. 21 Another study observed that kallistatin levels decreased significantly in rodents with hypertension, sepsis, diabetes, heart and kidney damage, and that serum kallistatin levels also declined in animals with liver disease, diabetic retinopathy, severe pneumonia, inflammatory bowel disease, obesity, and prostate and colon cancer. 22 Serum kallistatin levels are therefore thought to be capable of use as a novel biomarker for a number of diseases. In a clinical study of 42 patients with systemic inflammatory response syndrome (SIRS), 150 patients with sepsis, and a control group of 76 individuals observed for one month in terms of the inflammatory process, kallikrein levels increased in the cases of SIRS, sepsis, and septic shock. Kallistatin acts as an anti-inflammatory agent by inhibiting kallikrein in in vitro septic models. 23 Researchers have suggested that kallistatin may be capable of use in evaluating the diagnosis, severity, and prognosis of inflammation. However, no previous studies have investigated serum kallistatin levels in TOA, and this study is thus original from that perspective.
This prospective case–control study included more sociodemographic and obstetric data than other research in the literature. While greater homogenization between groups and a lower bias rate represent particular strengths of this study, the fact that it was conducted in a tertiary reference center is an important limitation.
In conclusion, this study shows that serum kallistatin levels can be used as a biomarker in the diagnosis of TOA. Further studies involving more participants are now needed to test the accuracy of our results.
Authors’ Contributions
Conceptualization (equal): Birsen, Kaba. Writing—original draft (lead): Birsen. Data curation (equal): Erturk, Onder, Eryilmaz, Inal. Investigation (equal): Birsen, Ellidag, Inal. Methodology (equal): Birsen, Ellidag, Inal. Formal analysis (equal): Birsen, Inal. Validation (equal): Birsen, Erturk, Onder, Eryilmaz. Visualization (equal): Birsen, Kaba, Inal. Project administration (equal): Birsen, Kaba. Resources (equal): Birsen, Inal. Supervision (equal): Birsen, Inal.
Funding Information
This research received no external funding or grants.
Footnotes
Author Disclosure Statement
The authors have no conflict of interest to declare.