
Abstract
Background:
Anterior cervical discectomy and fusion (ACDF) is a common spinal procedure with a low complication rate. Although dysphagia and recurrent laryngeal nerve paralysis are well-documented, deep surgical site infections (SSIs) are rare (0.03%–0.3%). This report presents a rare case of deep SSI with an epidural abscess post-ACDF and analyzes the incidence of SSI in Sweden using Swespine data.
Case Presentation:
A 55-year-old female developed cervicothoracic pain and bilateral arm pain three weeks after C6/7 ACDF. Imaging confirmed deep SSI with an epidural abscess. Despite antibiotic agents, reoperation was required 37 days post-operatively, involving C7 corpectomy and titanium reconstruction. Cultures identified oral flora, suggesting hematogenous spread from untreated dental caries. Swespine data showed a 0.05% incidence of deep SSI among 9,382 cases.
Conclusions:
Deep SSI following ACDF is an exceptionally rare but serious complication. Cervicothoracic pain may indicate SSI, and pre-operative dental care is advisable to reduce infection risk.
Introduction
Anterior cervical discectomy and fusion (ACDF) is one of the most frequently performed spinal procedures, 1 offering surgeons a versatile approach to address various cervical spine conditions with a relatively low incidence of substantial complications. 2 Among procedure-related adverse events, dysphagia and recurrent laryngeal nerve paralysis are relatively well-known, with reported incidence rates of 5%–21.3%1,3,4 and 0.9%–3.1%,1,5,6 respectively. However, the occurrence of surgical site infections (SSIs) has been rarely reported, with past studies indicating an incidence of only 0.03%–0.3%.7,8 In this case report, we present a rare case of deep SSI occurring one month following cervical ACDF. Additionally, we report the actual incidence rate of SSI after cervical ACDF in Sweden using national data from the Swedish spine register (Swespine).
Case Description
The patient is a 55-year-old female who underwent C6/7 ACDF as treatment for disc herniation with symptoms of radiculopathy, at another hospital. She experienced substantial improvement in pre-operative symptoms, encountered no major adverse events during or after operation, and was discharged the day following the procedure. Three weeks after the operation, she gradually developed neck pain in the cervicothoracic junction and radiating pain to both arms in the C6 dermatome. One week after symptom onset, she visited the emergency department with increasing symptoms of pain. Her body temperature was 38.1°C, but other vital signs were normal. She reported bilateral proximal upper extremity weakness and posterior neck pain, although physical examination showed no muscle weakness, suggesting pain inhibition rather than neural compression to be the cause of the subjective weakness. No signs of infection were noted at the surgical site (Fig. 1A). Computed tomography revealed air on the left side of the C6/7 intervertebral disc (Fig. 1B, C). T1-weighted magnetic resonance imaging (MRI) showed no substantial abnormalities, but Gd-enhanced MRI revealed contrast enhancement extending from C6/7 to the anterior spinal cord at C2 (Fig. 1D–F). Blood tests showed elevated white blood cell (WBC) (10.0 × 109/L), C-reactive protein (CRP) (130 mg/L), platelets (461 × 109/L), and low serum albumin (33 g/L). The patient had no history of diabetes mellitus, but had been treated with oral Cloxacillin (1,500 mg/d) for lumbar septic facet arthritis six months prior. On the basis of imaging and blood tests, she received a diagnosis of deep SSI with epidural abscess and was admitted for treatment. Cefotaxime (6 g/d) was initiated, and surgical intervention was planned. Four days later, she was transferred to our hospital, where the operation was performed 37 days post-initial operation.
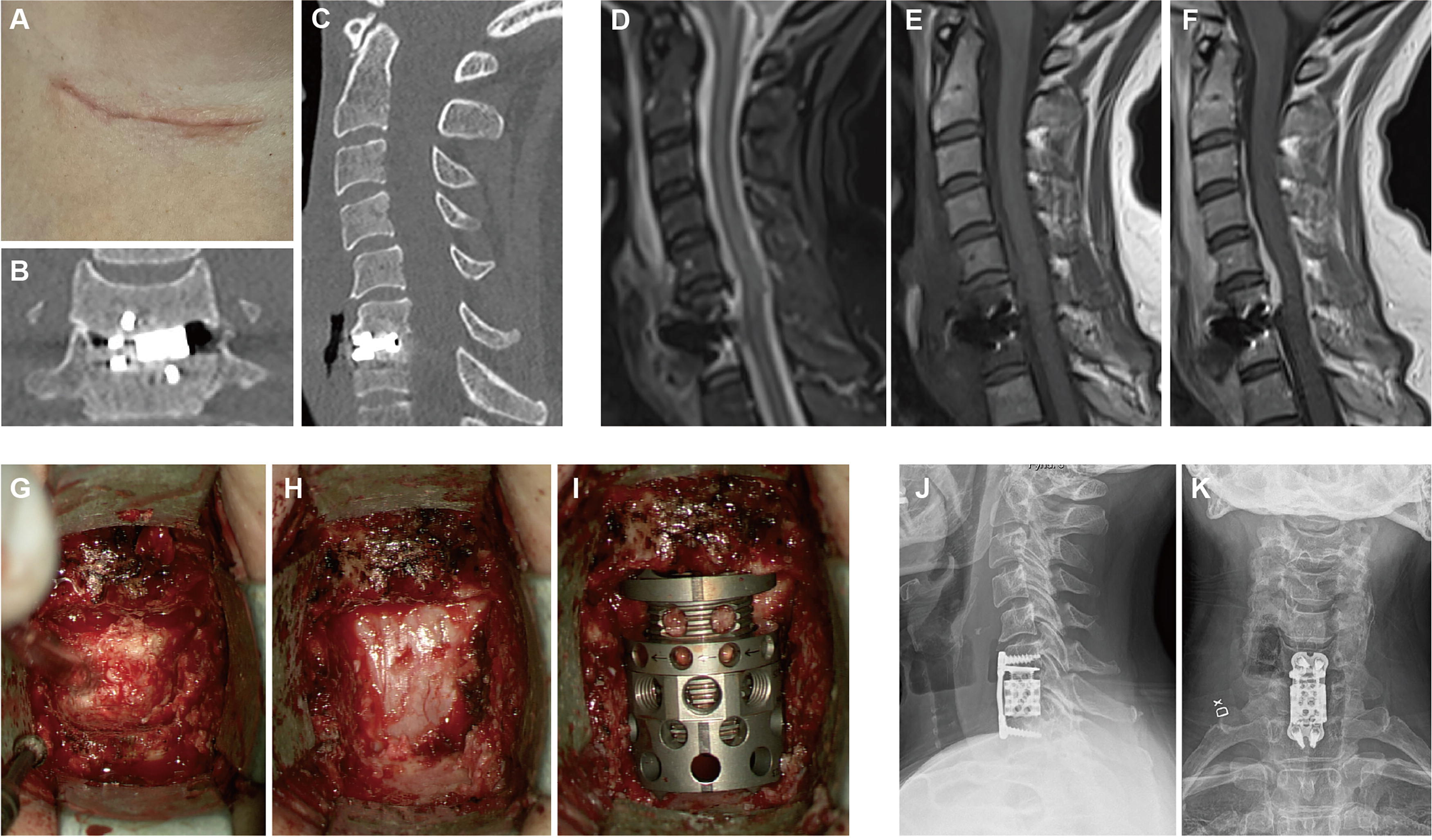
The operation was approached using the transverse skin incision in the right cervical region from the initial operation. No obvious abscess or similar findings were observed until reaching the anterior aspect of the C6/7 vertebral body. After removing the previously inserted cage, a brown abscess was detected within the spinal canal. Five tissue samples and polymerase chain reaction amplification of the 16S rRNA were collected. The C7 vertebral body had become substantially softened because of infection, making cage placement challenging in its existing state. As a result, all softened bone tissues were meticulously curetted, and a corpectomy was performed. Similarly, the portion of the C6 vertebral body in contact with the cage was slightly softened and required some curettage. However, the largest part of the C6 inferior end plate remained solid and was therefore preserved. An expandable titanium cage (anterior destruction device, Ulrich GmbH & Co. KG, Ulm, Germany) and a plate (Skyline cervical system, DePuy Synthes, Raynham, MA) were placed from C6 to T1 (Fig. 1G–K). The result of cultural examination revealed the presence of Streptococcus anginosus, Streptococcus mitis, Candida albicans, anaerobic mixed flora, and mouth flora. Subsequent investigations revealed the presence of untreated dental caries, suggesting that the SSI in this case was caused by hematogenous spread from untreated dental caries.
Post-operatively, neck pain improved substantially (Numeric Rating Scale for neck pain ranging from 1 to 10 points with 10 representing maximum pain, 9 decreased from 9 to 1 point). The post-operative antibiotic agents and the transition of WBC and CRP are shown in Figure 2. The patient was discharged to the referring hospital on post-operative day two. Although CRP concentrations decreased, swelling and pain at the surgical site on post-operative day nine indicated SSI, requiring irrigation and drainage. Persistent infection led to re-transfer, and wound irrigation was repeated on post-operative day 19 with findings of superficial SSI; no implant revision was necessary. Cultures showed Staphylococcus epidermidis and Cutibacterium acnes. After antibiotic therapy, inflammatory markers normalized. The patient continued oral antibiotic agents for SSI and dental caries for three months and has been monitored on an outpatient basis.
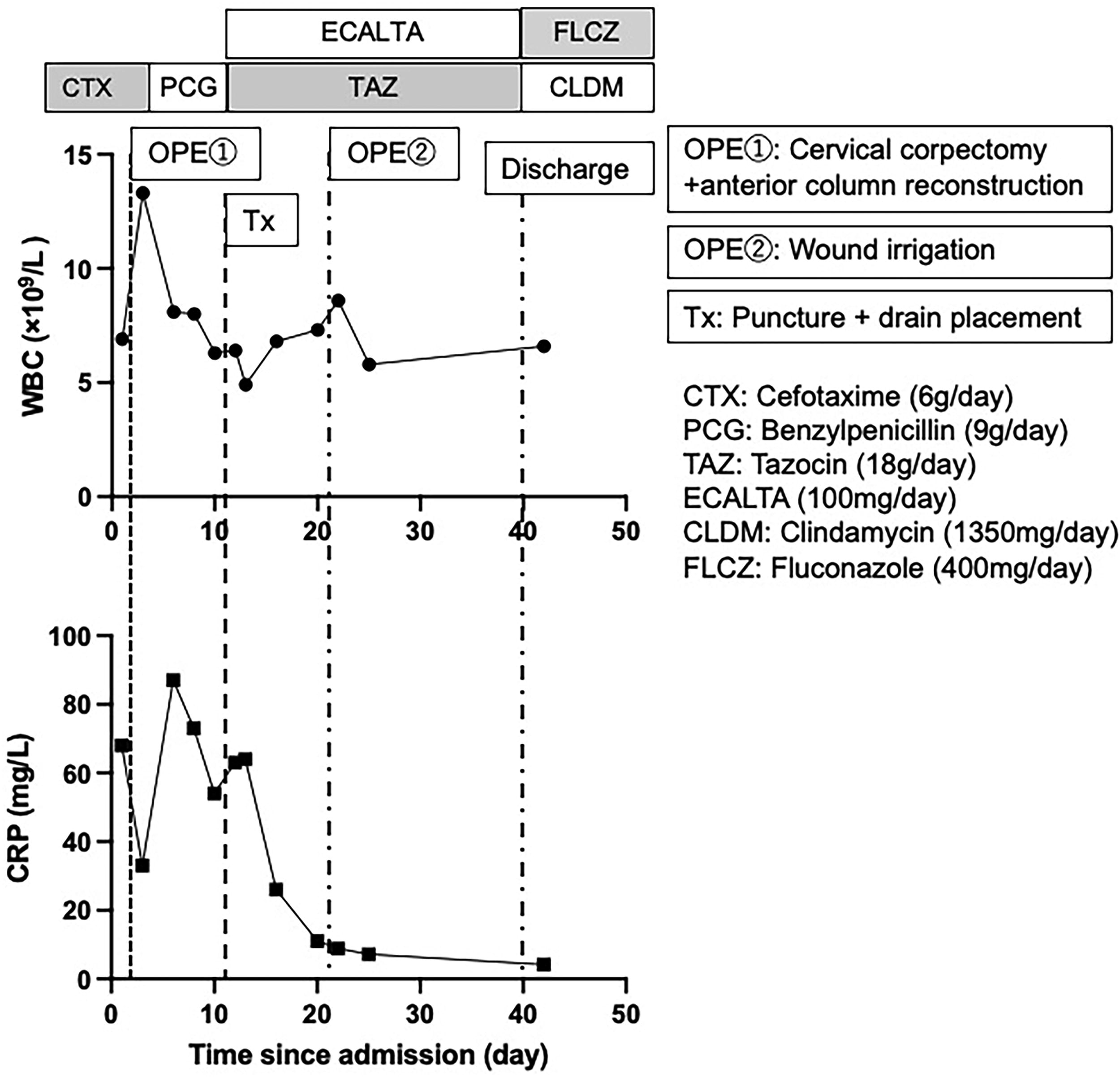
Trend of WBC (white blood cells) and CRP (C-reactive protein) concentrations from admission. OPE = operation; Tx = treatment.
The incidence of SSI following ACDF in Sweden
We investigated the incidence of SSI following ACDF in Sweden using the national Swespine register. Swespine was founded in 1998, and cervical spine procedures have been included since 2006. Approximately 80% of all spine surgical procedures in Sweden are registered. We analyzed the rate of surgically treated SSI following ACDF operation for cervical degenerative diseases in the Swespine registry, including cases with and without the use of a plate. On the basis of the analysis, a total of 9,382 patients underwent ACDF operation. Among them, 17 patients (0.18%) developed superficial SSI, whereas deep SSI was identified in five patients (0.05%).
Discussion
Deep SSI following ACDF is rare, with this study reporting an incidence of 0.05% in Sweden. Similarly, Ghobrial et al. found an incidence of 0.07% in a retrospective multicenter study of 8,887 patients, with all cases requiring revision surgical procedure. 9 Bertalanffy et al. identified an anterior cervical epidural abscess in 0.2% of 450 cases following anterior cervical discectomy without fusion. 10 Our case also involved an epidural abscess requiring revision operation, aligning with previous reports. Notably, delayed SSIs after ACDF have been reported, occurring up to 20 years post-operatively. 11
Despite the presence of SSI following ACDF, our patient exhibited only mild muscle weakness and severe neck pain at the cervicothoracic junction, without anterior cervical symptoms. Although post-operative infections often arise at the surgical site, rare cases of infections spreading via the epidural plexus or vertebral bone have been documented.12,13 The neck pain in our case was likely caused by the epidural abscess, as reported in other cases where neck pain was the primary symptom. 14 In patients presenting with posterior neck pain after ACDF, epidural abscess should be considered.
Risk factors for SSI following ACDF remain unclear because of its low incidence. General risk factors for spinal operations include diabetes mellitus, obesity, prolonged surgical duration, and blood transfusion. 15 In this case, the infection was likely caused by hematogenous spread from dental caries, a pathogen not previously reported in ACDF infections. However, studies highlight the importance of pre-operative oral care in preventing SSI in orthopedic operations. 16 A case-control study identified dental abscesses as potential sources of prosthesis infections in 2.9% of cases. 17 Although bacteria from dental caries are not typical in ACDF infections, this emphasizes the potential value of pre-operative oral hygiene measures, similar to those recommended for arthroplasty.
Infected disc treatment typically involves debridement and fixation combined with an antibiotic agent. 18 Although autologous bone has traditionally been used for anterior reconstruction, its greater rate of subsidence compared with metallic cages has been noted. 19 Titanium cages have been reported to provide post-operative stability and are associated with a low recurrence rate of infection. 20 Despite concerns about bacterial adhesion to implants, titanium cages provide strong post-operative stability and a low recurrence rate, even in osteoporotic conditions, because of the robust immune response in highly vascularized vertebral bone. 21 In this case, anterior reconstruction with a titanium cage and plate achieved excellent outcomes.
Conclusion
Deep SSIs following ACDF are rare but clinically significant complications that require prompt diagnosis and management. The results of this study revealed a low incidence of deep SSI following ACDF in Sweden (0.05%), consistent with previously reported data. This case highlights the importance of considering epidural abscess as a potential cause of atypical symptoms, such as severe neck pain in the cervicothoracic junction, even in the absence of anterior cervical symptoms. Furthermore, it suggests the potential significance of pre-operative oral examination and treatment in patients undergoing ACDF.
Data Availability
The datasets used and/or analyzed in this study are available from the corresponding author upon reasonable request.
Footnotes
Authors’ Contributions
Conception and design: R.F. Acquisition of data: R.F. and I.G. Interpretation of data: R.F., I.G., and P.V. Study supervision: A.M. and P.G. Drafting of the article: R.F. Critical revision of the article: R.F., I.G., P.V., K.I., P.G., and A.M. The final version of the article has been approved by all authors.
Informed Consent
Informed consent was obtained from the patient for the publication of this case report and accompanying images. All the procedures were conducted in accordance with the Declaration of Helsinki (1964).
Ethical Approval
This study was approved by the Swedish Ethics Review Board, January 31st, 2024 (Referens: 2023-07573-01).
Author Disclosure Statement
The authors declare that there are no relevant conflicts of interest.
Funding Information
This research received no specific grants from any funding agency in the public, commercial, or not-for-profit sectors.