
Abstract
Objective:
The objective of this study was to describe the clinical and microbiologic characteristics of adult patients with HIV infection and splenomegaly treated with splenectomy.
Methods:
We conducted a retrospective study, including patients with the diagnosis of HIV and splenomegaly treated with splenectomy between 2005 and 2023.
Results:
We included 20 patients with a mean age of 36 years (±2), with a predominance of males (n = 18). Some patients had more than one condition associated with splenomegaly. The following were considered as the indication for splenectomy: Splenic abscesses in 13 (65%), refractory thrombocytopenia in 9 (45%), symptomatic splenomegaly in 5 (25%), and splenic lymphoma in 1 (5%). After operation, spleen samples were sent for microbiology culture, displaying the invasion of bacteria in 11 (55%), fungi in 8 (40%), and viruses in 8 (40%). When evaluating the indications for splenectomy between groups, splenic abscesses were more present in those patients without active treatment (83% vs. 38%, p = 0.035), whereas symptomatic splenomegaly presented more frequently in those with active antiretroviral therapy (ART; 63% vs. 0%, p = 0.004).
Conclusions:
The cornerstone of treatment for patients with splenomegaly should initially focus on adherence to ART and addressing the underlying cause. However, when the condition is refractory splenectomy may be indicated.
With advanced HIV infection, established acquired immunodeficiency syndrome (AIDS), and a depleted number of CD4+, complications such as infections and neoplastic conditions become the common ground for patients. 1 Although, with the use of antiretroviral therapy (ART), disease control has become suitable for most people, some organs continue to serve as reservoirs for HIV, such as the case of the spleen. It has been demonstrated that in people living conically with HIV, the virus persists in this organ, particularly within dendritic cells and B cell follicles, even with active ART. 2
Invasion of the spleen by HIV may present clinically as splenomegaly, which is present in up to 66% of people living with HIV. 3 This organ has fundamental functions in hematopoiesis and in immunity, as it contains about one-quarter of the body’s lymphocyte reserve, serving as an immunogenic organ with functions in adaptive and innate response.4,5 The leading causes of splenomegaly include congestion, infiltrative processes, and hypertrophy, which play an important role in patients with chronic infections, such as in those with HIV. 6 If left untreated, patients with splenomegaly may suffer from complications such as splenic rupture and sepsis. 7
In most cases, treatment for splenomegaly may be limited to ART and management of secondary causes that may be associated. Nevertheless, when splenomegaly becomes painful or refractory to medical therapy, splenectomy can be considered. 8 Although splenectomy is effective, high-risk complications, such as sepsis, may present, particularly in patients with a deficient immune response. 8 The objective of this study was to describe the clinical and microbiologic characteristics of adult people with HIV infection and splenomegaly treated with splenectomy.
Patients and Methods
Our research project was approved by the Ethics and Research Committee of the Instituto Nacional de Enfermedades Respiratorias with the following approval number: C80-24, and followed the Code of Ethics of the World Medical Association (Declaration of Helsinki). We conducted a retrospective study, including people with the diagnosis of HIV and splenomegaly between 2005 and 2023. Patients underwent treatment for splenomegaly at the Thoracic Surgery Ward of the Instituto Nacional de Enfermedades Respiratorias in Mexico City. We conducted a review of clinical files retrieving demographic data, date of HIV diagnosis, treatment status, CD4+ count, viral load, comorbidities, and microbiologic findings of the spleen. Splenomegaly was defined as a spleen weighing >200 g and a size of ≥12cm on its longitudinal axis. 4 Active ART therapy was defined as a re-start in the previous 3 months. Alcohol consumption was defined as more than 14 units per week. All of the patients underwent splenectomy through an open approach (Fig. 1).
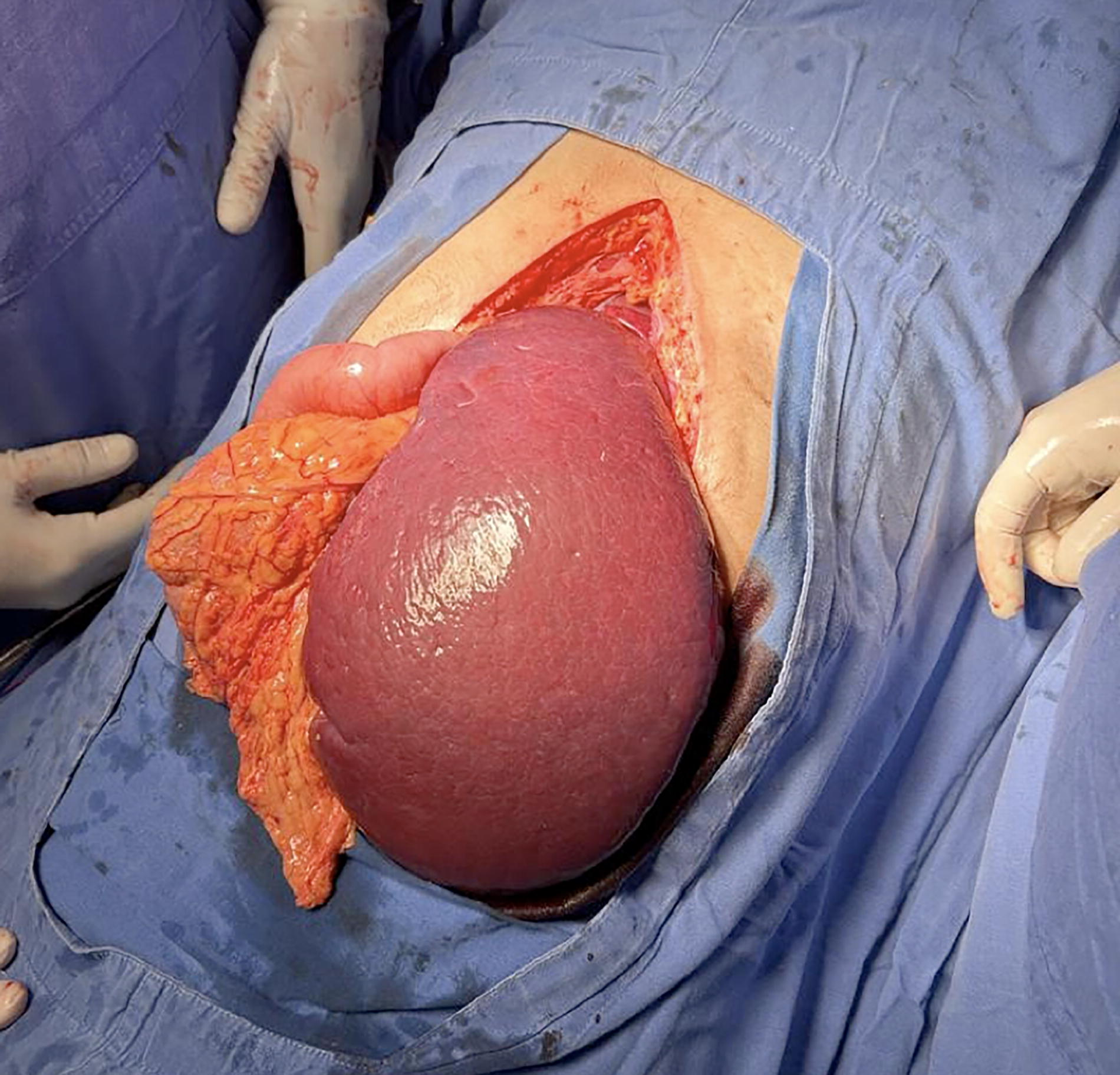
Medial laparotomy with an oversized spleen coming out of the incision site.
Statistical analysis
Categorical parameters were represented as frequencies with percentages (%), whereas continuous data were presented as the variable mean and standard error or median and interquartile range when data were skewed. Data distribution was ascertained by the Shapiro-Wilk test. For bivariate analysis, data were compared with Student’s t-test for parameters with a normal distribution or Mann-Whitney U, Pearson’s Chi-squared, and Fisher exact test for non-parametric data. Statistical analysis was conducted using SPSS version 25.0 (SPSS Inc., Chicago, IL, EE. UU.). We took into account a p-value <0.05 to define statistical significance.
Results
We included 20 patients with a mean age of 36 years (±2), with a predominance of males (n = 18). Patients were admitted with a median time from HIV diagnosis until splenectomy of 320 days (208–3121). Forty percent (n = 8) of the patients had an additional diagnosis of Mycobacterium tuberculosis (MbTb) infection, whereas 10% (n = 2) were diagnosed with an active M. avium infection. In addition, 10% (n = 2) had a diagnosis of type 2 diabetes mellitus, 55% (n = 11) had a history of alcohol consumption, and 45% (n = 9) were current or past intravenous drug users.
Regarding HIV treatment, eight patients (40%) had an active status of ART, although the median CD4+ and viral load were 45 cells/mm3 (19–78) and 5,764 copies (0–23,000), respectively. Before the surgical intervention, the diagnosis was confirmed with an abdominal ultrasound. Surgical indications are detailed on Table 1. In those patients with refractory thrombocytopenia, the mean platelet count was 26 × 109/L.
Indications for Splenectomy in People Living with HIV
Some patients had more than one condition associated with splenomegaly (included patients = 20).
The median blood loss during surgical procedure was 275 mL (200–962), with an average spleen size of 157 mm (±9) and a median spleen weight of 375 g (287–934). Following the surgical procedure, three patients (15%) developed sepsis, which ultimately led to their deaths.
After resection, spleen samples were sent for microbiology culture, displaying the invasion of bacteria in 11 (55%), fungi in 8 (40%), and viruses in 8 (40%). Most of these were associated with MbTb, Candida albicans, and cytomegalovirus, respectively (Table 2). In those patients treated for thrombocytopenia, post-operative platelets rose to a median value of 346 × 109/L (p = 0.004, compared with preoperative values). In those patients without an established diagnosis, antimicrobial therapy was initiated following resection. In our study, hospitalization ranged from 17 to 50 days with a median of 22, without readmissions associated with the surgical procedure after discharge.
Distribution of Microbiologic Findings
CMV = cytomegalovirus; HV8 = herpes virus 8; EBV = Epstein–Barr virus; HBV = hepatitis B virus.
When comparing patients with active ART versus those who were not taking active medication, we encountered an apparent difference in the mean size and weight of the spleen with 194 cm (±29) versus 145 cm (±8) and 929 g (232–1800) versus 350 g (275–619), respectively. In addition, the rate of bacterial invasion was greater in patients without active therapy (66%) compared with those with active therapy (37%), whereas viral invasion was more frequent in patients receiving active therapy (50%) than those without (33%). However, these differences were non-significant. When evaluating the indications for splenectomy between groups, splenic abscesses were more present in those patients without active treatment (83% vs. 38%, p = 0.035), whereas symptomatic splenomegaly presented more frequently in those with active ART (63% vs. 0%, p = 0.004). Comparative results are presented in Table 3.
Patient Demographics Compared Between Active and Non-Active Antiretroviral Therapy
*p significative of <0.05.
ART = antiretroviral therapy; MbTb = Mycobacterium tuberculosis; NS = Non significant.
Discussion
This study analyzed the clinical and microbiologic characteristics of 20 adult HIV-infected people with splenomegaly who underwent splenectomy. In people living with HIV, both hepatomegaly and splenomegaly are an apparent clinical sign of affection to the hematologic system. The latter has been described to be present in 66%–72% of patients with HIV. However, in most scenarios, it is clinically silent. 3 Splenomegaly can be associated in most cases to three causative mechanisms as follows: hypertrophy, infiltration, and congestion. 6 Viral invasion of the spleen appears to be a key cause, as it is related to collagen deposition and fibrosis, although it has also been shown to cause white pulp atrophy. 5 In addition, additive effects by other entities, such as splenic infections, congestion, or infiltration by oncologic conditions, may increase the size of the spleen even further.
Splenectomy may be considered in those who present with splenic rupture, abscesses, refractory thrombocytopenia, clinical splenomegaly, or oncologic invasion, among other causes.8,9 Although splenectomy appears to be a feasible option, patients must be carefully managed and operated on at the appropriate stage of their disease to minimize the risk of post-splenectomy sepsis. This complication, reported in up to 50% of cases in the literature and 15% in our series, often results in fatal outcomes. 10
In people with long-standing HIV infection, depletion of CD4+ cells leads to impaired immunity, rendering them vulnerable to a broad range of pathogens and opportunistic infections. Conversely, individuals who recently restarted ART may experience immune reconstitution inflammatory syndrome (IRIS), a paradoxic deterioration despite effective control of HIV viremia. 11 Both phenomena may explain why some patients in our cohort, despite being on active ART, presented with larger and heavier spleens. In contrast, patients not receiving ART showed a greater incidence of splenic abscesses, likely attributable to the complete loss of normal immune function. This IRIS could also have contributed to the post-operative mortality, as two of the three patients who died were on active ART, but had low CD4+ counts, possibly because of a recent therapy restart.
In our cohort, splenic abscesses were the leading indication for splenectomy, with most cases involving polymicrobial infections. However, MbTb emerged as the predominant pathogen infecting the spleen. This aligns with existing literature, which highlights immunosuppression such as that observed in HIV, malignancies, or post-transplant patients as a significant risk factor for splenic abscesses. 12 Dissemination of active MbTb in patients with advanced HIV has been implicated in splenic infections, with splenectomy often yielding favorable post-operative outcomes.13,14
Regarding the causative agent for the abscess, a recent study showed that the culture of Staphylococcus and Streptococcus was more prevalent in splenic abscesses, which differs from ours in which MbTb was more common. This discrepancy may reflect regional variations in microbiologic profiles and pathogen prevalence. 15 Adding to this, it is essential to point out that in said study, only half of the patients had immunodeficiency, including HIV infection, which predisposes patients to a different set of infections.
Nearly half of our patients presented with thrombocytopenia, a condition reported in approximately 10% of individuals with HIV and up to 30% of those with AIDS and in 45% of our study. 10 This condition may arise from a combination of increased peripheral platelet destruction and reduced production because of HIV-infected megakaryocytes in the bone marrow. 16 Supportive strategies and the initiation or re-initiation of ART are essential in managing HIV-associated thrombocytopenia, although splenectomy may be considered, as it has shown to be curative in up to 50% of patients refractory to medical treatment.17,18 In our cohort, all patients achieved normal platelet levels within one month post-splenectomy. Nevertheless, and as previously mentioned, splenectomy should be done in a timely manner to prevent complications.
It is essential to highlight the substantial gender differences in our study, with a male-to-female ratio of 9:1. This variation may be linked to differences in treatment adherence between men and women. As highlighted in the study by Linghua et al., the authors found that women living with HIV tend to have better treatment adherence compared to men. 19 However, the regional HIV prevalence in Mexico, where 84% of cases are in males and 16% in females, may better explain the results observed in our study. 20
As highlighted by Devanathan et al., the introduction of ART has substantially enhanced both the life expectancy and quality of life of individuals living with HIV, bringing them closer to those of non-HIV individuals. 5 However, nearly 40 years since the advent of ART, treatment adherence remains a major challenge for many. 21 Notably, there is a limited number of studies evaluating the outcomes of people living with HIV undergoing splenectomy, with most research predating the ART era, likely reflecting the lack of well-established diagnostic and therapeutic protocols during that time.17,22,23
Despite substantial advancements in HIV management, rare long-term complications, such as those presented in our study, continue to emerge even in the current era of ART. Factors that complicate the treatment of individuals with HIV include poor adherence to therapy, adverse treatment effects, and insufficiently addressed motivation by healthcare providers. These challenges often lead to costly health problems and reduced quality of life for people living with HIV, particularly when non-adherence persists. 24
It would be interesting for future studies, particularly in developing countries, to promote and evaluate quality improvement proposals to reduce non-compliance in people living with HIV and thus try to improve adherence. Such efforts could play a pivotal role in improving treatment adherence and, consequently, enhancing patient outcomes.
The limitations of our study include its retrospective design and small sample size. Furthermore, the absence of a control group comprising patients who did not undergo splenectomy prevented us from identifying additional parameters associated with the need for this procedure.
Conclusion
The lack of adherence to ART predisposes people living with HIV to an increased risk of complications, including splenomegaly. The cornerstone of treatment should initially focus on adherence to ART and addressing the underlying cause. However, when the condition is refractory or symptomatic, splenectomy may be indicated, although the timing of splenectomy is crucial.
Footnotes
Authors’ Contributions
P.G.-d.S.R.: Conceptualization, methodology, data curation, writing—original draft preparation, and writing—reviewing and editing. O.M.D.-C.: Methodology, data curation, investigation, and writing—original draft preparation. J.C.V.-M.: Conceptualization and supervision. R.S.V.-B.: Supervision and conceptualization.
Data Availability
The data underlying this article will be shared at a reasonable request by the corresponding author.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
No funding was provided.