
Abstract

To the Editor:
Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas, also known as pleomorphic carcinoma of the pancreas with osteoclast-like giant cells, is a special subtype of pancreatic ductal carcinoma and is very rare. 1 Herein, we report a case of undifferentiated carcinoma with osteoclast-like giant cells of the pancreas concurrent infection.
A 50-year-old female, presented with abdominal pain and fever, mainly manifested as epigastric distending pain with a temperature of 38.5°C. The patient subsequently underwent enhanced abdominal CT examination, and the results showed a large and small cystic solid mass about 5.0 × 4.8 × 6.0 cm in size at the tail of the pancreas, with poorly defined boundaries and obvious solid parts and enhancement (Fig. 1).
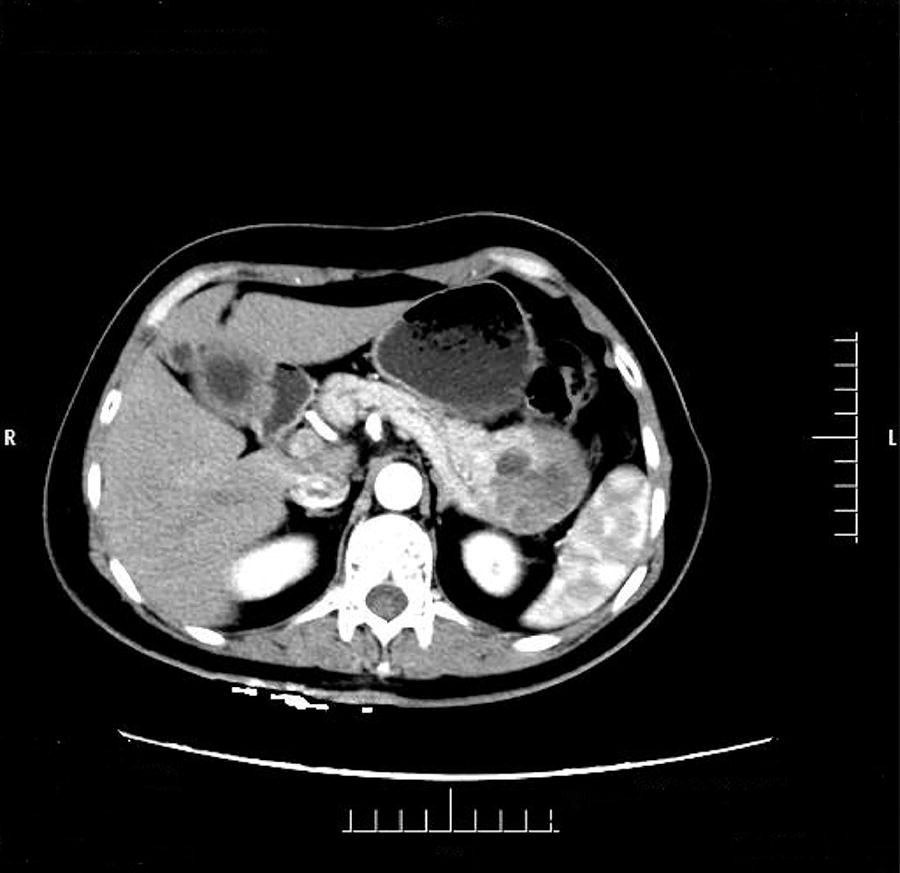
Abdominal CT examination and the results showed a large and small cystic solid mass about 5.0 × 4.8 × 6.0 cm in size at the tail of the pancreas with poorly defined boundaries and obvious solid parts and enhancement.
As the possibility of a malignant tumor could not be ruled out, the patient underwent surgery, during which a solid cystic mass containing white pus was found at the tail of the pancreas. The histopathological diagnosis was undifferentiated carcinoma with osteoclast-like giant cells of the pancreas (Fig. 2). The results of culture of pus were Escherichia coli. The patient recovered well after five days of symptomatic anti-infection treatment, and no obvious abnormalities were observed during follow-up.
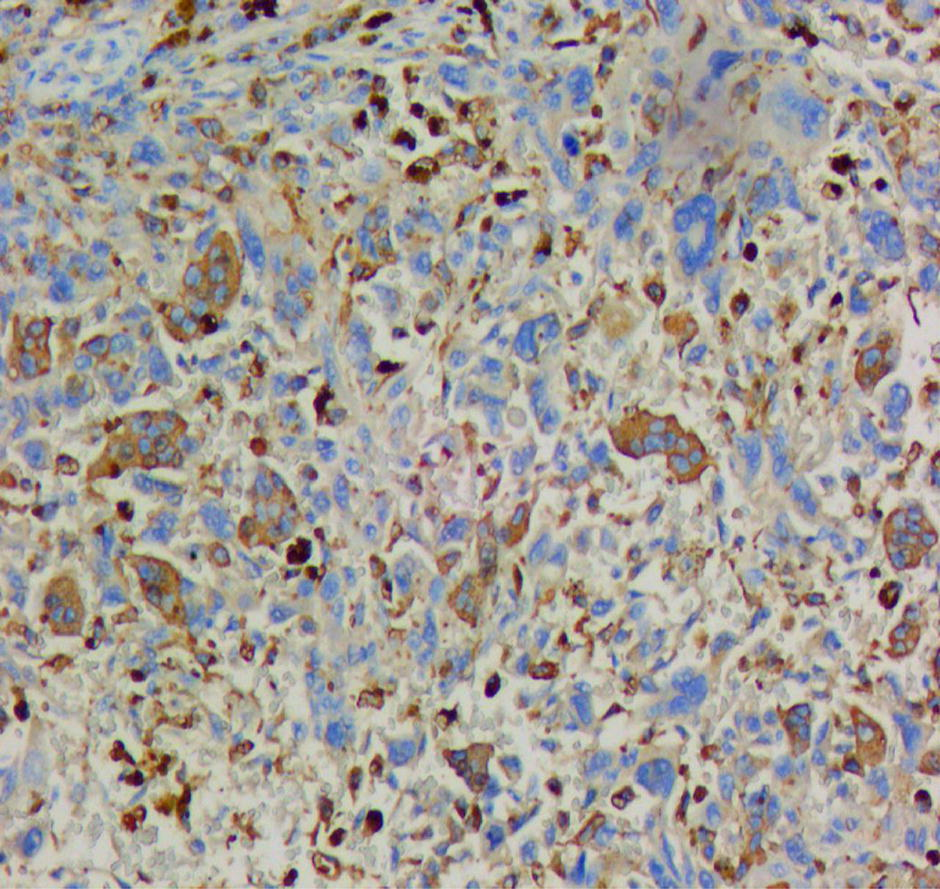
Postoperative histopathological diagnosis was undifferentiated carcinoma with osteoclast-like giant cells of the pancreas.
Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas is a rare and specific subtype of pancreatic ductal adenocarcinoma, accounting for about 1% of pancreatic malignancies. 2 The disease mainly occurs in middle-aged and elderly men and has no specific symptoms in the early stage. It usually occurs in the tail of the pancreas and grows rapidly. The clinical manifestations are abdominal pain and abdominal discomfort. 3 The disease lacks specific manifestations and is easily misdiagnosed. The diagnosis often depends on histopathological examination after surgery. Surgical resection is the main treatment for this disease. For patients with fever, the possibility of coinfection should be considered. Empirical anti-infective treatment can be performed before surgery, and targeted anti-infective treatment can be performed through bacterial culture after surgery.
Ethics Approval and Consent to Participate
Informed consent from patients was obtained for this study, and their anonymous information will be published in this article.
Footnotes
Author Disclosure Statement
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was received for this article.