
Abstract
Background:
Surgery ward caregivers are responsible for educating patients about the pre-operative shower (POS), assisting with the shower as necessary, and evaluating skin cleanliness before transport to the operating theater to mitigate the risk of surgical site infections.
Aim:
To describe the knowledge, attitudes, and declared practices of surgery ward caregivers concerning the POS.
Methods:
A multi-center prospective survey was performed on a random sample of nurses and nurse assistants from five French surgical facilities. Caregivers were asked about their training regarding POS, their ward protocol, knowledge of current French guidelines, attitudes, self-reported practices, and challenges pertaining to the POS.
Results:
All selected caregivers agreed to participate. Of the 72 respondents, 39% declared having received POS-related initial training, whereas 49% indicated the presence of a POS protocol within their ward. Both nurses and nurse assistants reported a lack of clear delineation in their tasks regarding the POS. Knowledge of the existing POS guidelines was found suboptimal, with superfluous precautions wrongly deemed mandatory. With regard to personal practices, caregivers highlighted the need to tailor communication to the patient’s age, dependence, and body size. The predominant declared method for assessing skin cleanliness was verification of POS completion, occasionally supplemented by visual inspection of the incision site. Skin cleanliness assessment was poorly organized and perceived as intrusive by caregivers, especially for surgical procedures involving genital areas, with the patient’s gender markedly impacting this perception.
Discussion:
This survey corroborates substantial deficiencies in POS process training, implementation, and caregiver perceptions.
Surgical site infection (SSI) continues to be a predominant cause of morbidity and mortality in surgical procedures.1–4 International guidelines recommend to take a pre-operative shower (POS) as the first step of skin preparation.5–8 French guidelines, promulgated in 2013, are still currently in force and therefore were used as reference in the present survey. They permit the use of either non-antiseptic soap or antiseptic agents such as chlorhexidine or povidone iodine for the POS. 5 Should the skin be found unclean at arrival at the operating theater, these guidelines mandate in situ cleansing of the incision area within the operating room, a measure that can be challenging if not anticipated. To ensure the efficacy of the POS, caregivers must verify that patients understand how to perform their POS and receive the assistance they possibly need to perform the shower. Subsequent to the shower, an evaluation of the patient’s skin cleanliness should be performed before their departure to the operating theater. In France, a state diploma is required to be a nurse or a nurse assistant. The content of the training is defined by regulations and includes training regarding infection control measures for hospital infections.
The POS technique, particularly when non-antiseptic soap is used as authorized by guidelines, may not diverge substantially from that of a routine shower, potentially leading to caregivers minimizing the significance of the POS. Concurrently, the upsurge in same-day surgical procedures, which entail shorter hospital stays, restricts the opportunity for caregivers to explicate POS techniques, assist those who face challenges during showering, or adequately assess skin cleanliness at the patient’s arrival in the ward after a POS at home.
Distribution of caregivers’ roles in POS may vary widely according to the uses and organization of each facility. Typically (although this may vary), during the visit where the operation is scheduled, the surgeon advises the patient to shower but does not describe the particulars of the POS. For POS at home, a leaflet describing these particulars may be given to the patient by the surgeon, or by a secretary, or by a nurse or nurse assistant, according to the facility organization. This leaflet is usually given, without oral explanations, together with other documents regarding the patient’s information and consent for operation and anesthesia. It may be assumed that when the professional giving the leaflet is a health caregiver (as opposed to a secretary), some more precise explanation about the POS technique may be given to the patient, but during our informal exchanges with many professionals of various facilities, these explanations were not formalized in a proceeding and were left to the goodwill of each health caregiver. French guidelines currently in force recommend “at least one POS,” “as close as possible to the surgical procedure,” which leaves room for interpretation. The survey by Verjat-Trannoy et al. showed that most facilities recommend in their local protocol a POS the evening before and the morning of the procedure. 9 Whether the patient has a same-day operation or is an inpatient, the evening shower (if required) may be taken at home or in the hospital, and the same applies for the morning shower. When the POS is performed at home, patients suffering from physical or cognitive disabilities may be helped for POS by a nurse or a nurse assistant if ordered by the surgeon. When the POS is performed in the hospital, ward caregivers (either nurses or nurse assistants) ask the patient to take the POS, either in a single or shared bathroom, and explain the specific steps of the POS procedure. During our informal exchanges with professionals before undertaking the survey, they explained that these explanations were not always protocolized. Disabled patients are supposed to be helped to shower, but no formal assessment of disability is performed in wards, so again help varies according to caregivers. Adequate skin cleanliness after a shower should be attested by caregivers before the patient’s departure, which may represent a substantial workload when many patients depart at a close time to the operating room. In summary, POS may be explained by the surgeon, a secretary, a nurse, or a nurse assistant either in the hospital or at home, and POS may take place in the hospital and at home. Disabled patients may be helped by hospital or home caregivers, and skin cleanliness must ultimately be assessed by ward caregivers before the patient is transferred to the operating room.
Our previous survey revealed that patients generally reported satisfactory experiences with the POS process, which included the quality of information provided; however, they noted difficulties in deciphering written instructions on POS. 10 Interestingly, they also disclosed that a proportion of healthcare professionals did not perform post-POS skin cleanliness assessments, with only 17% of patients testifying to visual evaluations conducted by caregivers before being transported to the operating theater.
The rationale for the omission of skin cleanliness assessment, despite its criticalness for antiseptic procedures at the incision site, is not well elucidated. Possible explanations include a lack of ward nurses’ expertise in skin preparation for an operation compared with their counterparts in the operating rooms, absence of explicit protocols mandating visual assessments, scarcity of time, or a belief that such evaluations are unnecessary, compounded by discomfort in potentially embarrassing patients, as suggested by prior surveys among surgical ward caregivers. 9
Therefore, to better understand the factors contributing to a less-than-optimal POS process, we undertook a multi-center survey of surgical ward caregivers to describe their knowledge, attitudes, and declared practices regarding this POS process.
Patients and Methods
Population
The survey was conducted among surgical facilities of an infection control network in Northern France. Managers of the eight surgical facilities of the network were contacted; five (two publicly funded, one non-profit private, and two private for-profit) consented to the participation of their facility in the survey. All participating facilities had a leaflet available explaining the technique of the POS, and all wards had a protocol for POS. Both day-surgery and conventional surgery wards were represented. The subjects of the survey were nurses and nurse assistants employed in the surgical wards. For each participating institution, a comprehensive roster of these professionals was compiled, and a random sample of one-third of the nurses and one-third of the nurse assistants was selected for participation. The selected professionals were then approached for consent to partake in an interview regarding the POS. Anonymity of their answers was guaranteed.
Pre-arranged individual interviews with consenting nurses and nurse assistants were coordinated by the managers of each facility.
The questionnaire, administered in person by trained researchers, encompassed queries about sociodemographic profiles, POS-specific training of caregivers, whether a leaflet was available for patient’s information on the POS, the existence and particulars of a POS protocol within their ward, as well as assignment clarity within the ward concerning tasks related to the POS briefing, assistance, and skin cleanliness assessment. Then, participants were asked if they were personally involved in the management of patients for the POS. If not, the interview stopped there. Affirmative responses prompted further questions about their knowledge of current French POS guidelines, opinion, and declared practices concerning the POS.
In relation to guidelines knowledge, caregivers were queried on the purpose of the POS, the recommended products for showering, the recommended timing of the POS, and whether the entire body or only the surgical site was to be cleansed, including the necessity of pre-operative hair shampooing.
Regarding their perceptions, they were consulted on their beliefs about the POS importance for patient safety, the assessment of skin cleanliness before operating room transfer, and how patients might perceive this evaluation.
Concerning the usual practice in their ward, participants were asked whether the shower was to be documented within the patient’s health record.
As for their own individual practice, caregivers were asked whether they usually explained the shower orally, with a leaflet, both, or neither, and whether their explanations varied based on patient characteristics, such as age, gender, body weight, autonomy, or linguistic ability. They were also questioned about any encountered challenges in conveying the shower instructions and what could potentially enhance patient’s information on this subject. They were then asked if some patients were reluctant to shower, and in that case what tactic they used to have them shower nevertheless, the nature of difficulties some patients faced during showering, and the provision of physical assistance for the POS. Regarding skin cleanliness assessment, participants were asked about their method for performing this assessment and whether there were patient characteristics such as age, gender, body weight, autonomy, or linguistic ability that affected their assessment approach.
They were asked if they felt that this assessment was sometimes difficult and why (especially for some specific surgical procedures), and how, in their opinion, skin cleanliness assessment by caregivers was perceived by patients. Reasons for difficulties and types of perception by patients were free text from caregivers and were not proposed in the questionnaire. Caregivers were asked if they recorded the result of the skin cleanliness assessment in the patient’s file. Eventually, they were asked their suggestions to improve the POS, including making skin cleanliness assessment easier and more effective.
The questionnaire was elaborated by the authors with input from a panel of surgery ward nurses and infection control nurses. Completion time for the questionnaire was approximately 20 minutes.
Statistical analyses
Data were entered and analyzed utilizing Microsoft® Excel 2000 (Microsoft Corporation, Redmond, WA). Qualitative variables were described via their frequency distribution, accompanied by 95% confidence intervals. Proportions were compared using a chi-square test.
Ethics
The protocol of the survey was approved by the Rouen University Hospital Institutional Review Board CERDE (Comité d’Ethique pour la Recherche sur Données Existantes) with the reference number CERDE E2025-10.
Results
A total of 72 caregivers from five surgical facilities participated in the interviews. No one refused to participate. Two respondents acknowledged no personal involvement in the POS process hence abstained from responding to subsequent POS-related inquiries. Respondent characteristics are described in Table 1.
Characteristics of Surgery Ward Caregivers Participating in the Survey Regarding the Pre-Operative Shower Process in Surgery Wards
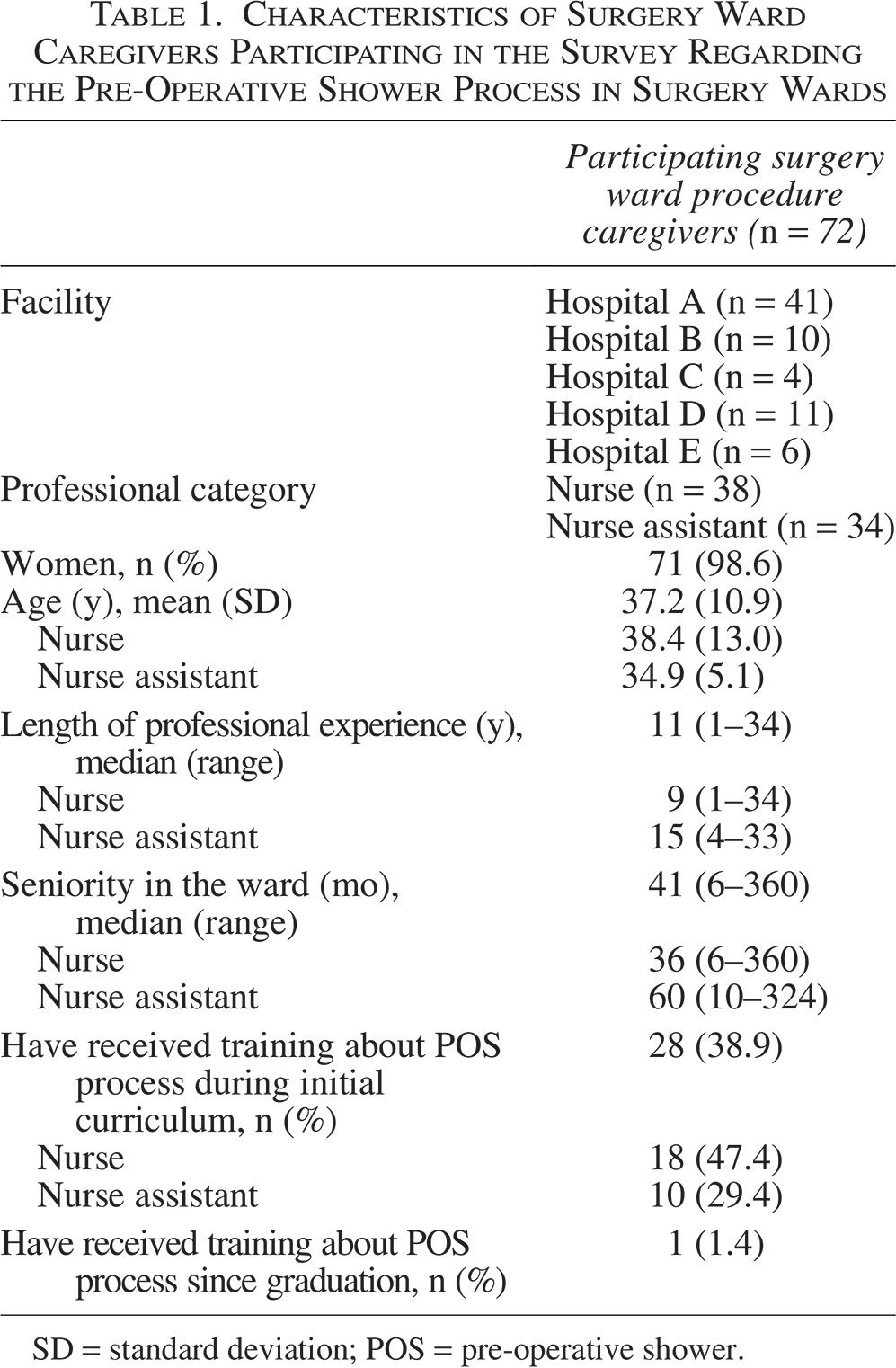
SD = standard deviation; POS = pre-operative shower.
All but one of the interviewees mentioned receiving training during their initial curriculum, with only a single nurse mentioning training about POS during continuing education (Table 1). Only 35 (48.6%) surgery ward caregivers declared that a POS procedure was available in their ward.
The distribution of tasks regarding the POS process within the wards, as reported by the participants, is described in Table 2. Briefing the patients about the POS, assisting them if necessary, and assessing skin cleanliness after POS were mainly carried out indifferently by nurses and nurse assistants.
Distribution of Tasks Regarding the Pre-Operative Shower Process in Surgery Wards as Declared by Participants (n = 72)
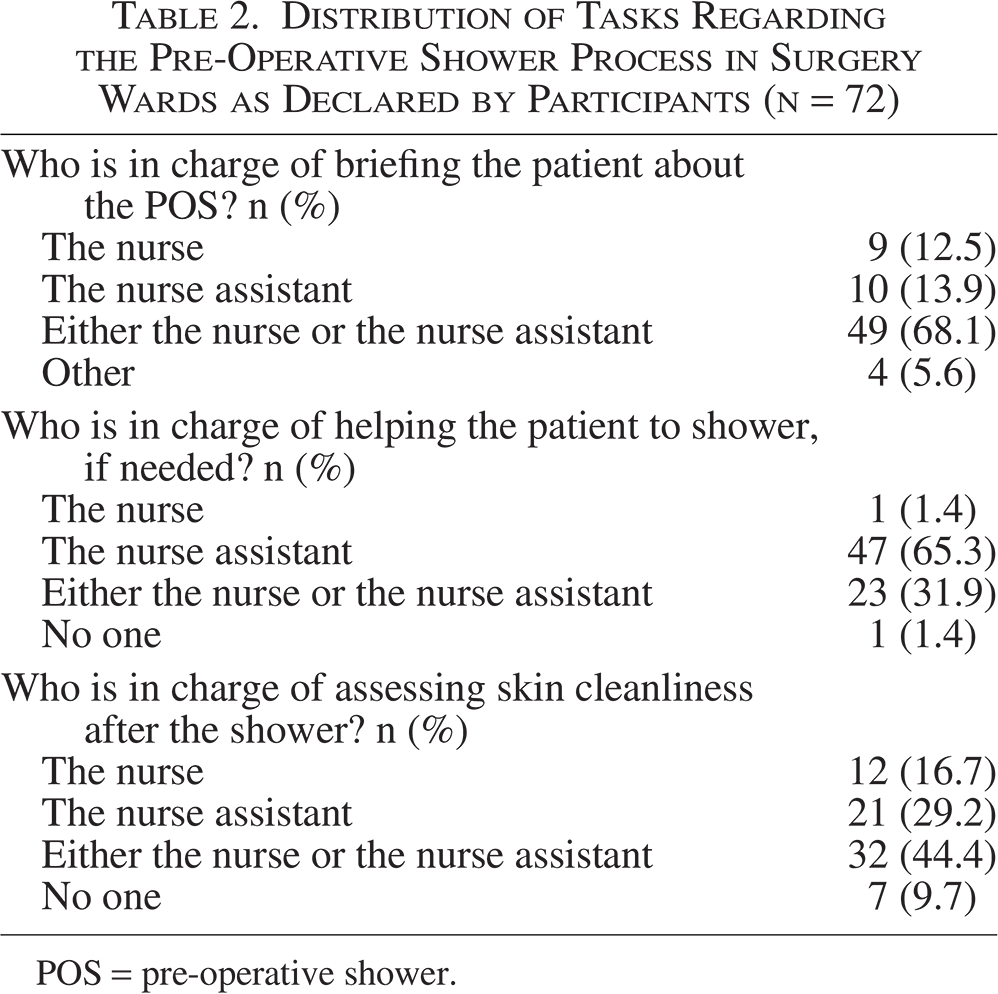
POS = pre-operative shower.
Table 3 details the knowledge, attitudes, and declared practices of surgery wards caregivers regarding the POS. Knowledge regarding the purpose and the technique (except for the part of the body to be showered) was suboptimal. However, almost all caregivers considered the POS and the assessment of skin cleanliness after POS as important for patient’s safety. Among the three caregivers who stated that they do not consider POS an important step for surgical procedure patient safety, only one provided an explanation, stating that it is not important because antisepsis will be performed in the operating room. The reasons mentioned by the four caregivers, who did not consider it important to assess skin cleanliness before the patient went to the operating room (OR), were that they thought it was sometimes not necessary according to the patient’s appearance or autonomy (n = 3), or because the assessment would be performed in the OR (n = 1).
Knowledge, Attitude, and Declared Practices of Surgery Ward Caregivers (n = 70) Regarding the Pre-Operative Shower (POS) (Regarding “Knowledge” Section, Correct Answers According to French Sf2h 2013 Guidelines Appear in Bold Characters)
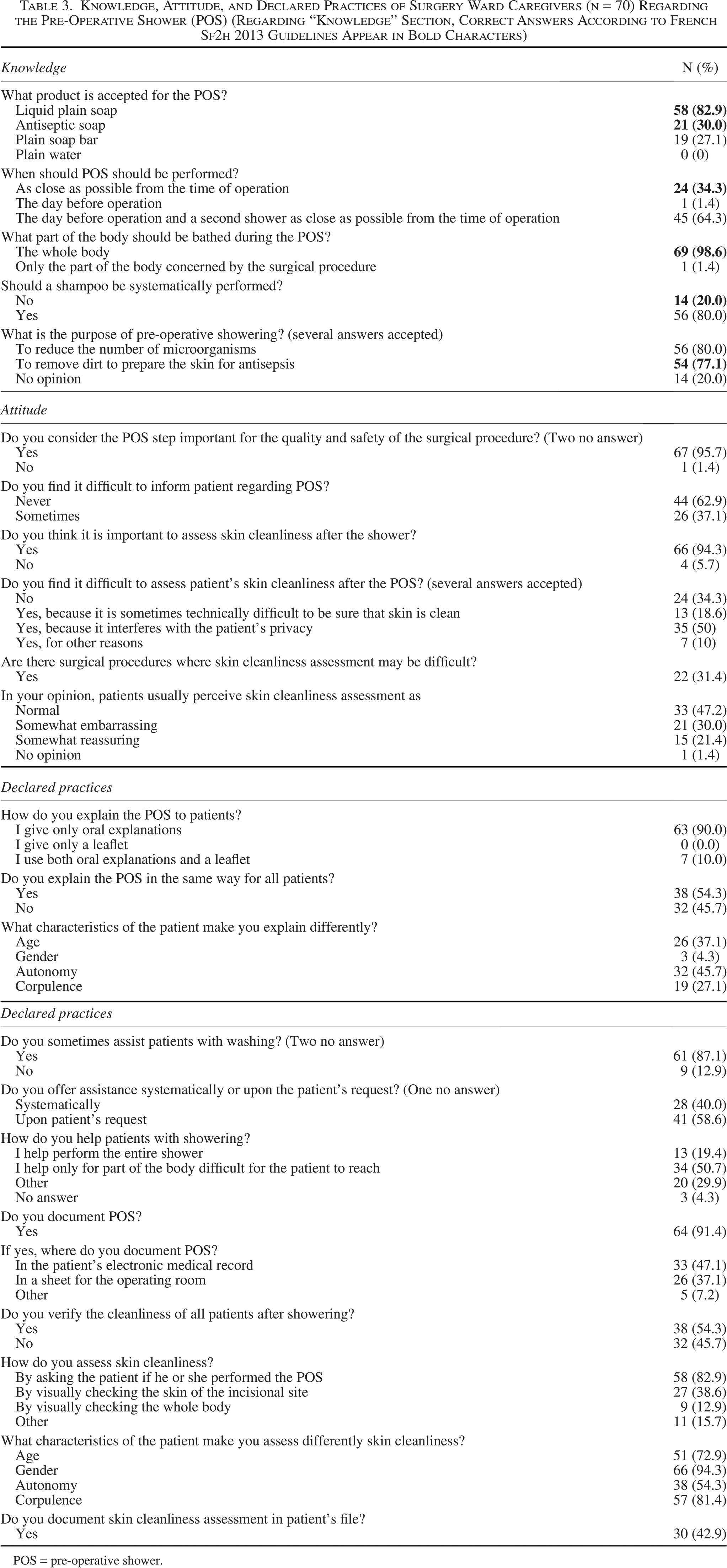
POS = pre-operative shower.
Caregivers commonly reported difficulties in confirming genuine skin cleanliness, with nearly a third of them perceiving patient embarrassment during such evaluations. Caregivers explained that they considered a thorough visual skin cleanliness assessment a violation of the patient’s privacy. Among the 22 (31.4%) caregivers indicating greater difficulty in assessing skin cleanliness for particular types of operation, 21 cited procedures implicating anal or genital areas as the principal challenge. Overall, 28 (40.0%) caregivers reported having ever experienced an uncomfortable situation during skin cleanliness verification. About one-third of caregivers also thought that patients considered skin cleanliness assessment as something embarrassing.
Proposed enhancements for patient information about the POS were the distribution of leaflets (n = 40, 57.1%), deployment of informative posters in patient rooms and/or shower cubicles (n = 12, 17.1%), and the provision of verbal guidance upon patient admission to the ward (n = 6, 8.6%). Caregiver’s propositions to facilitate skin cleanliness assessment included the introduction of a structured checklist of body parts to be assessed (n = 7, 10.0%), a protocol revision to remind caregivers to warn the patient, before POS, that cleanliness will be assessed (n = 7, 10.0%), and the need for increased time allocation for thorough evaluations (n = 7, 10.0%). However, 43 (61.4%) caregivers offered no suggestions for improving skin cleanliness assessment.
Discussion
This is the first survey, to our knowledge, providing an insight on the POS process, a most important step of skin preparation before a surgical procedure, from the point of view of surgical ward caregivers. Its findings suggest that POS is not always a smooth process.
First, half of the interviewed caregivers mentioned the absence of a POS protocol within their ward, whereas all facilities had in fact a protocol available. Noteworthy, similar tasks regarding the POS were assigned to nurses and nurse assistants in the ward, which may suggest that the caregiver’s tasks regarding POS are not considered as “nurse-level.”
Second, it is somewhat surprising that a substantial proportion of caregivers claim to lack specific POS training during the initial curriculum, considering that prevention of SSI is part of the national curriculums. This result could be explained either by a true lack of training or by a bad recall of the training received, understandable as the mean time because the caregiver’s graduation was 11 years in our survey. Noteworthy, further analysis of the initial nurse’s and nurse assistant’s curriculum programs shows that these programs do not precisely define the knowledge to be acquired by students regarding the prevention of SSI, with items “Identify infection control procedures used in hospitals and provide arguments to explain their use” and “Identify risks related to therapeutic and examination activities and determine appropriate preventive and/or corrective measures” in the nurse’s program and “Care for a person undergoing surgery or non-invasive intervention in collaboration with the nurse” in the nurse assistant’s program.11,12 The formulation of these items leaves an important margin of freedom to schools to decide what SSI control measures should be taught to students. A nationwide survey of these schools would be helpful to better understand what is really taught. The lack of training on POS in continuing education, however, is more difficult to explain by a lack of recollection of the training received, as the latter would logically be more recent.
Given these results regarding training, it is somewhat not surprising that most caregivers in our survey had an imprecise knowledge of the purpose of POS and believe nearly equally that it is done to remove dirt and to decrease skin microbial load, when French guidelines from 2013 insist strongly that POS aims to remove dirt to permit efficient antisepsis in the OR and does not aim to decrease the microbial load on the skin. 5
Taken together, these two results suggest that surgery ward caregivers could benefit from training regarding skin preparation before an operation, including POS.
Third, although the caregivers’ knowledge was not optimal, identified deviations erred on the side of excessiveness, such as mandating two showers, the exclusion of plain soap, and mandatory shampooing—stipulations exceeding those elucidated by the prevailing French guidelines. 5 These findings align with a recent survey by Verjat-Trannoy et al., which gauged the integration of the 2013 French guidelines on skin preparation within local surgical facility protocols. 9
Regarding patient’s information, caregivers frequently noted challenges in conveying information to patients and the necessity to modulate communications based on patient characteristics. This difficulty in conveying information about the POS related by caregivers contrasts with findings from our prior survey of patients having undergone a surgical procedure, where patients, on the contrary, expressed satisfaction with the POS-related information they had received. 10 This discrepancy would suggest either an overestimation by caregivers of patients’ comprehension difficulties or an unconscious miscomprehension of information by patients.
Our most problematic finding pertained to the difficulty reported by caregivers in evaluating skin cleanliness. This is noteworthy, as caregivers are generally experienced in intimate care. Putting the reported challenges together, it seems unsurprising that the majority of skin cleanliness assessments are conducted as could be described superficially, if not outright omitted, and when performed, are restricted solely to inspecting a limited part of the body (the incisional site).
This finding regarding the fragility of skin cleanliness assessment aligns with the results of our previous surgical patient-directed survey, where a mere 17% reported visual cleanliness checks by caregivers. 10 The rationale for the omission of skin cleanliness assessment, despite its criticalness for antiseptic procedures at the incision site, is not well elucidated. Possible explanations include a lack of ward nurses’ expertise in skin preparation for a surgical procedure compared with their counterparts in the operating rooms, the absence of explicit protocols mandating visual assessments, scarcity of time, or a belief that such evaluations are unnecessary, compounded by discomfort in potentially embarrassing patients, as suggested by prior surveys among surgery ward caregivers. 13 Regarding this last hypothesis, our previous qualitative study suggested that the perceived ordinariness of the POS, akin to daily showers, led caregivers to view their assessment of post-POS cleanliness as a judgment on the individual’s personal hygiene, a role they felt unqualified to assume. 13 A parallel narrative emerged in the present survey, where caregivers expressed concern over intrusiveness and the potential discomfort caused to patients. Notably, this apprehension was not echoed by patients in the preceding survey, who instead declared they felt that the visual cleanliness assessment was reassuring. 10 The “organizational ambiguity” (absence of protocols, unassigned responsibility for cleanliness assessment) unveiled by caregivers may also stem from their discomfort with this aspect of care, prompting them to avoid working as a team to enhance organizational proficiency of skin cleanliness assessment within the ward. Conversely, this ambivalence could partly explain the low rate of assessments conducted.
Our survey has some limitations. Conducted in a single region of France, its generalizability to other regions of France or other countries may be constrained. However, we included facilities of diverse funding types, performing elective or unscheduled surgical procedures across varied surgical specialties, and accommodating both day and traditional surgical procedures. Literature suggests no geographic variance in knowledge, views, or practices in surgical pre-operative care. Consequently, we hypothesize that our findings accurately reflect the context of the POS in France. Another consideration is the interview mode—face-to-face—which may have influenced responses because of social desirability bias. Mitigation efforts included engaging external interviewers and assuring participant anonymity. In addition, desirability bias should have led participants to give answers along the lines of what was expected, and therefore, our result reporting approximately 13% of visual checks of cleanliness is probably overestimated.
The study’s robustness stems from the randomized participant selection with a 100% response rate. This response rate was achieved both by the subject of the survey, which participating caregivers were eager to discuss with the interviewer, and by the guarantee of anonymity. This 100% response rate permitted us to avoid selection bias and to provide an authentic insight into the operational dynamics of the POS.
In conclusion, this survey suggests that skin cleanliness assessment following the POS is most of the time indirect and relies on the patient’s declaration rather than on direct assessment by caregivers. However, our work was not designed to assess if an indirect cleanliness assessment was indeed associated with an impaired level of skin cleanliness in the operating room, although this could be an undesirable logical consequence of a non-direct assessment. With the increase of day operation and the growing trend of same-morning admissions for non-day operation, the POS is progressively relegated to a home-based task unaided by medical professionals. Therefore, imparting comprehensive information on POS procedures and meticulous scrutiny of skin cleanliness becomes a pivotal safeguard in ensuring that patients enter the operating theater with appropriately prepared skin, reinforcing patient safety imperatives. A greater investment in caregiver education, standardized POS protocols, and improved ward organization would be useful in enabling surgical ward caregivers to effectively perform this critical safety evaluation, thereby contributing to the diminution of SSI risks.
Authors’ Contributions
A.C.: Validation, data curation, formal analysis, and writing—original draft. J.M.: Investigation and formal analysis. M.C.: Investigation. M.L.: Writing—review and editing. H.M.: Conceptualization, methodology, and writing—review and editing. V.M.: Conceptualization, methodology, and writing—review and editing.
Footnotes
Acknowledgments
The authors warmly thank the participating surgical facilities, their infection control teams, and the healthcare givers who agreed to participate. They also thank Amin Naymaa for his help in data collection and Alice Manchon for her help in editing the article.
Author Disclosure Statement
The authors declare they have no conflicts of interest regarding this survey.
Funding Information
This survey has not received any funding.